 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Middle East Fertility Society Journal, Vol. 9, No. 3, 2004, pp. 215-219 Serum β-hCG level: can it discriminate between unruptured and ruptured tubal ectopic pregnancies? Selcuk Arslan, M.D.* ,Gorkem Tuncay, M.D.†,Hakan Aytan, M.D.†,Omer Lutfi Tapisiz, M.D.† Dr. Zekai Tahir Burak Woman Health Education and ResearchHospital, Ankara, Turkey * Specialist at Reproductive Endocrinology Department Corresponding author: Gorkem TUNCAY MD, Bulbulderesi Cad. 48/ 8 06660 Kucukesat, Ankara, Turkey. Phone: +90 312 4179745, Fax: + 90 0 326 2149632, E-Mail: drgorkem@ hotmail.com Received on March 30, 2004; Code Number: mf04040 ABSTRACT Objective: To evaluate the predictive value of
serum βhCG levels in discrimination of intact tubal pregnancies
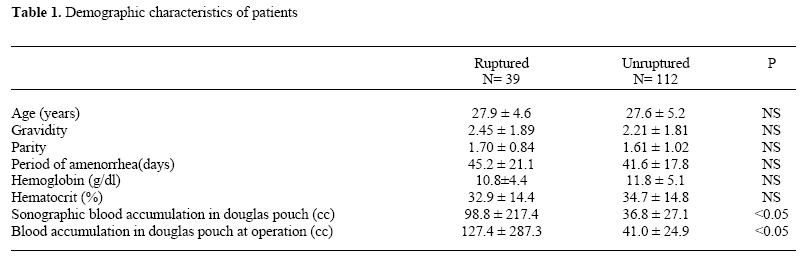
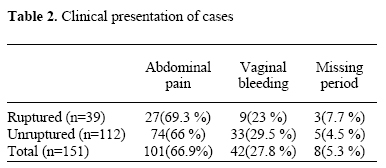
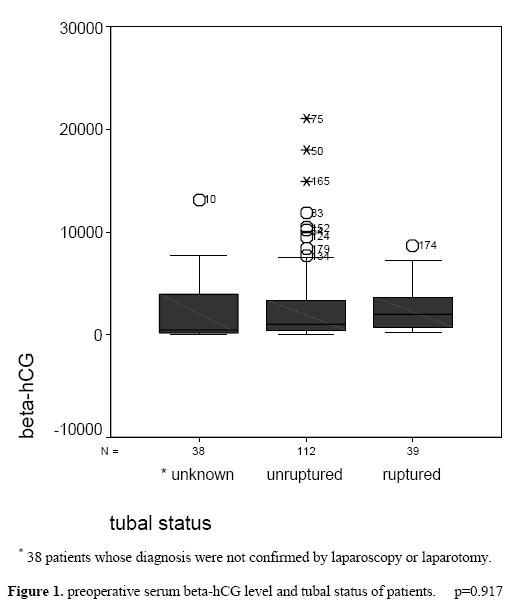
from ruptured tubal pregnancies. Key words: Ectopic pregnancy, preoperative serum βhCG level, tubal integrity. There has been a marked increase in both the absolute number and the rate of ectopic pregnancies in the past two decades. The reasons for this increase are not entirely clear. Increased prevalence of sexually transmitted tubal infection (1,2), earlier diagnosis with sensitive assays for chorionic gonadotropin and transvaginal ultrasound - in some, resorption would occur before diagnosis in the past, popularity of contraception that prevents intrauterine, but not extrauterine pregnancies, unsuccessful tubal sterilizations, induced abortion followed by infection, increased use of assisted reproductive techniques, and tubal surgery are implicated factors (3). However, the most promising development is the significant decrease in mortality due to improved diagnostic and therapeutic modalities. The success of methotrexate therapy resulted in a shift from even minimal invasive surgical interventions such as laparoscopy, towards preference of medical alternatives. Herein the non-invasive diagnostic work-up of patients admitted to clinics gain importance. Ultrasonographic evaluation of the patients in experienced hands may be very beneficial in this era; however, the significance of serum βhCG levels - which can identify women with a high probability of ectopic pregnancy (4) - used for confirmation of ultrasonography in predicting the tubal status still remains to be explained. In this study we tried to determine whether βhCG levels measured at admission in the emergency unit is a good parameter for prediction of tubal status. MATERIAL AND METHODS A prospective study was conducted between September 1998 and December 2001 at Dr Zekai Tahir Burak Women's Health Education and Research Hospital Emergency Unit. 151 of the 189 patients admitted with the diagnosis of ectopic tubal pregnancy that was confirmed by laparoscopy and or laparatomy were enrolled. Remaining 38 patients who took medical or expectant management were excluded and accepted as patients with unknown tubal status. Detailed medical and obstetrical history was obtained and physical / pelvic examination was performed to each patient. Preoperative diagnostic investigations, serum βhCG, hemoglobin and hematocrit levels, transvaginal ultrasonographic evaluation notes were recorded. Intra-operative findings -tubal rupture, abortus and or intact tubes- were noted. SPSS 10.0 version was used for statistical analysis. RESULTS Laparoscopy and or laparatomy confirmed tubal pregnancy in 151 of the 189 patients. In 39 cases the tubes were ruptured and in the remaining 112 cases the tubes were found to be intact. There was no statistically significant difference between mean ages, (27.9 ± 4.6 and 27.6 ± 5.2 years in ruptured and intact groups respectively) complaints at admittance, physical examination findings, and the number of previous pregnancies. The demographic characteristics of the patients are depicted in Table I. Also a crosstabulation for period of amenorrhea, hemoglobin- hematocrit levels and blood accumulation in douglas pouch sonographically and peroperative given in Table I. Only a statistical difference was observed in ultrasonographic and peroperative evaluation of blood in douglas while there were no statistical differences of other demographic data. The dominant complain was abdominal pain in both groups. Vaginal bleeding and missing period were the following complains in both groups. Clinical presentation of cases displayed on Table II. The mean serum βhCG levels measured from blood drawn during admission was 2560.08 ± 2116.9 mIU/ml in the ruptured and 2763.83 ± 3732.2 mIU/ml in the intact groups respectively. There was a positive correlation between preoperative ultrasonographic dimensions of gestational sacs and the serum βhCG levels. The mean diameter of gestational sacs was found to be 44.1 SEM 3.1 mm in the ruptured group, whereas it was 32.8 SEM 1.7 mm in the intact group (p=0.0001). No tubal rupture was observed with a gestational sac of less than 30 mm. However, no significant correlation was found between serum βhCG levels and the tubal status (p=0.917). (Figure 1) DISCUSSION HCG is secreted by syncytiotrophoblasts and levels approximately double every 2 days in early, normal intrauterine pregnancies, and a lower increase is associated with ectopic pregnancies and spontaneous miscarriages (5). However some ectopic pregnancies, at least for a while, display a normal rise in titer as syncytiotrophoblasts multiply as in normal intrauterine pregnancies. With advancing gestational age syncytiotrophoblasts begin to invade vessel lumens causing bleeding and hematoma formation and because their viabilities are affected throughout this process, the expected linear increase in serum βhCG levels cannot be observed. Ultrasonography as the first step is the most efficient and accurate method of diagnosing ectopic pregnancies and algorithms using a combination of ultrasonography and β-hCG result in the best outcomes (6). As well as the diagnosis of ectopic pregnancy the assessment of the tubal status is also of vital importance and most of the time this would beimpossible with non-invasive techniques. In our series we showed that ultrasonographically measured dimensions of ectopic pregnancies, and gestational ages calculated by last menstrual period have a positive correlation with tubal status (tubal rupture, abortus or intact tubes) (p=0.001). Mol and colleagues showed that risk of tubal rupture and or active bleeding is increased when gestational age is ≥ 7 weeks, ectopic mass is ≥24 mm and serum βhCG levels are ≥ 1300 IU/L (7). This study points out statistical difference between blood accumulation on sonographic screen and per operative procedure among groups. It probably originates from sonographic validity on estimating fluid in the pouch of Douglas. Abdominal pain has a high sensitivity in the diagnosis of ectopic pregnancy; present in 157 of the 189 cases (93.5%). However, it was not so beneficial in discrimination of intact tubes from ruptured ones. In the same report Mol and colleagues showed that presence of abdominal pain and fluid accumulation in the cul-de-sac increases the possibility of tubal rupture in 19% and 13% respectively (7). In most of the published reports in literature there is a general consensus on the point that when gestational age is > 10 weeks and serum βhCG levels > 8500 IU/L, the probability of predicting risk of tubal rupture or active bleeding is over 10 %. Nevertheless we have to clarify that ectopic tubal pregnancies resulted from infertility treatments; such as in vitro fertilization programs should be taken carefully and followed as early as possible with a reliable diagnosis and management manner could be achieved with vaginal sonography and βhCG estimation. In this study it was not always possible to decide on the appropriate management approach, medical or surgical, just by clinical evaluation of the patients that were hemodynamically stable. Ackerman and colleagues (8) found a positive correlation between serum βhCG levels and tubal rupture like Job-Spira et al who in their report (9) suggested that a high level of βhCG (at least 10000 IU/L) when ectopic pregnancy was suspected increases the risk of rupture (OR 2.9[1.5 to 5.6]). However, in contrast Roussos et al, similar to our findings, reported that serum βhCG level does not predict tubal rupture (10). In our study serum βhCG levels were only associated with the dimensions of the tubal pregnancy (p=0.002). Evaluation of tubal integrity is very important before deciding on conservative management of tubal ectopic pregnancy. We ascertained that serum βhCG levels are not helpful in this evaluation. The mean dimensions of tubal ectopic pregnancies in ruptured and un-ruptured cases are found to be different with a statistical significance (p=0.001). For this reason, ultrasonographic evaluation seems to be a better parameter for determination of appropriate management protocol in tubal ectopic pregnancy. REFERENCES
Copyright © Middle East Fertility Society |

{kind=link}
{kind=link}
{kind=link}