 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Middle East Fertility Society Journal, Vol. 9, No. 3, 2004, pp. 227-231 Can serum prostate-specific antigen be a promising marker for patients with polycystic ovary syndrome and hirsutism Ansam A.Al Bayatti, Ph.D. *,Summer H. Al-Samak, F.I.M.C., Ob.Gyn. †,Awatif J. Al Bahar, F.A.H.K.A.R.Z.T. ‡ Department of Biochemistry, College of Medicine, University of Baghdad; Al- Elwyia Teaching Hospital -Al-Kindy Collage of Medicine, University of Baghdad, Baghdad, Iraq and Al Wasal-Hospital, Dubai, AUE *Dept. of Biochemistry, College of Medicine, University of Baghdad Correspondence: Assist. prof. Dr. Ansam Al-Bayatti, Dept. of Biochemistry, Collage of medicine, University of Baghdad, E-mail: ansimalaad@Yahoo.com, Tel: +964 17722065, 7901331923 Received on April 26, 2004; Code Number: mf04042 ABSTRACT Background: Total prostatic specific antigen (TPSA) is a glycoprotein
that is secreted from the prostate in males and from paraurethal glands and
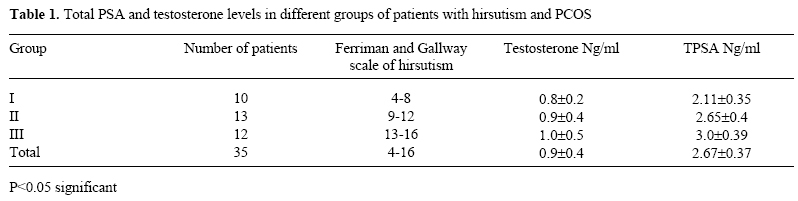
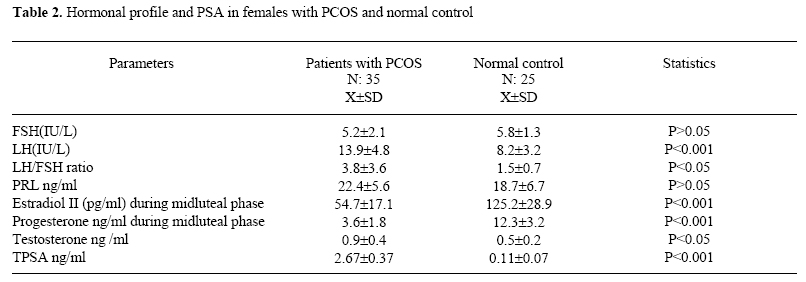
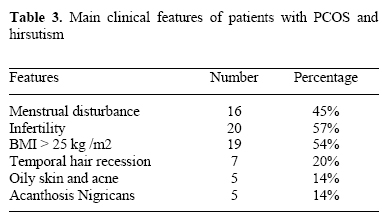
breast in females. Keywords: PCOS, TPSA, hirsutism, ELFA Prostate specific antigen PSA was thought to be produced from prostate gland in male, however non prostatic PSA had been found in many normal female tissues particularly breast tissue, parotid glands, endometrial tissue and periurethral glands (1,2), by the fact that these glands in females are highly homologous to male prostate (3). In healthy women PSA is present in very low concentration and its level vary during menstrual cycle Zarghami et al (4) speculated that corpus luteum steroids stimulate target tissues capable of producing PSA one of which is the breast for PSA production into the mammary ducts. A fraction of this PSA diffuses into general circulation and can be measured in the serum. Peak concentration after 10-12 days after Progesterone peak, once corpus regress PSA conc. Decreases with an apparent half life of 3-5 days, measurement of PSA in this study by PCR complicated technique. PSA level is detectable in women serum with excess androgen and do not change during treatment with contraceptive pill as mentioned by Escobar-Morreale H. et al (5) who used ultra sensitive chemoluminescent immunoassay. PSA in female is a potential marker of androgen excess, however the adrenal gland and the ovary do not appear to be source of PSA (7). Polycystic ovary syndrome PCOS is a disorder characterized by hyperandrogenism and chronic anovulation as well as features were documented by ultrasound examination (6,7). Serum PSA in normal women are very low while in those who have PCOS with hyper androgenic features, PSA level is elevated but not always detected by using ultra sensitive method time-resolved fluorometeric immunoassay with established lower detection limit one ng/ml (8). Urinary PSA was markedly elevated in PCOS using the above mentioned method (9). Our aim to use highly sensitive method to detect serum PSA in normal and PCOS patients in order to shade a light on the normal range of PSA in females. MATERIALS AND METHODS Thirty five females with features of PCOS and hirsutism that were proven clinically and by abdominal sonar and were attending AL-Elwyia Teaching Hospital from the period of September 2003 till March 2004. Twenty five apparently healthy fertile females matching the studied group in age and served as control were included in this study clinical examination of those patients to asses the score of hirsutism depending on the Ferriman and Gallway scale, in this approach, hair growth was judged in each of 11 androgen -sensitive areas, the grade for each area ranged from zero (non terminal hair) to 4 (frankly virile). The body areas used to grade hirsutism areas 1. upper lip, 2. chin, 3. chest, 4. leg, 5. thigh, 6. upper arm, 7. forearm, 8. upper back, 10. upper abdomen and 11. lower abdomen (10). Blood samples were aspirated during second -third day of menstrual cycle, to asses Follitropin (FSH), Lutropin (LH), Prolactin (Prl), Testosterone (testo) and Total Prostate-Specific Antigen (TPSA). Another blood samples were aspirated during midluteal phase to asses Progesterone (Prog) and Estradiol II (E2) levels. All these parameters were measured by highly sensitive Enzyme Linked Fluorescent Assay ELFA with established lower detection limit 0.07 ng/ml for TPSA. Patients with amenorrhea were excluded from this study body weight and height were measured in all patients to calculate Body Mass Index BMI(kg/m2). Data processing and analysis The collected data were entered and processed using statistical package for social science (SPSS). RESULTS Thirty five patients with PCOS and hirsutism were classified according to the Ferriman and Gallway scale of hirsutism, all females with score less than 4 and more than 16 were excluded from this study. They were divided into three groups depending on hirsutism score, their Testo. levels were more or less similar in the three groups while TPSA was significantly higher (P< 0.05) in group II and group III who had higher hirsutism score as in Table (1).it was noticed that the more the score of hirsutism the higher serum TPSA. The hormonal profile of the studied groups showed significantly high LH; LH/FSH ratio, Testo, and TPSA while midluteal serum P. and E2 were significantly low in comparison with control Table (2). There was no correlation between Testo. level and TPSA in patients with PCOS of hirsutism (r:0.7 P:0.1). Those patients had different presenting signs of symptoms as follow, infertility 57%, obesity 54% and menstrual disturbance 45%, however these are other features were documented Table(3). DISCUSSION PSA can no longer be regarded as a tissue specific or tumor-specific marker for only prostatic tissue but as ubiquitous molecule that can be synthesized and secreted by cell bearing specific hormones receptors under conditions of steroidal modulation or stimulation (12). It could be elevated in case of breast cancer in serum nipple aspirate fluid and tissue using time-resolved immunoflurorometric assay (13). PSA could be detected in cerebrospinal fluid (14), human endometrium (15) and human placenta (16). Different studies have already demonstrated that females with hyperandrogenism usually have elevated serum TPSA (11,17). Also other studies have indicated that women treated with testosterone over prolonged period of time, had significantly increased TPSA (11). This study pointed out that the more the score of hirsutism the higher the TPSA level (Table 1), which disagrees with a previous study which found no association between the Ferriman-Gallway score and the level of urinary TPSA (11). This might be attributed to the present study that it was restricted to PCOS with hirsutism and not PCOS in general, while Obiezu CV. et al (11) had measured urinary TPSA rather than serum TPSA that might explain the disagreement. However, there is agreement about poor correlation between Testo and urinary TPSA (11,18) as well as in the present work between Testo and serum TPSA. Recent study pointed that there is no significant association between PSA and the presence of idiopathic hirsutism per se & PCOS were excluded from that study, however they used completely different method micro particle enzyme immunoassay (MEIA), the lower limit of detection of PSA was > than 0.03 ng/ml (19), while in ELFA method that was used in this study with lower limit of detection is >0.07 ng/ml i.e. more sensitive. The interesting finding in this work is to record the mean value of serum TPSA in PCOS 2.67±0.37 ng /ml table (2) that was detected by sensitive method ELFA and the control values 0.11±0.07 ng/ml as well. The hormonal profile was similar to other studies (20,21) i.e. elevated LH/FSH ratio and Testo levels Table (2). Most of studied patients had anovulatory cycle i.e. significantly low E2 values table (3) that was in agreement with different studies (13). The main clinical presenting features of PCOS with hirsutism are more or less similar to other studies (22,23), in spite of different percentage of certain features of the present work. In conclusion serum TPSA can be a promising marker in patients with PCOS and hirsutism in detectable level by using ELFA method that may open new modalities for treatment of this syndrome. REFERENCE
Copyright © Middle East Fertility Society
|

{kind=link}
{kind=link}
{kind=link}