 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
The effect of intramural fibroids on the outcome of IVF Mona M. Aboulghar, M.D.,Hesham G. Al-Inany, M.D.,Mohamed A. Aboulghar, M.D.,Gamal I. Serour, M.D., Ragaa T. Mansour, M.D., Ph.D. The EgyptianIVF-ETCenter, Maadi, and Department of Obstetrics and Gynecology, CairoUniversity, Cairo, Egypt Correspondence: Mona Aboulghar, M.D., The Egyptian IVF-ET Center, No. 3 Street 161, Hadayek El-Maadi, Maadi, Cairo11431, Egypt, Fax: +202-3383049, E-mail: monaaboulghar@yahoo.com Received on August 12, 2004; Code Number: mf04048 ABSTRACT Objective: To evaluate the effect of fibroids on outcome of IVF and
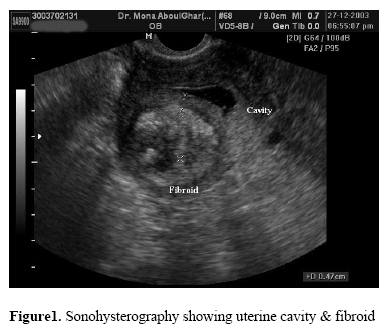
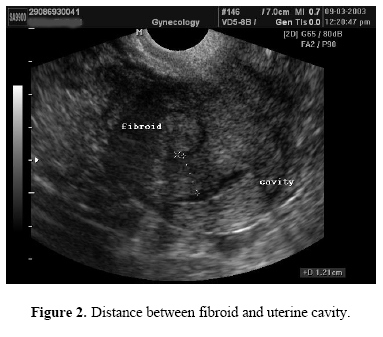
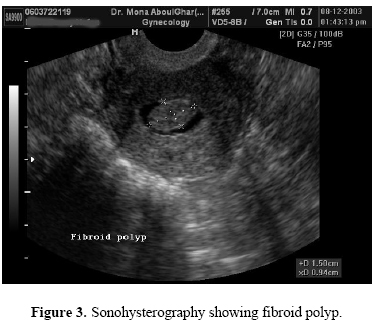
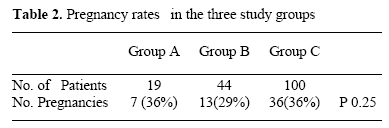
study value of myomectomy prior to IVF. Keywords: Fibroid, myomectomy, endometrial cavity, Sonohysterography, IVF Uterine fibroids are known to affect >30 % of women above the age of 30(1). The incidence of fibroids in infertile women with no obvious cause of infertility is estimated to be between 1 and 2.4% (2). Submucous fibroids are known to be associated with subfertility and increased miscarriage rates (2,3) proved by a reduction of 50% in spontaneous abortion rates after myomectomy (2). However, debate still exists on the effect of intramural fibroids on fertility and on the results of IVF. Only a few studies have been published regarding this issue (7-16) and no prospective randomized trial has been done. The aim of this study was to evaluate the effect of intramural fibroids on the outcome of IVF and to compare the value of surgical excision versus non-excision of fibroids before IVF-ET trial. MATERIALS AND METHODS The present study is a prospective controlled study, which was conducted at the Egyptian IVF-ET center in the period from December 2002 to January 2004. The inclusion in the study was based on the ultrasound examination, done routinely for all our patients before enrolment in the IVF-ET program. A full pelvic ultrasound examination using 2D transvaginal probe (Sonoace 9900, Medison, Korea) was performed. Measurement of the uterus and both ovaries in the three planes were done, assessment of the myometrium for presence of fibroids, and assessment of the endometrial lining; including thickness and appearance. This was followed by sonohysterography (Saline infusion hydrosonography). A speculum was inserted into the vagina, the cervix exposed and painted with povidone iodine. Any patient with mucopurulent discharge was postponed till after treatment. A rigid ET catheter (Cook, Australia) was introduced through cervical canal into the uterine cavity. This was usually easy and rarely required resorting to volsellum manipulation. The speculum was then removed and the vaginal probe introduced. Under ultrasound guidance, sterile saline was injected in the uterine cavity. A maximum of 10 cc of saline was required to distend the cavity. The procedure took approximately 10 minutes for each patient, none of the patients found the examination intolerable. Under ultrasound guidance, distension of the cavity enabled proper evaluation of the endometrial lining and cavity, revealed intrauterine polyps, confirmed submucous fibroids and enabled the exact measurement of the distance of intramural fibroids to the endometrial lining (figure 1, 2, 3, 4). This was done both in sagittal and transverse planes of the uterus. Patients diagnosed as having intramural fibroids were counseled for either myomectomy or no treatment prior to IVF-ET and the choice was left to the patient. All patients with submucous fibroids and uterine polyps were advised to have myomectomy and polypectomy respectively. The hypothesis was believed prospectively that submucous myomas and polyps affect the outcome All patients whether treated by myomectomy or not, received our standard long luteal phase agonist protocol (4). Patients received the GnRH analogue for 2 weeks after which downregulation was confirmed by E2 levels below 40 pg/ml. This was followed by induction of ovulation using IM injections of hMG (the dose determined according to patients' age and weight). Folliculometry was performed staring the 8th day of induction and dose of hMG adjusted thereafter according to response. hCG was scheduled when 3 or more follicles measured 18mm or more. Ovum pick-up was done 36 hours following the hCG injection. Embryos were transferred day 2 or 3 after ovum pick- up (a maximum of 3 embryos were transferred), using the Wallace catheter (H.G.Wallace Ltd, West Sussex, UK) or a Cook catheter (Cook, Australia). Luteal phase support was given routinely in the form of a daily progesterone injection (100 mg, progesterone; Steris, Phoenix, AZ, USA) till b-hCG testing was performed and if patient was pregnant till the first pregnancy ultrasound. A serum b-hCG test was done to confirm pregnancy two weeks after embryo transfer. Clinical pregnancy was diagnosed 3 weeks after a positive test by the presence of a gestational sac with fetal echoes and pulsations on ultrasound. Statistical analysis Data were statistically described in terms of mean, standard deviation (± SD) and percentages. Comparison between different groups in the present study was done using Student t test for comparing continuous data when normally distributed and Mann Whitney U test when not normally distributed. For comparing categorical data, Chi square (X2) test was performed. Yates correction was used instead when the frequency is less than 10. A probability value (P value) less than 0.05 was considered significant. All statistical calculations were done using computer programs Microsoft Excel version 7 (Microsoft corporation, NY, USA) and SPSS (Statistical Package for the Social Science; SPSS Inc. Chicago, IL, USA) statistical program. RESULTS There were 185 patients enrolled in the study. The etiology of infertility was mixed; including tubal, male factor and unexplained infertility. The patients were divided into the following four groups; Group A, included 19 patients, who were treated by myomectomy. Group B, included 44 patients who did not undergo myomectomy. Group B was subdivided, according to distance of intramural fibroid from endometrial lining into B1, 11 patients with fibroids at a distance of less than 5 mm from the endometrial lining and B2, 33 patients at a distance of more than 5 mm. A third group C, included 100 control patients chosen from an age-matched group of tubal factor infertility patients. Group D included 11 patients with submucous fibroids and 10 patients with fibroid polyps. The intramural fibroid sizes ranged from 10 – 76 mm. The Mean age of the patients and the mean infertility period in the four groups is shown in Table 1. There was no statistical difference in the mean age or the infertility period between all 4 groups. Table 2 shows the number of pregnant patients and pregnancy rates in the three study groups. Pregnancy rates between groups A, B and C were found to be non significant. Out of 11 patients diagnosed with submucous fibroids; 6 underwent myomectomy 2 became pregnant (18%). Out of 10 patients with intrauterine polyps, who all underwent polypectomy, 6 became pregnant (60%). Table 3 demonstrates the pregnancy rates of subgroups B1 and B2. There was no statistical difference in pregnancy rates of both subgroups. However there was a trend to increase in pregnancy rates in patients with fibroids at a distance of >5 mm from lining who did not perform a myomectomy. DISCUSSION Only a few studies have searched into the effect of fibroids on results of IVF (7-16). The etiology of reduced implantation potential of embryos in patients with fibroids is unclear but proposed factors are vascular changes, hyperplasia atrophy or inflammation of the endometrium or presence of local transmitter substances in the myometrium (5). In addition altered uterine contractility has also been proposed as an interfering factor with fertility (6). Most authors agree to the negative effect of submucous fibroids on fertility and therefore most of the studies included only intramural fibroids not distorting the cavity, except for 3 studies; Jun et al (7) studied 141 patients with fibroids at various locations including submucous. They found no significant effect on pregnancy outcome so long as cavity is normal and size was <7cm. Eldar-Geva et al (8) included submucous fibroids in their study as well. They found significant reduction in implantation and pregnancy rates, even with no deformity of the cavity. Narayan et al (3) found submucous fibroids to be a significant cause of subfertility proved by a significant increase in pregnancy rate after treatment of the fibroids. All other studies included only intramural and subserosal fibroids. Based on the results of the studies the effect of intramural fibroids has proven to be a controversial issue.A few studies found a significant effect of fibroids on the outcome of IVF. Hart et al (9) found a reduction in pregnancy implantation and ongoing pregnancy rates by 50% following IVF, in patients with fibroids. Eldar-Geva (8), found a reduction in pregnancy rates with intramural and submucous fibroids when compared to subserosal and no fibroids. However, Farhi et al (10) in a small study including 46 women undergoing IVF with fibroids, found impaired implantation only when associated with abnormality of the cavity. Stovall et al (11) studied 91 patients performing IVF with intramural and submucous fibroids and found that fibroids significantly reduced the clinical pregnancy and delivery rate. In most of the studies the size of the fibroids was small < 5cm, In our study the maximum size of the fibroids was 7 cm. Oliviera et al (12) in a retrospective study including 245 subserous and intramural fibroids (not distorting the cavity), found no reduction in pregnancy rates for fibroids <4cm., However, there was an insignificant reduction in pregnancy rates with fibroids >4 cm. Other studies found no effect of intramural fibroids on the outcome of IVF, so long as not distorting the cavity (13-17). Our study is the first to determine the effect of the distance of the intramural fibroid from the endometrial lining on IVF results. Although the numbers are small and there was no significant difference in fibroids < 5mm compared to fibroids > 5mm from endometrial lining, yet there was a tendency to higher pregnancy rates with fibroids lying farther away from endometrial lining (>5mm). Larger prospective randomized studies are needed to answer the question of effect of fibroids on results of IVF, and whether size of fibroid or distance to endometrial lining has an effect on clinical pregnancy rate. REFERENCES
Copyright © Middle East Fertility Society |

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}