 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Peritoneal fluid leptin and interleukin-15 in pelvic endometriosis Mohamed Abd El-Salam, M.D.*,Gamal Kenawy, M.D.†,Ashraf El-Mashad, M.D.*,Mamdooh Abadeer, M.D.† Obstetrics and Gynecology, and Medical Biochemistry Departments, Benha Faculty of Medicine, Zagazig University, Egypt *Department of Obstetrics and Gynecology, Benha Faculty of Medicine,
Zagazig University, Egypt Received on August 19, 2004; Code Number: mf04037 ABSTRACT Objective: This study investigated the relation between peritoneal
fluid (PF) leptin and interleukin-15 (IL-15) concentrations and the severity
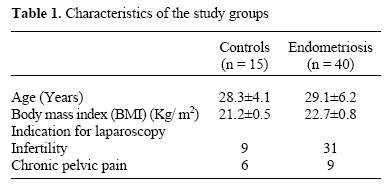
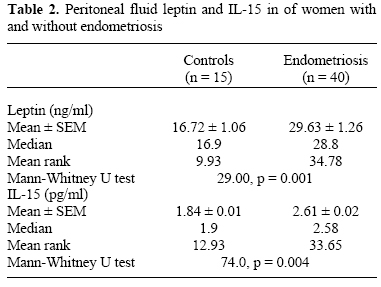
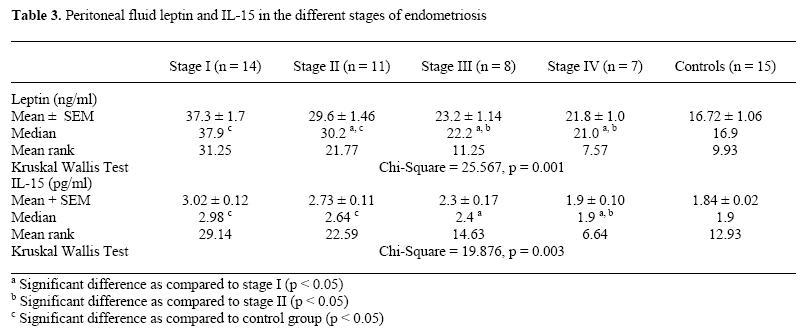
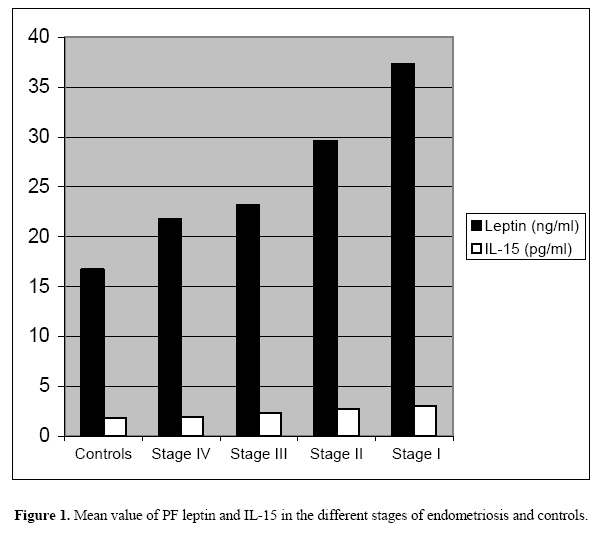
of pelvic endometriosis. Key Words: Endometriosis - Peritoneal fluid - Leptin - Cytokines- Interleukin-15 Endometriosis is defined as the presence of endometrial tissue outside the uterus. Although the pathogenesis of endometriosis is unknown, the theory of retrograde menstruation in conjunction with immunological and peritoneal factors that stimulate angiogenesis and cell growth is currently the most widely accepted explanation (1). Growth factors and inflammatory mediators produced by peritoneal leukocytes are postulated to participate in the pathogenesis of endometriosis. These include interleukins (IL), tumor necrosis factor (TNF), monocyte chemotactic protein (MCP-1), transforming growth factor (TGF-b) and vascular endothelial growth factor (VEGF) (2-5). These cytokines are increased in the peritoneal fluid (PF) of women with endometriosis. In most cases MCP-1, IL-6, IL-8, IL-10 levels were found to correlate with the severity of the disease (6-9). IL-15 is a recently described cytokine that activates the beta and gamma chains of IL-2 receptor. There is increasing evidence that IL-15 may play an important role in diseases where mononuclear cell infiltration is a hallmark feature (10). IL-15 activates human natural killer (NK) cells (11) and promotes lymphocyte proliferation and migration (12). IL-15 is produced by a wide variety of cells and tissues, among which are epithelial cell lines and monocytes. Human endometrium expresses IL-15, most abundantly in the secretory phase of the cycle (13). Progesterone is a potent inducer of IL-15 mRNA expression by human endometrial stromal cells (14), although this effect may be mediated by prostaglandin E2 and interferon-gamma (15). Leptin is a 16 kDa adipocyte-derived protein belonging to the class of helical cytokines. It is the product of the obese gene, and regulates food intake and energy expenditure (16). Circulating concentrations of this hormone are correlated to body fat mass. During inflammatory responses, leptin is produced in the acute phase and represents an early reactant together with C-reactive protein and IL-1β (17). Recent evidence suggests that leptin has immunoregulatory properties. In particular, it shows a marked and specific effect upon CD4+ T-cell responses and their cytokine profiles (18). Furthermore, leptin has angiogenic promoting activities in vivo and in vitro (19). Leptin also induces vascular permeability, and synergistically stimulates VEGF and fibroblast growth factor-2 (20). The concentration of leptin in endometriosis has recently been investigated. Serum leptin was found to increase in patients with endometriosis compared to controls (17). In the present study, we investigated leptin and IL-15 concentrations in the peritoneal fluid of women with endometriosis and their correlation to the severity of pelvic endometriosis. MATERIALS AND METHODS Peritoneal fluid samples were collected from women undergoing laparoscopy at the Department of Obstetrics and Gynecology, BenhaUniversityHospitals between September 2001 and August 2003. Indications for laparoscopy included evaluation of infertility or chronic pelvic pain. Women were classified according to the findings observed during laparoscopy. Peritoneal biopsies were taken from all patients with laparoscopic evidence of pelvic endometriosis for histopathological confirmation. The endometriosis group included 40 women with pathlogically confirmed endometriosis. They were classified into 14 cases stage I, 11 cases stage II, 8 cases stage III and 7 cases stage IV according to the revised American Fertility Society (21) classification. Fifteen women undergoing laparoscopy for evaluation of infertility or pelvic pain served as controls. They had normal pelvic anatomy. All women with or without endometriosis had not used any hormonal therapy for at least 3 months before laparoscopy. Exclusion criteria were: clinical and/or ultrasonic stigmata of polycystic ovarian disease, diabetes mellitus, systemic hepatic, thyroid or inflammatory disease, at time of laparoscopy. All women underwent laparoscopy under general anesthesia after at least 12-hour fasting. After the induction of pneumoperitoneum with 3-4 L of CO2, the pelvis was carefully observed by a 10 mm, 0 degree sheath of laparoscopy inserted at umbilicus. The PF was collected by aspiration from anterior and posterior cul-de-sac at the beginning of laparoscopy. Samples were not used if bleeding into the pelvic cavity from the abdominal stab punctures was observed. The PF sample was placed in a sterile tube and centrifuged immediately at 3000 rpm for 15 min using a cooling centrifuge at 4oC. The supernatant was collected, aliquot and stored at -80oC until assayed. Biochemical Assays Supernatants derived from PF samples were diluted in carbonate buffer pH 9.6 before being used. Quantitative measurement of PF leptin was done by enzyme-linked immunosorbent assay (ELISA) (22) using a monoclonal antibody-based ELISA kit (Med. Diagn. Comp., Germany). The results were expressed in ng/ml. Quantitative measurement of PF IL-15 was done by enzyme amplified sensitivity immunoassay (EASIA) (12) using a monoclonal antibody-based solid phase EASIA kit (Medgenix Diagnostic S.A., USA). The results were expressed as pg/ml. The minimal detection limit of the assay for leptin was 0.2 ng/ml while for IL-15 was 0.5 pg/ml. Statistical Analysis Numeric values were expressed as means ± SEM. The non-parametric Mann-Whitney and Kruskal-Wallis tests were used for the statistical comparison of the variables in the various groups. Student t test was used for comparison of means of parametric data. Pearson's correlation coefficient was used to correlate PF leptin, IL-15 levels, age and stage of endometriosis. A P-value of < 0.05 was considered statistically significant. All analyses were performed using the statistical software package for the social sciences (SPSS Inc., Chicago, IL) on an IBM personal computer. RESULTS Table 1 shows that there was no significant difference in mean age between controls (28.3 ± 4.1) and women with endometriosis (29.1 ± 6.2). Moreover, no significant difference was found in body mass index among women with and without endometriosis (21.2 ± 0.5 vs. 22.7 ± 0.8 Kg/m2). Table 2 shows that the mean rank of PF leptin was significantly higher in women with endometriosis compared to controls (34.78 vs. 9.93, p = 0.001). Furthermore, the mean rank of PF IL-15 was significantly higher in endometriosis group compared to controls (33.65 vs. 12.93, p = 0.004). Table 3 shows that PF leptin and IL-15 levels were significantly different in the various stages of endometriosis. There was a significant difference in PF leptin in women with endometriosis according to the stage of the disease (Kruskal Wallis Chi-Square test = 25.567, p = 0.001). Moreover, there was a significant difference in PF IL-15 in relation to the stage of the disease (Kruskal Wallis Chi-Square test = 19.876, p = 0.003). The PF leptin from stages I and II was significantly higher than stages III and IV. In addition, significantly higher concentrations of IL-15 were found in stage I than stage III and IV (figure 1). A significant negative correlation was found between PF leptin levels and the stage of endometriosis (r = -0.578, p = 0.001). Moreover, a significant negative correlation was found between IL-15 and the stage of endometriosis (r = -0.425, p = 0.001). Furthermore, a significant positive correlation was found between PF leptin and IL-15 levels in endometriosis group (r = 0.381, p <0.05). However, no significant correlation was found between age and both variables. DISCUSSION The present work demonstrated that PF leptin levels were significantly higher in women with endometriosis compared to controls. This result is in accordance with previous studies (17,22,23). Leptin is known to stimulate angiogenesis (19, 24) and to induce vascular permeability (20). Angiogenesis is believed to be a necessary requirement for sustaining endometriotic implants (25). Park et al., (24) reported that leptin induces expression of matrix metalloproteinases in vitro and in vivo. Matrix metalloproteinases play a critical role in the invasion of endometrial cells into the mesothelium (26). Moreover, Wu et al., (27) reported that high doses of leptin enhance mitogenic activity in cultured endometrial stromal cells. Thus, leptin may provide a link between angiogenesis, invasion of the mesothelium and endometrial stromal proliferation. The obtained results showed that PF leptin levels were higher in women with stage I and II endometriosis than those with more invasive advanced stage disease. Moreover, there was a significant negative correlation between PF leptin and stage of endometriosis. This finding is in accordance with results of Matarese et al., (17); DePlacido et al. (22) and Mahutte et al. (23). Although endometriosis cells express the leptin receptors, mRNA levels for the receptor decrease in association with increasing stages of the disease (27). This might explain the inverse relation between PF leptin levels and stage of pelvic endometriosis. Both leptin receptor and, to a lesser extent, leptin itself are expressed in human endometrium (28). Moreover, the expression of leptin mRNA is significantly increased in endometriosis cells as compared with eutopic endometrium (27). Thus, endometriosis implants are both a potential source of leptin production and a potential target for its action, particularly in stages I-II of the disease. This finding might indicate that leptin may play a role in the pathogenesis of peritoneal endometriosis. The present findings demonstrated that PF IL-15 levels were significantly increased in endometriosis group compared to controls. This goes in hand with the results of Arici et al., (29) who demonstrated increase level of IL-15 in PF in women with endometriosis more than control group with no endometriosis. Cytokines are believed to play a major role in the pathogenesis of endometriosis. They serve as immunomodulators, angiogenic factors and agents promoting endometrial cell growth (30). IL-8 is believed to have a major facilitatory role in the development of endometriosis (31). IL-15 has some similarities to IL-8. IL-15 inhibits neutrophil apoptosis (32), stimulates the production of matrix metalloproteinases (33), and has a role in angiogenesis through up-regulating secretion by endometrial natural killer (NK) cells (34). This study showed a significant inverse correlation between endometriosis staging and IL-15 levels. Moreover, PF IL-15 levels were significantly higher in stage I compared to stage III and IV. These results were in agreement with that obtained by the study of Arici et al., (29). The inverse correlation between the stage of disease and PF IL-15 levels is distinct from other PF cytokines such as IL-6, VEGF and MCP-1 all of which have been shown to correlate positively with the stage of endometriosis (31). Although the reason for this is unclear, it suggests a possible role for IL-15 in the early pathogenesis of endometriosis (29). Such a role of IL-15 in endometriosis is consistent with its recognized role in other early immune responses. For example, although both IL-2 and IL-15 stimulate T-cell proliferation in vitro, there is evidence in vivo that IL-2 renders T-cells susceptible to apoptosis, whereas IL-15 initiates T-cell division (34). Similarly, although both IL-2 and IL-15 activate NK cells, IL-2 renders them susceptible to apoptosis whereas IL-15 prevents apoptosis (35). Such data suggests that early in the immune response, prior to activation of T-cells, IL-15 generates activated NK cells as a first line defense. However once T-cells become activated, they produce sufficient IL-2 to keep the NK and T-cell response in check. Hence, IL-15 may have a more prominent role in early as opposed to late endometriosis (29).The inverse correlation between PF leptin, IL-15 and the extent of endometriosis may be explained by the fact that the pathogenesis of early peritoneal endometriosis is different from deep late endometriosis. Whereas PF factors may play an important role in peritoneal disease, deeper lesions may be more influenced by hematological or ovarian actors (36). In the current study, there was a significant positive correlation between leptin and IL-15 in endometriosis group. Leptin has intrinsic angiogenic and mitogenic properties that may be induced by the inflammatory cytokine IL-15. Moreover, IL-15 may up-regulate leptin secretion (29). In conclusion, this work demonstrated that PF leptin and IL-15 are elevated in women with endometriosis particularly in the early stages of the disease. This could suggest a role for leptin and IL-15 in the pathogenesis of peritoneal endometriosis and development of endometrial peritoneal implants. REFERENCES
Copyright © Middle East Fertility Society |

{kind=link}
{kind=link}
{kind=link}
{kind=link}