 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
3D power Doppler; a possible new predictor for ovarian hyperstimulation syndrome in PCOS: hormonal correlation* Mohamed Eid, M.D.†‡§ ,Samir Abbas, F.R.C.O.G.†,Amany Tayae, M.Sc.†,Emad Soliman, M.D.†,Amal Shohiab, M.D.†‡ Dr. S. Abbas Medical Center (IVF unit), Jeddah, KSA and Department of Ob. Gyn., CairoUniversity, Cairo, Egypt. * Accepted as poster presentation in the ESHRE meeting (Madrid,
2003), and Oral presentation in MEFS meeting (Beirut, 2003) Received on May 9, 2004; Code Number: mf04043 ABSTRACT Objective: An attempt for prediction of severe OHSS using 3D power
Doppler scan of ovarian stromal blood flow in PCOS patients and correlating
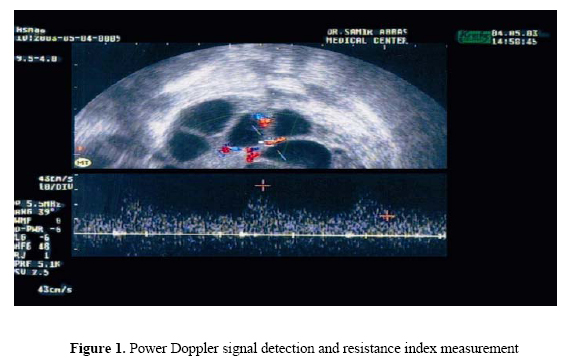
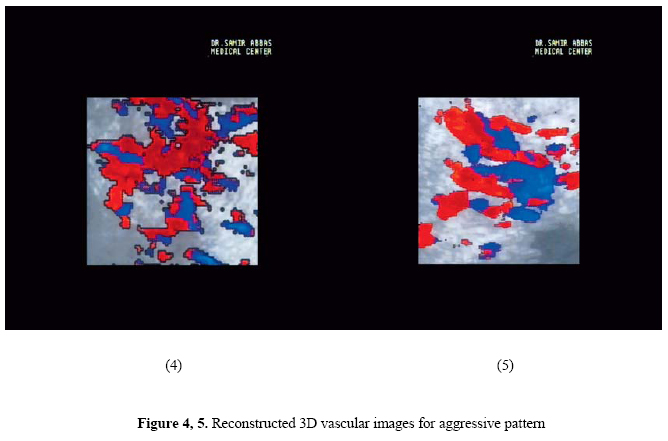
the findings with serum estradiol (E2). Key words: OHSS, PCOS, power Doppler, 3D-US. Ovarian hyperstimulation syndrome (OHSS) is an iatrogenic, serious complication of controlled ovarian hyperstimulation (COH), usually self-limited, but occasionally life-threatening and typically occurs with gonadotrophins, rarely with clomiphene citrate (1). The incidence of OHSS (all forms, mild, moderate & severe) in ART ranges from 0.6 to 14%, while the severe form complicates only 0.2 to 2% of all IVF cycles (2, 3). Several risk factors have been identified in patients prone to develop OHSS, e.g. young age (<35 years), lean habitus and polycystic ovarian syndrome (PCOS) (4). As the pathophysiology of OHSS is still not well understood, so all preventive strategies depend on identifying patients with a high risk profile during COH. Very high estradiol (E2) response(>4000 -6000 pg/ml) and multiple follicular response (>20 follicles) is associated with an 80% chance of developing severe OHSS (5). PCOS is considered the major item in the high risk profile for developing severe OHSS. The stromal blood flow velocities of the ovaries have been studied before by two-dimensional (2D) Doppler ultrasound, but the findings were considered inconclusive, as it was obtained from a subjectively chosen artery lying in a 2D plane that was also subjectively chosen (6). The latest technical achievement in the field of ultrasound is three-dimensional (3D) power Doppler ultrasound, which theoretically provides the possibility of assessing the volume, blood perfusion and vascularization of the whole target organ. So far, this modality has been used in quantifying the power Doppler signal in PCOS (7), to check down-regulation (8), in adnexal masses (9), and in the endometrium (10). The aim of our study was an attempt for prediction of severe OHSS by studying the morphology of the ovarian stromal blood flow using 3D power Doppler ultrasound modality and correlating the findings with the serum E2 level. MATERIALS AND METHODS Patients A total of 22 patients (22-35 years old), except one patient (37 yrs), were included in this prospective-observational study. All had the diagnosis of PCOS based on ultrasound findings of PCO ovaries, menstrual irregularities, clinical evidence either of acne, alopecia or hirsutism and abnormal hormonal values, high testosterone or a LH/FSH ratio >1. Patients were already under gonadotrophins stimulation for IVF or ICSI and their ovarian response was monitored serially by U/S and E2. Serum E2 level was in the range of 3000-7000 pg/ml, except in 3 patients (12 with E2 = 3000-5000 pg/ml, 7 with E2 = >5000-7000 pg/ml and 3 with E2 = 9000-11000 pg/ml). 3D power Doppler examination TV/US examination was done for all patients on day of HCG administration. All examinations were performed by one author (T.A.), who was blind to the serum E2. A conventional 3D power Doppler ultrasound (Voluson 530D, Medison-Kretz, Austria), was used. The scan was done on both ovaries excluding the ovarian vessels. Once the Doppler signal had been detected (Figure. 1), the volume mode was switched on. 3D volume was generated by automatic rotation of the mechanical transducer 360°. The acquisition time was around 10 seconds. During recording, the probe was kept steady and patient asked to lie still on bed. 3D power Doppler imaging "Reconstructed 3D vascular image" was recorded and resistance index (RI) was also measured. RESULTS Two patterns of 3D vascular images were detected (Table 1); each pattern was mostly confined to certain level of serum E2, (pattern I & pattern II). Pattern I "Reassuring pattern" The vascular description was that of regular branches, minimal coils and mild dilatation (Figures 2, 3), associated with (RI) = 0.55-0.61, that of normal well-formed vessels. This pattern was observed in 15 patients (71%), 12 had serum E2 = 3000-5000 pg/ml, and of interest 3 patients had very high E2 (9000-11000 pg/ml). Analysis of history of those exceptional patients, it was found that; one was 37 years old, the second had a BMI of 29.5 kg/m2, and the third was associated with endometriosis. Old age, marked obesity and associated ovarian pathology could modify the vascular response. Follow up of patients with this pattern showed that, no case of severe OHSS was recorded. Pattern II "Aggressive pattern" The vascular morphology was that of irregular branches, several coils and angles with marked dilatation (Figures 4, 5), associated with low RI = 0.48-0.52, that of newly formed vessels (devoid of muscular layer). This pattern was observed in 7 patients (29%), associated with serum E2 > 5000-7000 pg/ml. OHSS developed in 3 patients (14%), 2 cases were moderate and one case was severe OHSS. DISCUSSION
Three-dimensional ultrasound is a new, accurate and non-invasive emerging technology. The implementation of 3D display with power Doppler ultrasound permits the physician to see three dimensional on the screen interactively, rather than mentally assembling the sectional image. It displays the total flow in a confined area, giving an impression similar to that of angiography (11). In our study, 3D power Doppler ultrasound allowed us to study ovarian stromal blood flow in more details and reflects the degree of neovascularization "angiogenesis" that stays behind the pathogenesis of OHSS. The descriptive terms applied in this observational study is a trial to classify the cases according to possibility for OHSS development. So, "reassuring pattern"; applied when the vascular morphology detected on 3D power Doppler supports the clinical situation, i.e. no risk of OHSS, while the "aggressive pattern"; raises the possibility for OHSS to the maximum and calls for immediate preventive measures. To the best of our knowledge, this the first trial to study the ovarian stromal blood flow by 3D power Doppler ultrasound during COH to detect the possibility of OHSS development in high risk PCOS patients. Reports on the use of 3D power Doppler ultrasonography for the evaluation of the polycystic ovaries are scarce (12). Recently, Pan et al., (7) proved that increased ovarian stromal Doppler signal by 3D power Doppler ultrasound may be a possible new ultrasound marker in the diagnosis of PCOS. It is well documented that women with PCOS are at increased risk of developing OHSS during COH for IVF (13, 14). Early Doppler ultrasound studies have demonstrated increased stromal vascularity in PCO (15, 16). One hypothesis is that the increased blood flow and the increased vasculature seen in the stoma of these ovaries, with the resultant increased gonadotrophin delivery, may be responsible for the increased risk of OHSS. Our study is considered a continuation of the work of Pan et al., (7), with 2 exceptions; first, it is a qualitative study of the vascular morphology (reconstructed 3D vascular image) and not a quantitative study of the vascular indices (VI, FI, VFI), second, it is done on stimulated polycystic ovaries (on day of hCG) and not on resting ovaries (on day 2 or 3 of the cycle). In a very recent study by Jarvela et al., (8) they used the same modality "3D power Doppler ultrasound" to evaluate the changes taking place in the ovaries before and after pituitary down-regulation. They proved that the dominant and nondominant ovaries in the preceding cycle showed no differences between each other after GnRH analog therapy, which was also the case when comparing the right and left ovary. They agreed with us that 3D power Doppler ultrasound, as a method, provides a new aspect to examine the changes taking place in ovarian vascularization and blood flow. Thus, the increasing research interest in the ovarian stroma has highlighted the need for a reliable and objective method of stromal analysis, because stromal hyperechogenicity (17) is a notoriously subjective parameter. Review the literatures stated that, "RI value" was taken as a marker for ovarian activity (<0.04 = malignant condition, <0.05 = inflammatory condition & >0.05 = normal condition). As OHSS is considered equal to an inflammatory ovarian condition, so OHSS risk associated with the aggressive pattern became more evident if "RI value" was considered as shown in our study. The clinical observations of severe OHSS occurrence in patients conceived spontaneously (18), in those with low serum E2 levels on the day of hCG administration (19), or the well known practice that high E2 levels do not always lead to OHSS (20), suggest that the previously accepted risk factors, especially high serum E2 levels, are unreliable for the prediction of severe OHSS. Applying these facts to our study, guided us to suggestion that, the combination of 3D vascular image of the ovarian stroma blood flow and serum E2 could be more accurate for the prediction of severe OHSS rather serum E2 alone. As we study the vascular morphology on the day of hCG, we will have enough time for all preventive measures to be taken if a profile of high risk for severe OHSS is recognized (high E2 plus aggressive pattern) e.g.; coasting, reducing the dose of hCG, I.V. albumin on day of oocyte retrieval, cryopreservation of embryos or cycle cancellation. With the recent advances of 3D ultrasound, its clinical application in the field of ART has been widely extended, e.g.; follicular measurement and volume, ovarian volume in PCOS and OHSS, endometrial thickness and volume, congenital and acquired uterine cavity anomalies and tubal patency by 3D sonohysterography (21). In conclusion, 3D power Doppler ultrasound of ovarian stromal blood flow in PCOS (aggressive pattern) could be used as an additional complementary predictor for severe OHSS, if a situation of high risk profile is recognized (E2 > 5000-7000 pg/ml & follicular count > 20 follicles). Moreover, it might be used for reassurance against OHSS development in certain cases of PCOS (age > 35 yrs, BMI > 27 kg/m2 & associated endometriosis) even with very high serum E2 levels, but this observation needs further extended studies. REFERENCES
Copyright © Middle East Fertility Society |

{kind=link}
{kind=link}
{kind=link}
{kind=link}