 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Clinical, ultrasonographic and endocrine predictors of ovarian response to clomiphene citrate in normogonadotropic anovulatory infertility Wafaa M Aboul Enien, M.D.*,Nadia A Barghash, M.D.†,Fayrouz S Mohamed Ali, M.D.† Department of Obstetrics and Gynecology, and Department of Medical Biochemistry, Faculty of Medicine, Alexandria University, Egypt. * Department of Obstetrics and Gynecology, Faculty of Medicine,
Alexandria University, Egypt. Correspondence: Wafaa M Aboul Enien, Dept. of Ob. Gyn., ShatbyUniversityHospital, Alexandria, Egypt Received on June 7, 2004; Code Number: mf04045 ABSTRACT Objective: To identify screening characteristics involved in the prediction
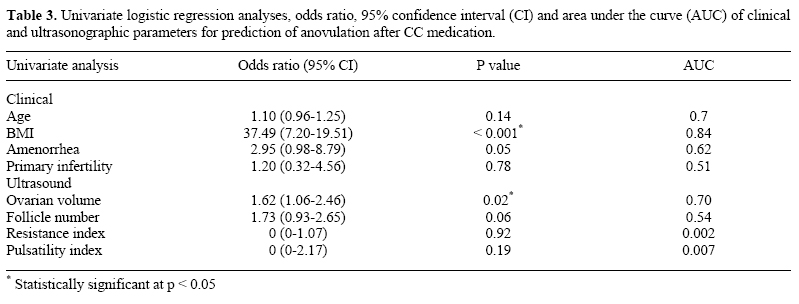
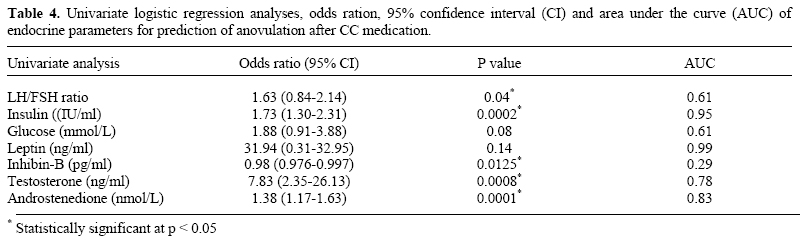
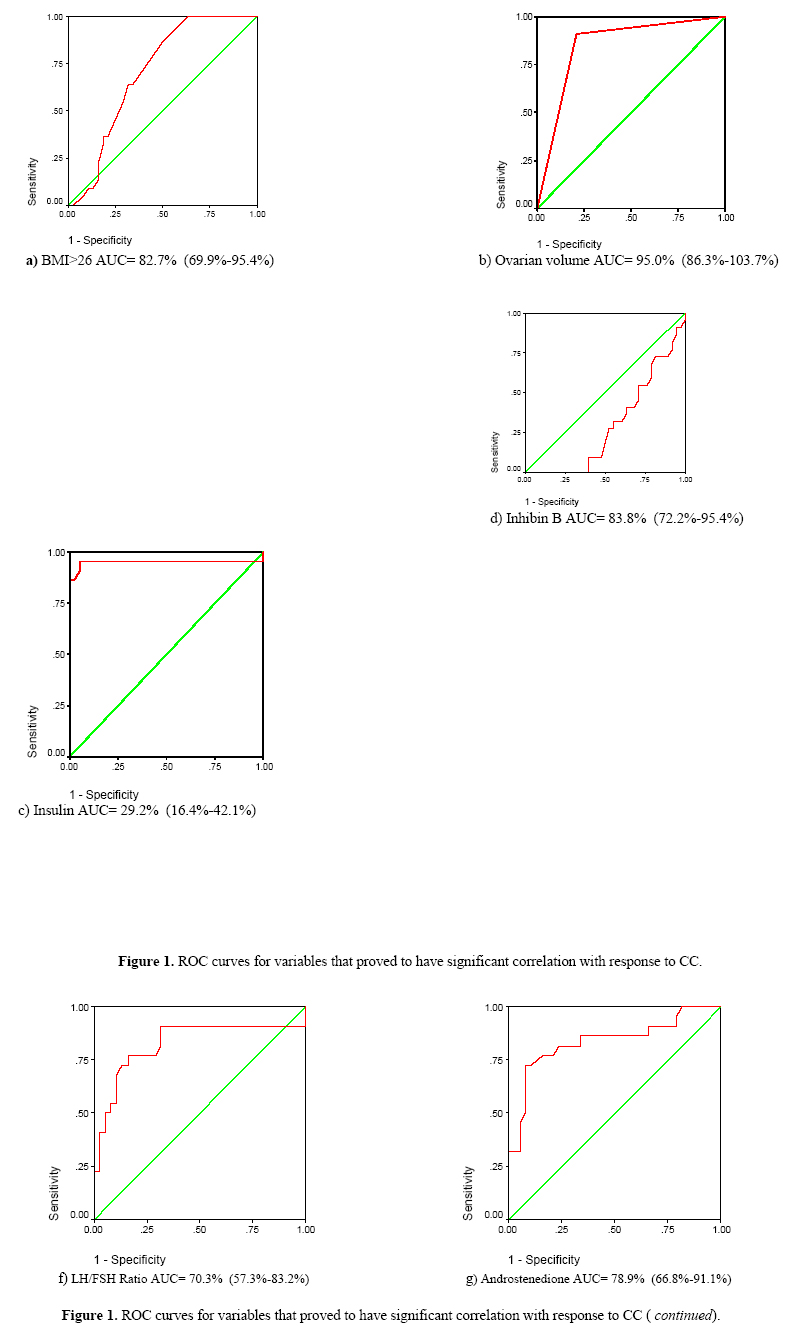
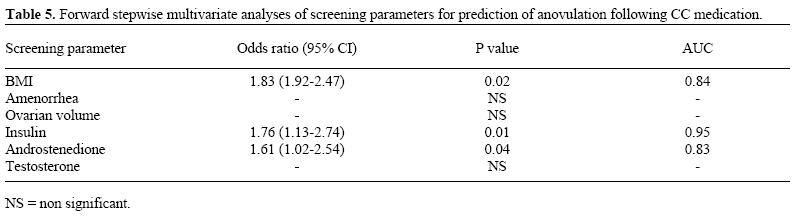
of anovulation after clomiphene citrate (CC) medication. Keywords: Clomiphene citrate, infertility, ultrasound, anovulation, leptin, insulin, inhibin-B. Chronic anovulation is a frequent cause of infertility and approximately 80% of patients present with serum FSH and estradiol levels within the normal range (WHO group 2)(1). The polycystic ovarian syndrome (PCOS) is the most common cause of normogonadotropic normo-estrogenic anovulatory infertility. Despite the heterogeneity of the symptoms associated with PCOS, the essential feature is arrested follicular development at the stage when selection of the dominant follicle should normally occur (2). The cause of arrested follicular growth in PCOS remains unknown, but various investigators reported on the prominent role of insulin resistance, possibly by stimulating thecal cell androgen production leading to gonadotrophin secretory abnormalities and anovulation (3,4). Recently, the role of leptin has been the focus of investigations. Leptin is an adipocyte-derived hormone which plays a central role in the regulation of body weight and energy homeostasis and in signaling to the brain that adequate energy stores are available for reproduction (5). There appears to be a feedback loop linking the hypothalamic-pituitary-gonadal axis and the leptin system, in addition to the direct intraovarian actions of leptin (6). In PCOS, local excess of leptin may cause abnormalities in the FSH control system and in the steroidogenic response induced by intra-ovarian factors as insulin-like growth factor I in the dominant follicle. Reduced estrogen secretion signifies an inadequate signal for LH secretion and thus anovulation (7,8). Furthermore, inhibin B may serve as a marker for ovarian dysfunction in PCOS patients. Inhibin is a dimeric non-steroidal glycoprotein hormone that selectively inhibits FSH release from the pituitary gland. It consists of two partially homologous subunits,α combined with either βA (inhibin A) or βB (inhibin B) (9). Since inhibin B is produced predominantly by the developing small antral follicles, it has been postulated that its concentrations are increased in some PCOS patients. High inhibin B augments LH- stimulated androgen production by theca cells and may be held responsible for an elevated LH/FSH ratio characteristic for some patients (10,11). Diagnosis of PCOS, classically defined by ultrasound as the presence of multiple follicular cysts arranged around an echogenic stroma, is now enhanced with new functional data obtained by color Doppler ultrasound (12). In PCOS, a peculiar vascular pattern has been reported with sustained stromal vascularization, characterized by increased blood flow velocities, low resistance index and low pulsatility index values. This pattern has been correlated to the angiogenic properties of LH (13,14). Clomiphene citrate (CC) is a convenient, inexpensive and safe first choice medication in normogonadotropic anovulatory infertility (WHO group 2). Approximately, 70-80% of patients ovulate after CC medication, whereas 40-50% of ovulatory women conceive (15,16).Despite numerous reports demonstrating that CC exerts its anti-estrogenic actions at multiple levels within the hypothalamic pituitary-gonadal axis, the mechanism underlying its ovulation induction properties remains unclear (17). Although rising serum FSH due to CC interference with estrogen negative feedback may be responsible for stimulating follicle growth, other mechanisms of action have been proposed (18). However, a significant proportion of treated women, do not respond. The aim of the current study was to investigate whether clinical, ultrasonographic and endocrine characteristics during initial screening of normogonadotropic anovulatory infertile women may predict ovarian response to CC medication. MATERIALS AND METHODS The study included 60 patients presenting with oligomenorrhea (bleeding interval > 35 days and < 6 months) or amenorrhea (bleeding interval > 6 months) and infertility. Patients were recruited from the infertility Clinic, Department of Obstetrics and Gynecology, ShatbyUniversityHospital, Alexandria. An informed consent was obtained from all patients. Additional inclusion criteria were serum FSH ≤10IU/L, spontaneous menses or positive bleeding response to progestagen withdrawal, normal serum prolactin and TSH levels, body mass index (BMI, weight divided by the square of patient's height) more than 18 and age from 20-35 years. Clinical, ultrasonographic and endocrine screening took place before initiation of CC medication. Clinical screening included age, BMI, menstrual history, whether infertility was primary or secondary, previous medications and/or surgery. Transvaginal sonographic screening was performed with 7.5 MHz vaginal transducer (Hitachi, model EUB-515, Japan) equipped with color and pulsed Doppler. Ovarian volume, follicle distribution and number were recorded. Ovarian volume was calculated by the formula D1XD2XD3X0.52 where D1, D2 and D3 represented the largest ovarian length, width and depth diameters (19). After assessment of ovarian morphology, color Doppler was used to demonstrate ovarian stromal blood vessels. Although several blood vessels were detected, only the one with the lowest downstream impedance was selected for Doppler measurements. Blood flow characteristics were analyzed and the relative signals assessed in terms of vascular impedance to blood flow (resistance index and pulsatility index). All ultrasound examinations were performed by the same operator. Hormone assays Blood samples were obtained by venepuncture in the early follicular phase before initiation of CC therapy. Serum was stored at –20oC and assayed for prolactin, TSH, LH, FSH, fasting insulin, glucose, leptin, inhibin-B, testosterone and androstenedione. Hormones were measured using enzyme linked immuno-sorbent assay (ELISA) kits. Serum LH and FSH (Eurogenetics Comp, France), serum insulin (Biosource Europe SA Belgium) and expressed in uIU/ml, (20) serum leptin (Diagn Biochem, Canada) and expressed in ng/ml, (21) serum testosterone (Biosource Europe S.A. Belgium) and androstenedione (Diagn Prod Corp, USA). Dimeric inhibin B concentrations were assessed using an immuno-enzymometric assay obtained from Serotec (Oxford, Oxon, U.K.) and expressed in pg/ml (22). CC ovulation induction protocol CC medication was initiated on day 3 after spontaneous or progestagen-induced withdrawal bleeding. The starting dose was 100 mg/day, orally, for 5 consecutive days. In case of absent response, daily doses were increased by 50 mg in the next cycle. First ovulation was used as the end-point and the duration of follow-up was three treatment cycles.Ovulation was assessed by midluteal serum progesterone and transvaginal sonographic monitoring of follicle growth. Responders were defined as patients who ovulated during CC therapy, independent of the dose administered. The number of treatment cycles and the CC dose in which the first ovulation occurred were recorded. Non-responders were patients who did not ovulate despite receiving maximum CC dose of 150 mg/day. Statistical methodology Data were collected and coded then entered into an IBM compatible computer, using the SPSS Version 10 for Windows. Entered data were checked for accuracy and normality, using Kolmogorov-Smirnov test, and did not prove to be normally distributed. Qualitative variables were expressed as number and percentage, whereas, quantitative variables were expressed as median and range. The statistical tests used were X2-test for comparison between the distribution of two qualitative variables, Fisher's exact test for comparison between the distribution of two qualitative variables wherever the X2 test was inappropriate, Mann-Whitney test (Z-value) for comparison of parameters between responders and non-responders and Spearman's rank correlation coefficient (r) to measure the mutual relationship between two non-normally distributed quantitative or ordinal variables. Univariate and multivariate logistic regression analyses were used for prediction of anovulation in response to CC medication. A 5% level was chosen as the level of significance in all statistical tests used. RESULTS From the total study group of 60 patients treated with CC medication, 48 (80%) had primary infertility, 23 (38.3%) had amenorrhea, 28 (46.7%) were considered obese (BMI ≥ 26) and 39 (65%) presented with elevated serum LH (≥7 IU/L) (23) 22 patients (36.6%) remained anovulatory despite receiving maximum CC dose of 150 mg/day. A total number of 124 CC cycles were analyzed. In Table 1, the clinical and ultrasonographic characteristics are presented for the overall study group and separately for responders and non-responders after CC medication. The median age and percentage of obesity was significantly higher in non-responders compared to responders. Moreover, in non-responders, ovarian volume was significantly increased and the resistance and pulsatility indices of ovarian stromal blood vessels significantly decreased denoting increased vascularity. Endocrine screening parameters of the overall study group and separately for patients who did or did not ovulate after CC medication are shown in Table 2. The LH/FSH ratio, fasting insulin level, serum leptin, testosterone and androstenedione were significantly higher and inhibin-B levels significantly lower in non-responders. P values after univariate analysis with logistic regression analyses, odds ratio, 95% confidence interval, and the area under the receiver operating characteristics curve (AUC) of screening parameters are shown in Table 3 and Table 4. Again BMI, ovarian volume, LH/FSH ratio, serum insulin, inhibin-B, testosterone and androstenedione were significantly different between CC responders and non-responders. The receiver operating characteristics curves (ROC) of variables that proved to have significant correlation with the response to CC are shown in Figure 1. By using forward stepwise multivariate analyses for the prediction of clomiphene resistant anovulation, the capacity of ovarian volume, LH/FSH ratio, serum testosterone and inhibin B were eliminated, and 3 variables were eventually selected: BMI, serum insulin and androstenedione. Combining the three screening parameters showed a good predictive power with AUC equal to 0.87. The final prediction model for anovulation was statistically significant where chi-square = 62.43 (P < 0.001). Data are presented in Table 5. DISCUSSION PCOS is one of the most common endocrine dysfunctions in women of reproductive age (24). Despite the various clinical and experimental data published, the pathogenesis of this syndrome remains uncertain. The present study was designed to investigate whether ovarian response after CC medication could be predicted in normogonadotropic anovulatory infertility. If patients remaining anovulatory despite CC therapy could be identified, ineffective and time-consuming CC treatment could be prevented. This may be helpful particularly for women of advanced reproductive age. In the current study, we focused on ovulation rather than conception. Ovulation is most closely relevant to the desired effects of CC medication, whereas conception as the end-point requires a comprehensive study of other factors as male factor, tubal factor, and endometrial function. As a first step we focused on the clinical screening parameters of the studied group. BMI and age were significantly higher in CC non-responders, however in univariate and multivariate analyses, only BMI had a good predictive power for anovulation. This is in agreement with previous studies (25,26). A positive correlation between body weight and CC dose required to induce ovulation has been established (27). Concerning the ultrasonographic screening characteristics, ovarian volume was significantly increased and the Doppler indices of ovarian stromal blood vessels significantly decreased in CC non-responders. Similar findings were reported in previous studies (26,28,29). However, ovarian volume was the only significant ultrasonographic predictor of anovulation in univariate analysis but not when tested among other variables (multivariate analyses). Our data confirm previous observations pointing to increased stromal blood flow within the polycystic ovary (30). However, contradictory results were reported by other investigators stating that polycystic ovaries do not bear an inherent disturbance in blood flow dynamics of the uterine and ovarian arteries, as measured by color Doppler (31). Endocrine parameters potentially related to ovarian dysfunction in PCOS were the main focus of the present study. LH/FSH ratio, serum insulin, leptin, testosterone and androstenedione were significantly higher and inhibin-B significantly lower in CC non-responders. When a univariate analysis was applied, the capacity of serum leptin to predict CC resistant anovulation was eliminated. Furthermore, in the final multivariate prediction model, serum insulin and androstenedione were the only endocrine parameters chosen to predict anovulation after CC medication. The current study also suggests that LH/FSH ratio is implemented in ovarian dysfunction in PCOD. This agrees with previous studies (32). However, others contradict this finding (27). Our observations suggest that obese hyperandrogenic hyperinsulinaemic women are less likely to respond to increased stimulation by FSH, suggesting that these factors are crucial in inducing follicle maturation arrest. Similar results were reported in previous studies (25,26,33). The correlation between BMI and ovarian response after CC suggests that much emphasis should be focused on weight reduction. Furthermore, the disturbed dominant follicle selection in hyperandrogenic patients may result from disrupted enhancement of FSH-induced aromatase activity. This could be due to intraovarian dysregulation of FSH action either by locally produced growth factors or insulin resistance (34,35). The role of insulin resistance has been of interest as recent reports suggest that ovarian dysfunction may improve after the use of insulin sensitizing agents (36). Through its action on insulin-growth factor-I receptor, elevated insulin may increase thecal androgen synthesis in response to LH and stimulate ovarian stromal angiogenesis. Furthermore, insulin has a strong negative effect on sex hormone binding globulin concentration, with resulting high free androgen levels that could be held responsible for CC unresponsiveness (12,16). In the current study, serum leptin was assessed as it participates in the regulation of ovarian folliculogenesis by a direct regulatory activity and indirectly via the control of LH and FSH secretion. Since circulating leptin levels are directly related to body adiposity, hence elevated leptin concentrations associated with obesity may partly explain the negative impact of obesity on fertility (37). In our study, serum leptin was significantly higher in CC non-responders, which is in accordance with previous reports (8,33). Finally, serum inhibin-B was significantly lower in CC non- responders and a predictor for anovulation in univariate analysis. Our results are in accordance with those of Seifer et al (38) who reported that women with low day 3 inhibin levels demonstrate a poorer response to ovulation induction and are less likely to conceive. However, this is contradicted by other studies denoting similar inhibin B levels between CC responders and non responders (33,39,40). The clinical importance of the findings in this study is that weight loss is the first-line therapy for obese women with PCOS and that even normal weight and lean women should respond to pharmacological measures to improve insulin sensitivity, such as administration of agents like metformin, with decrease in both ovarian and serum androgens. In conclusion, the present follow-up study demonstrates that body mass index, serum insulin and androstenedione are the predominant predictors for anovulation after CC medication. REFERENCES
Copyright © Middle East Fertility Society |

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}