 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Middle East Fertility Society Journal, Vol. 9, No. 3, 2004, pp. 220-226 A prospective comparative study between 3D ultrasonography and traditional 2D ultrasonographic assessment of ovarian tumours Dalia Youssef, M.D.,Mona Aboulghar, M.D.,Khaled Abdel Malek, M.D.,Ahmad El-Halwagy, M.D.,Bahaa El-Din Hammad, M.D.,Essam Aboul Foutouh, M.D. Department of Obstetrics & Gynecology, CairoUniversity, Cairo, Egypt Contact address: Mona Aboulghar, M.D. E-mail: ivf@link.net Received on April 26, 2004; Code Number: mf04041 ABSTRACT Objective: to evaluate the value of 3D ultrasonographic examination
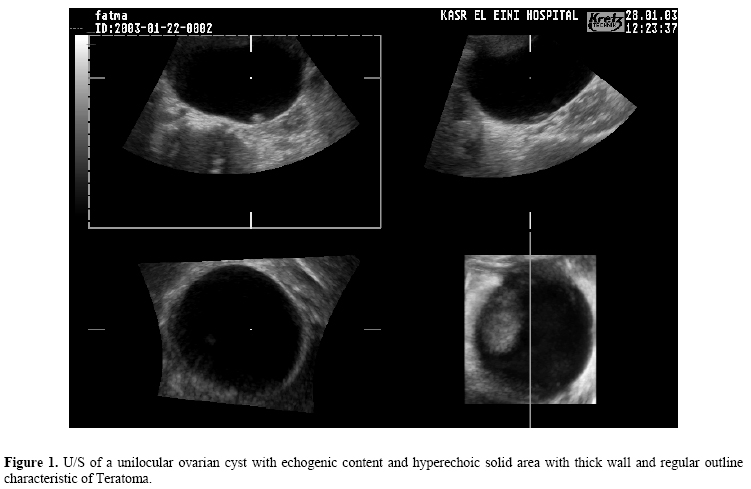
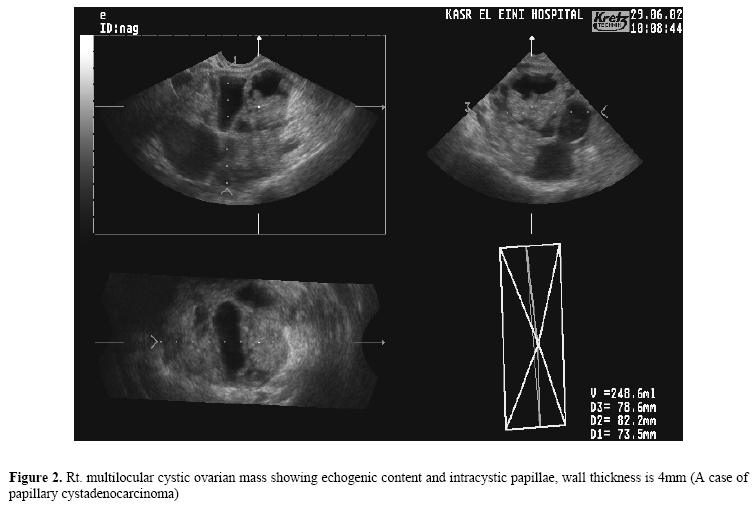
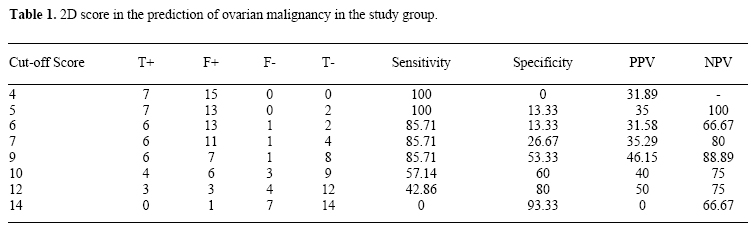
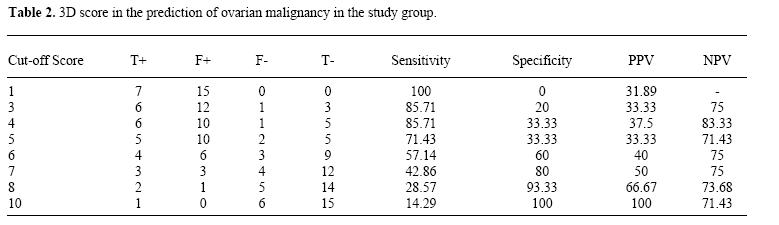
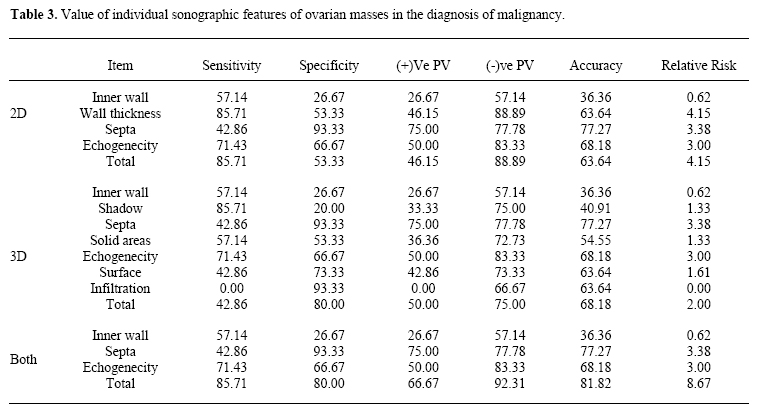
of adnexal masses compared to 2-dimensional ultrasound. Keywords: 2D ultrasonography, 3D ultrasonography, ovarian cancer, tumors Several studies indicated that two dimensional sonography screening for ovarian malignancy has a positive predictive value of only 10% in post-menopausal women (1, 2). As a result, there has been increased interest in the evaluation of several adjunctive diagnostic methods as a mean to increase the specificity and positive predictive value of ultrasonography screening (3). Three dimensional ultrasound represents a new technique of imaging owing to its ability to register all three imaging planes simultaneously; to reconstruct new planes which are otherwise not visible as well as to visualize surfaces three-dimensionally (4). Although surgery for an ovarian mass is currently the inevitable outcome, prior knowledge of the odds for malignancy can guide such aspects as timing, extent and availability of frozen section pathology, not to mention patient counseling. Exact knowledge of the mass size, surface and relation to surroundings may select cases for laparoscopic surgery. The aim of this study is to explore the diagnostic value of 3D ultrasonographic examination of ovarian masses in terms of accurate detection as compared with two-dimensional ultrasound. MATERIALS AND METHODS A prospective study was conducted at the Obstetrics and Gynecology Department of El Kasr El Aini-Hospital - CairoUniversity in the period between September 2002 and May 2003 after approval of the local ethical committee. Patients with postmenopausal bleeding were subjected to complete clinical examination, 2-D and 3-D ultrasonographic evaluation. Then the findings were compared to histopathological examination of tissue specimens after laparotomy. Ultrasonographic evaluation was done using Voluson 530D (Medison; Kertz apparatus); through transvaginal route (using 6.5 MHz intracavitry probe). A 3D image was built by selecting a region of interest from a 2D image and superimposing on it a volume box defined by the examiner. The crystal array of the transducer sweep mechanically over the 2D region selected through a 60° angle. Within 5 s, the outlined volume is automatically scanned and a sculpture-like 3D image is displayed simultaneously on the screen. In this system (Vol-mode), the ultrasound beam is regarded as a projection ray in volume rendering, and ray tracing was conducted in real time. The procedure was not as complex as that of conventional 3D ultrasonography, and images could be obtained immediatelyAdnexal masses were described according to their site (Right, Left or bilateral), size, nature (solid, cystic or heterogeneous), echogenicity, wall thickness, wall for the presence of irrigations and septae. The scoring system described by Sassone et al., (1991) for the prediction of malignant lesions was applied. A score of 9 is used as the threshold for distinguishing benign from malignant masses (5). Ovarian lesions were evaluated for the same items as 2-D. The score described by Kurjak et al. for the prediction of ovarian malignancy by 3-D was applied (6); which includes, in addition to items, previously examined by 2-D,shadowing, surface irregularity and relation to surroundings. Doppler-based assessment was not preformed. The total score is the sum of individual scores. The cutoff score >7 is associated with high risk for ovarian malignancy. In our study; Score 6 was taken equivalent to score >7 (7.8) when adjusted since the used score (13 points) (excluding the Doppler points) is expected to be less than the actual score including Doppler based assessments (17 points). The different 3-D modes are dedicated to detect various items in the above scoring systems. For example; "the surface reconstruction" allows the study of inner and outer wall surfaces of tumor. This capacity makes it possible to study tumor echogenicity; papillary projections; septa and small irregularities of the tumor wall;. Other modes like "transparent maximal minimum" mode revealed intratumoral objects with high echogenicity such as areas of calcification or bones in dermoid tumors. The reliability of the 3D volume data was assessed by the authors who were all experienced in pelvic ultrasonography. They independently analyzed all the stored scans and were unaware of each other's results. The results of 2-D and 3-D U/S findings were compared to each other and to the final diagnosis which was made after laparotomy and pathological examination of the lesion. Statistical analysis Data were tabulated and presented in terms of range; mean; standard deviation (+SD) and percentages. All statistical calculations were done using computer programs Microsoft Excel version 5 and SPSS (Statistical Package for the Social Science). RESULTS The present study enrolled one hundred postmenopausalwomen presenting with bleeding attending the outpatient clinic and by examination adnexal mass could be detected in 22 of them. Their mean age was 49.7 years ± 8.6 (range 46-76) and parity was 2.58 ± 1.0 (range 1-5). The adnexal masses were bilateral in two cases (9.1%) and unilateral in 20 cases. Concerning the nature, 2 were entirely solid, 15 were cystic and five were heterogeneous. On pathological examination, they were found to be differentiated into malignant lesions (7 cases); benign lesions (13 cases) and non-neoplastic lesions (2 cases), which were PID and endometrioma. Out of the seven malignant cases; five were cystadenocarcinoma. Among the benign lesions, the most common were serous cysts and mature teratomas (4 patients each; 8%) (Figures 1, 2). Considering the optimal cut-off score for malignancy, score 9 provides 85% sensitivity and 53% specificity. Higher scores improve specificity but with an unacceptably low sensitivity. Using a cut-off value of 7 had a fair specificity (80%) but too low sensitivity (43%). Mathematical correction for Doppler points (a cut-off 6) still has a low sensitivity (57%). At a cut-off score of 4, sensitivity rose to 85% but specificity was only 33%. Combining both scores at cut-off points of 9 and 7 for 2D and 3D respectively achieved 85% sensitivity and 80% specificity (Table 1,2). Individual sonographic features had different values of sensitivity and specificity and are shown in Table 3. DISCUSSION Medical ultrasound has during the last decades experienced enormous technological progress, and in obstetrics and gynecology it has become an integral part of the clinical work. Within the last years several new ultrasound techniques have appeared. Three-dimensional ultrasound scanning (3DUS), in which there has been great interest, is one of them. Especially within gynecology several papers on that topic describe promising results. However, until now only few prospective works have been published, most of them counted as preliminary (7). In the present study, wall thickness and septa were satisfactorily assessed by 2D while surface rendering mode of 3D U/S was used to assess wall regularity. Solid areas were found to be 57% sensitive and 53% specific for malignancy. Although the mentioned studies suggest that the lack of a solid component virtually excludes malignancy, the present study found a sensitivity of only 57%. Positive predictive value of solid areas would increase from 3% to 50% if the three patients with shadowing were excluded; agreeing with Brown and colleagues that shadowing coincides with benign nature. The absence of shadowing was the most sensitive sonographic parameter for malignancy in this study (85.7%); albeit with a low specificity (20%). The presence of shadowing therefore virtually excludes malignancy. Thirteen patients (59%) had irregularities on the inner wall surface, of whom 10 patients had papillarities (>3 mm thick). The presence of wall papillarities or predominantly solid lesions, as opposed to smooth walls or fine irregularity (<3 mm) was 57% sensitive and 26.7% specific for malignancy. According to recent literature, (8) thick wall >2 to 3 mm is considered a sign of malignancy but this is less specific because many hemorrhagic cysts and endometriomas also have wall thickening. The results agree with this study since wall thickness of >3 mm was 85.7% sensitive but 53.3% specific.Concerning septa, they were present in 9 patient of whom four had thick septa (>3 mm). Thick septa had 93% specificity and 43% sensitivity for detection of malignancy. This high specificity is in accordance with other researchers (9) who used a scoring system using presence and thickness of septations as one of 3 parameters for diagnosis of malignancy (the other two parameters were central flow and moderate to large amount of intraperitoneal fluid with a sensitivity of a 3% and specificity 93%. Lesions with mixed echogenicity (9 cases) or high echogenicity (one case) were 71.4% sensitive and 66.7% specific for malignancy. The surface of the mass was observed (using surface rendering mode) to be irregular in 7 patients, which gave our sensitivity 42.86 but a very high specificity 93.33 for malignancy. Infiltration of the surrounding structures was also studied by 3D and present in only one case falsely interpreted as malignant which is a case of PID mostly due to extensive adhesions. Among the previously-discussed points, the most sensitive were wall thickness and lack of shadowing (both 85.7%) while the most specific were thick septa >3mm and irregular surface (93%). Regularity was assessed by 3D surface rendering mode while the three other parameters showed no difference in findings between 2D and 3D assessments. Combining these four criteria may combine high sensitivity and specificity. The score suggested by Sassone et al. (5) which is based on 2D findings and suggests a score of 9 as suggestive of malignancies was applied. Ten patients scored above 9 of whom six patients had a (pathologically-proven) benign lesion. Only one patient who scored <9 proved to have a malignant lesion (Mucinous cystadenocarcinoma scoring 5). These data show that a cut-off value of 9 was highly sensitive (85.7%) but poorly specific (53.3%). This study agrees it is the optimal cut-off value. Sassone et al. (5) reported similar findings of high sensitivity and lower specificity but they reported higher values (100% and 83% respectively). A 3D and power Doppler-based score was suggested by Kurjak et al. who suggested 7 as the cut-off value. The score comprised 17 points of which 4 were Doppler-based. Because Doppler was not uniformly used in this study, the maximum score was only 13 points. Score 7 in this case was 43% sensitive and 80% specific, 4 malignancies were missed. A score of 6 would be equivalent to >7 (7.29) if corrected mathematically for the missing Doppler points. Even so, 3 malignancies are still missed with a sensitivity of only 57%. Acceptable sensitivity (85.7%) would be achieved at a cut-off score of four when specificity would be 33%. Although this would suggest the lack of an additional role of 3D, two points need to be considered: First, the Doppler assessment and second, raising 3D cut-off score enhances specificity (albeit at the expense of sensitivity) and if used in conjunction with 2D assessment would raise the specificity at 85%, sensitivity to 80%, far better than either alone. This agrees with other investigators (10) who studied 8 patients and found that although the morphological score did not differ between 2 and 3D U/S for benign cysts, one additional malignancy was diagnosed by 3D, which had been missed by 2D. 4 other malignancies were diagnosed by 2D and 3D. They concluded the ability of 3D U/S technology to enhance the morphologic scoring system and further improve the ability to differentiate benign from malignant ovarian masses.3D assessment is reported to be more informative regarding papillary projection, characteristics of cyst walls and extent of capsular infiltration (11). In the currents study results indicate that the presence of irregular surface by 3D was highly specific for malignancy and wall thickness <3mm was virtually exclusive. However, we could not demonstrate increased accuracy of 3D in the detection of papillae >3mm thick. We also had apparent infiltration in one case of an inflammatory mass, PID. The score of Sassone et al. (5) for diagnosis of ovarian malignancy based on 2D U/S had 85.7% sensitivity at a cut-off value of 9. It is highly sensitive but some malignancies can still score <9. Specificity is lower and in this study it was even lower than that reported by Sasssone et al (53%). Combining 2D and 3D assessments achieved a higher accuracy than either alone; with reasonable sensitivity and specificity. In conclusion, 3D U/S is potentially helpful in the diagnosis of ovarian masses. It could be used to supplement 2D assessment and further large-scale studies are needed to refine and test the scores used to differentiate benign from malignant lesions. REFERENCES
Copyright © Middle East Fertility Society The following images related to this document are available:Photo images[mf04041t3.jpg] [mf04041f1.jpg] [mf04041t2.jpg] [mf04041t1.jpg] [mf04041f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}