 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Middle East Fertility Society, Vol. 10, No. 1, 2005, pp. 1-21 REVIEW Strategies for fertility preservation and gonadal protection during gonadotoxic chemotherapy and radiotherapy Mohamed A. Bedaiwy, M.D. Division of Reproductive Sciences, Department of Obstetrics and Gynecology,
University of Toronto, and Mount Sinai Hospital, ON, Canada. Received
on October 19,
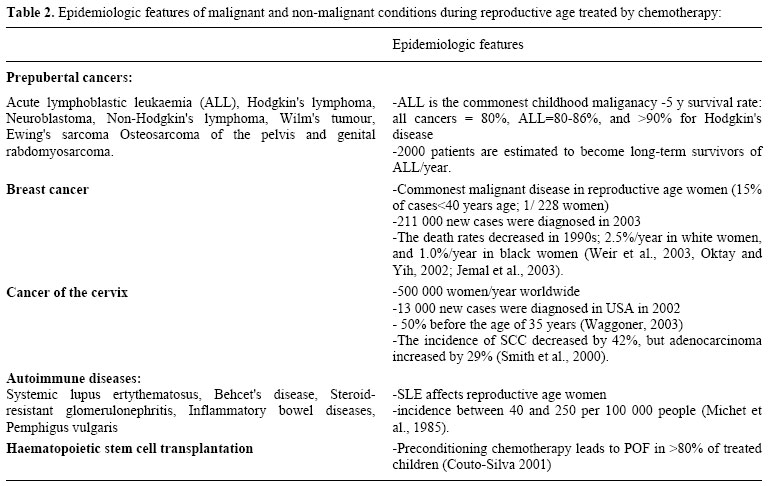
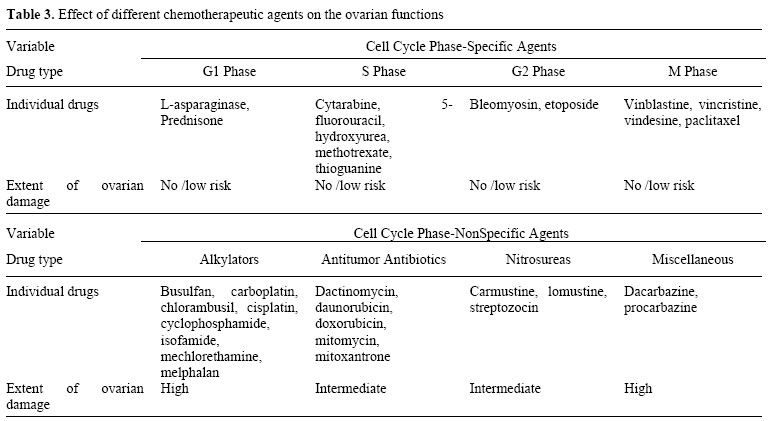
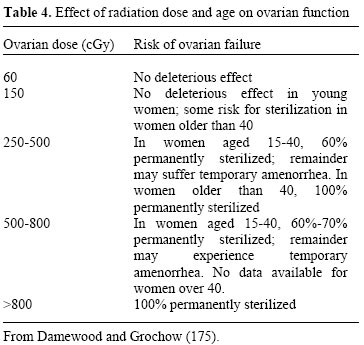
2004; Code Number: mf05001 ABSTRACTWith the recent report of a pregnancy and delivery after autotransplantation of cryopreserved-thawed ovarian cortical strips, preservation of the reproductive potential resurfaced. There is a growing academic and public interest in exploring the available strategies for fertility preservation in patients at risk. This is due to the increasing incidence of cancer during the reproductive age. The overall survival and cure rates of reproductive age cancers are improving due to improvements in cancer therapy. Reproductive derangement is one of the major consequences of cytotoxic chemotherapy and radiotherapy. GnRh analogues concomitant therapy, laparoscopic ovarian transposition, oocyte cryopreservation, embryo cryopreservation and transplantation of cryopreserved-thawed ovarian tissue, are all strategies for fertility preservation in patients at risk. However, no evidence-based strategy is available yet. This article discusses the mechanisms of reproductive failure after gonadotoxic therapy and the currently available fertility preservation strategies. Key words: chemotherapy/fertility preservation/ovarian failure/radiotherapy. INTRODUCTIONAbout 15 % of treatments of childhood and adolescent cancer carry a substantial risk to future fertility. This risk varies according to the presenting pathology and requires treatment. It has been estimated that at the year of 2000, one in 1000 adults will be a survivor of childhood cancer (1, 2). This was due to the current use of multi-agent chemotherapy regimens and/or well-tailored radiotherapy. However, this was on the expense of reproductive functions and future fertility of those patients (3, 4). Consequently, better attention has been paid to prevent reproductive failure in those patients. Moreover, it was also reported that 650,000 new female cancer cases are estimated to be diagnosed in 2003 in the USA (2). Approximately 8% of them occur during the reproductive years (5). In addition, there is a steady incremental decline of cancer mortality rates for all malignancies in women. It was estimated that the decline rate is 0.6% per year during the period from 1992 to 1999 despite an increase in the incidence by 0.3% per year from 1987 to 1999 (2). The National Cancer Institute (NCI) estimated the number of survivors of all child hood cancers to be 1 per 1000 population in 1997 (6). It is estimated that by the year 2010, 1 in 250 patients will have survived malignancies (7). Summary of the distribution of cancers among women in the reproductive age is shown in table 1. Besides the expected premature ovarian failure and its consequences, multi-agent chemotherapy and high dose radiotherapy may be associated with early pregnancy loss, premature labor and low birth weight (8, 9). There is a growing concern regarding the future reproductive functions in pediatric oncology survivors. Moreover, the safety of offsprings of those survivors may be subjects to future abnormalities. Consequently, there is increasing demand for a fertility preserving interventions. On the other side, there is an increase in the techniques to preserve fertility via medical protection, surgical procedures, assisted reproduction and cryopreservation (10). In this article we will review the pathophysiology of chemotherapy/radiotherapy induced gonadal toxicity and current techniques of fertility preservation. Possible future options will also be discussed. CHEMOTHERAPY-INDUCED OVARIAN FAILUREReproductive age malignancies treated with chemotherapy Premature ovarian failure (POF) is a well-known consequence of exposure of the female gonad to chemotherapeutic drugs (11, 12). A wide variety of malignant and non-malignant conditions during the reproductive age are treated with gonadotoxic chemotherapy (Table 2). Patients are exposed to these agents for treatment of malignancies such as acute lymphoblastic leukemia (ALL). ALL is the commonest childhood malignancy and it is estimated that more than 2000 patients are destined to be long-term survivors of ALL each year (13). In addition to leukemias, patients with Hodgkin's lymphoma, neuroblastoma, non-Hodgkin's lymphoma, Wilm's tumor, Ewing's sarcoma and osteosarcoma of the pelvis and genital rhabdomyosarcoma receiving chemotherapy are at risk of developing POF (14-17). In addition, breast cancer is the commonest malignancy in women during the reproductive age (18). There is steady rise in the incidence and decline of the case fatality rate of female breast cancer (18). It is estimated that 1 out of every 228 women will develop breast cancer before the age of 40. Moreover, 15% of all breast cancer cases are estimated to occur at <40 years (2, 5). The well known gonadotoxic cyclophosphamide-based multiagent cytotoxic chemotherapy is one of the combinations of choice in treating such disorder (19). Cancer of the cervix is another malignancy that might affect reproductive age women and some of those patients receive radiosensitizing chemotherapy which again might affect their gonads. It is estimated that 13, 000 new cervical cancer cases were diagnosed in USA. Around 50% of the new cases were diagnosed before the age of 35 years (20). Following the routine screening program, there is an estimated decline of squamous cell carcinoma of the cervix by 42%, however, the estimated incidence of adenocarcinoma of the cervix increased by 29% (21). Autoimmune disease is another non-malignant indication of chemotherapy. Systemic lupus erythematosus (SLE) is the commonest member of this category to affect reproductive age women. The incidence of SLE is 3 per 1000 people (22). High dose cyclophosphamide, with or without haematopoietic cell transplantation (HSCT), could be used in these patients with subsequent risk of POF (23). Chemotherapy with alkylating agents is also used in other autoimmune diseases as Behcet's disease, autoimmune glomerulonephritis, Crhon's disease, ulcerative colitis and pemphigus vulgaris that probably affects reproductive age women (24-26). Recently, HSCT has been used in the treatment of autoimmune diseases previously unresponsive to immunosuppressive therapy, diseases associated with genetically abnormalstemcells,aplastic anemia, myelofibrosis, sickle cell anaemia, autoimmune thrombocytopenia (27). HSCT has also been used in patients with breast cancer, multiple myeloma and lymphoma (28). Pre-existing bone marrow ablation using cytotoxic chemotherapy is a pre-requisit before HSCT. This is commonly a cyclophosphamide/busulfan-based regimen. Both are known with their deletrious effects on the ovary (29). Factors affecting the extent of chemotherapy-induced gonadotoxicity Chemotherapy-induced gonadotoxicity is almost irreversible. Histologic sections of the ovary following exposure to cytotoxic drugs showed a spectrum of changes ranging from decreased numbers of follicles to absent follicles to fibrosis (30). As survival rates continue to improve for young cancer patients, the reproductive consequence of exposure to chemotherapeutic agents becomes a significant concern. The exact incidence of POF following chemotherapy is difficult to establish since many factors contribute to ovarian failure. Bines and associates evaluated the effects of adjuvant chemotherapy in pre-menopausal women with breast cancer (31). They reported the rates of amenorrhea among the different chemotherapeutic regimens and analyzed the variables that may have attributed to amenorrhea. Depending on the type of chemotherapy regimen used, the incidence of chemotherapy related amenorrhea ranged from 0-100%. Rates of amenorrhea varied from 21-71% in the younger age group as compared to 49-100% in the older age group. The risk of gonadal damage increases as the age of the female increases, likely due to the presence of a lower number of remaining oocytes compared to the younger patient. Type of chemotherapeutic agent Cytotoxic chemotherapeutic agents are not equally gonadotoxic (Table 3). The drug regimen used (type, duration, and dose) alsodetermines the likelihood of POF. Alkylating agents such as cyclophosphamide, L-Phenyalanine mustard, and chlorambucil produce permanent damage to gonadal tissue by interacting chemically with DNA. They cause inaccurate base pairing and produce single and double stranded breaks. Thus DNA, RNA and protein synthesis is inhibited. Agents that do not induce permanent ovarian failure include: 5-Fluorouracil, methotrexate, etoposide, and doxorubicin. In one study in which seven women with osteosarcoma were treated with methotrexate, there was no evidence of premature ovarian failure or gonadal dysfunction (32). Also gonadal dysfunction has not been demonstrated in women treated with methotrexate for high risk vesicular mole and choriocarcinoma. Differential sensitivity of the different cellular components of the ovary to chemotherapeutic agents The close structural and functional relationship between granulosa cells and the oocyte make it difficult to establish the exact target of cytotoxic drugs. Destruction of either one leads to demise of the other. These drugs may impair follicular maturation and/or deplete primordial follicles (30,33). Temporary amenorrhea will result when maturing follicles are destroyed by cytotoxic drugs. Permanent amenorrhea or POF will result when all primordial follicles are destroyed. There is conflicting data regarding the sensitivity of the primordial follicle to cytotoxic drugs. The primordial follicles of the mouse are sensitive to cyclophosphamide but those of the rat are not (34,35). Since alkylating agents are not cell cycle specific, they may be able to act on both the oocyte and pregranulosa cells of the primordial follicles leading ultimately to their destruction (36,37). The dose of the cytotoxic agents used The cumulative dose of the cytotoxic drug being administered is a key factor impacting permanent ovarian failure. Goldhirsch and associates demonstrated a steadily increasing rate of POF, ranging from 10%- 61% as the cumulative dose of cyclophosphamide increased(38). Younger women require higher cumulative doses of cytotoxic drugs than older women before amenorrhea is induced. "The average dose of single agent cyclophosphamide before the onset of amenorrhea was 5200 mg, 9300 mg, and 20,400 mg among 40, 30, and 20 year olds respectively" (39). These investigators also demonstrated that the "cumulative dose appears to be more important than the dose rate since administration of low daily doses of cyclophosphamide given over several months was only slightly less effective at inducing permanent ovarian failure than a high dose in 4 days". Finally older women have a shorter duration to onset of amenorrhea after exposure to cytotoxic drugs. Bines's review showed that women younger that 40 years experienced amenorrhea 6-16 months after initiation of chemo versus women older than 40, who experienced amenorrhea within 2-4 months (31). The effect of duration of treatment and route of administration on gonadal toxicity is not yet clear. The population of women that may potentially require gonadal protection against alkylating agents is quite large including breast cancer. In the typical regimen of CMF ( cyclophosphamide 11-15 grams, methotrexate, 5-fluoro-uracil), two thirds of breast cancer patients will become amenorrheic. With the AC ( doxorubicin, cyclophosphamide) protocol 34 % will be amenorrheic at 3 years. This figure is worse if taxanes ( such as docetaxel) are also used with this regimen. Women age Prepubertal girls seem less susceptible than young women to cytotoxic drugs (40). Treatment of girls with up to 50,000 mg of cyclophospahmide failed to induce ovarian failure in this population (41). Nicosia et al showed that while the number of growing follicles was reduced in patients receiving combination chemotherapy regimens, there was no significant change in the number of primordial follicles (42). This may explain the apparent decreased susceptibility of the pre-pubertal ovary to cytotoxic drugs. The true incidence of POF in this population is unclear since long-term follow-up studies are rare (40,43-46). Most of these studies have documented subsequent menarche and ovulatory cycles in these patients (46). When the outcome of subsequent pregnancies in these patients was reviewed, the frequency of congenital anomalies in the children born to them was not increased (47,48). However, others debated that young girls are equally susciptable to chemotherapy-induced gonadotoxicity (17,49). On the other hand, women with advanced age are more susciptable to chemotherapy induced gonadal toxicity as previously discussed. RADIOTHERAPY-INDUCED OVARIAN FAILUREReproductive age malignancies treated with radiotherapy Several cancers afflicting young premenopausal women can be cured with radiation therapy. These include cervical, vaginal and ano-rectal carcinomas, some germ cell tumors, and CNS tumors. Due to early detection, approximately half of the patients with cervical cancer are premenopausal and about a third under 40 years of age (50). An even higher proportion of women are premenopausal with the other aforementioned cancers (51). The radiation doses to the ovaries with standard pelvic radiation therapy will uniformly induce ovarian failure. Total body irradiation has been also used in conditioning regimens prior to HSCT to eradicate the host's pre-existing bone marrow as in leukaemias. This is commonly associated with ovarian failure (4). Factors affecting the extent of radiotherapy-induced gonadotoxicity The ovarian follicles are remarkably vulnerable to DNA damage from ionizing radiation. Irradiation results in ovarian atrophy and reduced follicle stores (52). On the cellular level, oocytes show rapid onset of pyknosis, chromosome condensation, disruption of the nuclear envelope and cytoplasmic vacuolization. Serum levels of FSH and LH rise progressively within 4-8 weeks following radiation exposure along with a decline in serum E2 levels (53). The degree and persistence of ovarian damage, and suppression of ovarian function, is related to the patient's age and the dose of radiation to the ovaries (1,51,53) (Table 4). In addition, the extent and type of radiation therapy whether abdominal, pelvic external beam irradiation, or brachytherapy are contributory factors. The fractionation of the total dose plays an important role in determining the extent of ovarian damage as irradiation is more toxic when given in single dose compared to fractionated doses (1). Two studies indicated that the break point for radiation induced ovarian failure is around 300 cGy to the ovaries. Only 11 - 13% experienced ovarian failure below 300 cGy versus 60 - 63% above that threshold value (54). The addition of chemotherapy increases the risk of premature ovarian failure (55,56). A dose-dependant reduction in the primordial follicle pool was noted upon exposing the ovary to radiotherapy (57). At ovarian dose >6 Gy irreversible ovarian failure is encountered due to the extremely sensitivity of the oocytes to radiotherapy (58). It was also estimated that <2 Gy is enough to destroy 50% of the oocyte population (LD50 <2 Gy) (59). Long-term reproductive functions after radiotherapy The risk of ovarian failure was evaluated in long-term childhood cancer survivors after abdominal and pelvic irradiation for more than 16.4 years (41). When both ovaries were in the irradiation field, ovarian failure occurred in 68% of the patients, and in 14% of the patients when both ovaries were at the edge of the treatment field. When one or both ovaries were outside of the abdominal treatment field, POF was not noticed. Successful full term pregnancies were reported (60), when the ovarian functions are saved even in part (61). If pregnancy is achieved, various obstetric complications were reported notably; early pregnancy loss, premature labour, and low birthweight (8,9). FERTILITY PRESERVATION STRATEGIESA wide array of options has been tested as fertility preserving strategies. However, none of them was tested in a prospective randomized controlled trial. Many of the available techniques are experimental and totaly based on case reports, retrospective studies and expert opinions. Pharmacologic Protection Gonadotropin releasing hormone agonists (GnRH-a) After noting that premenarchal female gonads appear to be least sensitive to cytotoxic drugs (40,48), investigators attempted mimicking this state by using GnRH agonists. There is some evidence in the murine and rat models that adjuvant treatment with GnRH-a might protect the gonad (62-64). Presumably by suppressing gonadotropin elevation, GnRH-agonists inhibit the normal physiologic loss of primordial follicles by recruitment and subsequent atresia. There is some controversy regarding the existence of GnRH agonist receptors on human ovary, while GnRHa receptors have clearly been detected in the rat ovary. Thus the response may not be similar across species. The protective effect of GnRH-a on primate ovaries has been investigated. Ataya et al., found that GnRH-a protected the Rheusus monkey ovary from cyclophosphamide-induced damage. Six monkeys received cyclophosphamide injections. They were divided into two groups and received either depo-lupron or placebo injections. 64.4± 2.8% of the total primordial follicles were lost in the cyclophosphamide only group verusus 28.9 ±9.1% in the lupron group(65). Same authors failed to demonstrate any protective effect of GnRH analogue treatment against radiation-induced ovarian injury in rhesus monkeys. Germinal epithelium is extremely sensitive to irradiation, and despite some reports showing a protective effect, it seems unlikely that radiotherapy-induced gonadal damage can be prevented by gonadal suppression (66). Multiple studies have failed to show a protective effect of GnRHa on human male gonads exposed to cytotoxic drugs (67,68). Waxman performed one of the first clinical studies in which GnRH-a was utilized to down regulate the ovaries of eight women undergoing chemotherapy. At follow up, 4 of 8 women were amenorrheic who had received the agonist and 6 of nine controls were amenorrheic. Thus it appeared that buserelin was not effective in preserving fertility in this population of humans (67). Blumenfeld and colleagues have reported on the largest group of females exposed to both cytotoxic drugs and GnRH-a thus far. Sixty patients with lymphoma were initiated on GnRH-a 7-10 days prior to their chemotherapy regimen. The control group consisted of 60 historical patients of similar age range treated with chemotherapy but not GnRH-a. The rate of POF was 5% versus 55% in the GnRH-a/chemotherapy versus chemotherapy alone group (69-71). However, this study was an observational one, with historical control group and relatively short follow up period. Recently another preliminary report has been released regarding the use of GnRH-a for protection of the adolescent ovary during cancer treatment. All GnRH-a treated adolescents resumed cyclic ovarian function, where as all chemo only patients experienced hypergonadotropic hypogonadism (46). However, others debated a role of gonadal suppression in women in preserving ovarian function against chemotherapy (17). They argued that ovarian reserve is made up of primordial follicles that constitute 90% of the total follicle pool (72). Primordial follicles initiate follicle growth through an unknown mechanism which is FSH independent (73). FSH receptors are not expressed in primordial and primary follicles, but the expression is uniformly present in as early as 3-4 granulosa layer preantral follicles (17, 118). This means that GnRH analogues preserve only follicles that have initiated growth which constitute only <10% of all the follicular pool at any given time in the ovary. Once growth has been initiated, they are destined either to become atretic or to ovulate. It is quite possible that GnRH analogue co-treatment delays the fate of these follicles; hence giving the impression that ovarian function is protected in the short run. On the other hand a counter argument propose a direct action of GnRH in the ovary were recently proposed (17,74). Moreover, luteinized immortalized granulosa cell lines were shown to express GnRH receptors (75); however, no evidence so far that these receptors are on human primordial follicles or oocytes. Furthermore, pre-pubertal children receiving heavy chemotherapy still suffer from ovarian failure as reported by some authors (49). Meirow proposed that as younger patients have a larger ovarian reserve, absence of immediate ovarian failure does not mean that gonads are unaffected by the chemotherapy (76). Given the above mentioned arguments and counterarguments a prospective randomized study with sufficient power will appropriately evalute the effectivness of GnRH analogue as a potential strategy for fertility preservation. Apoptotic inhibitors The role of apoptosis in the process of normal germ cell depletion both prenatally and postnatally is well documented (77,78). The existence of a genetic predetermined pathway that initiates and regulates germ cell apoptosis, has raised the possibility that this pathway could be activated aberrantly via chemotherapeutic drugs (79). When mice oocytes were exposed to doxorubicin in vitro, they underwent a series of changes leading to formation of apoptotic bodies (80). Since a series of specific signaling events are activated in the cell bound for apoptosis, inhibition of these signaling events could potentially stop the apoptotic process and protect the patient from premature ovarian failure. Sphingosine-1-phosphate may be an example of an apoptotic inhibitor. Ceramide is a sphingolipid molecule believed to be an early messenger signaling apoptosis in response to stress. The oocytes of mice that lacked the enzyme to generate ceramide, acid sphingomyelinase, and wild type mice oocytes that had been treated with sphingosine-1-phosphate therapy, resisted apoptosis induced by doxorubicin (81). With eventual identification of the molecular and genetic framework of chemotherapy induced germ cell death, apoptotic inhibitors may be one of the most promising stratiegies for preventing oocytes loss. Ovarian transposition For patients subjected to gonadotoxic radiotherapy, ovarian function could be maintained by transposing the ovaries out of the field of irradiation. The ovarian dose following transposition is reduced to approximately 5 - 10% of untransposed ovaries (58,82,83). The dose to each transposed ovary is 126 cGy for intracavitary radiation, 135 - 190 cGy for external radiation therapy (4500 cGy) and 230-310 cGy with the addition of para-aortic node irradiation (4500 cGy) (82). Medial transposition Initially, ovarian transposition for Hodgkin's disease patients receiving nodal irradiation was performed by suturing the ovaries posterior to the uterus and shielding them during treatment. Later, the ovaries were mobilized laterally out of the pelvic field. Gaetini reported that of the 3600 cGy delivered to central axis with total nodal irradiation for Hodgkin's disease, the ovaries in normal position were exposed to 3,524 cGy whereas those transposed medially received 534 cGy and those transposed laterally 319 cGy (55). However, this technique is currently abandoned. Lateral transposition On the other hand, lateral transposition entails dissecting the ovarian pedicle and moving the ovary up the lateral pelvic sidewall. Hadar et al performed CT follow up of 7 cervical cancer patients who underwent lateral ovarian transposition and 9 Hodgkin's disease patients with medial transposition prior to radiation therapy. Six of the 7 patients with lateral transposition had the ovaries outside field and all retained ovarian function. Scattered doses to the ovaries were 100-300 cGy. The 1 patient with ovaries within the field received 450 cGy and developed ovarian failure. Only 3 of the 13 identified ovaries following medial transposition were outside the field. Even the 3 ovaries outside the field received approximately 300 cGy (84). A compilation of 10 case reports and small series comparing medial and lateral transposition noted ovarian failure in 50% and 14% respectively (85). Lateral ovarian transposition was typically performed by laparotomy at the time of radical hysterectomy for cervical cancer or staging laparotomy for Hodgkin's disease. The utero-ovarian ligament is divided and the ovary is mobilized with the ovarian vessels to the paracolic gutters. Ideally, the vascular pedicles are kept retroperitoneal to avoid tension, torsion or trauma and bowel herniation while the ovaries remain intraperitoneal to reduce cyst formation (50,86). van Beurden reported that with a tumor dose of 4,000 cGy for cervical cancer, the ovaries receive 280 cGy at 3 cm and 200 cGy at 4 cm from the radiation field edge due to scatter (87). Bidzinski confirmed that ovarian function was preserved if they were transposed at least 3 cm from the upper border of the field (88). In another study, 100% of the patients whose transposed ovaries were above the iliac crest maintained ovarian function as opposed to none of those whose ovaries were below (89). Ovarian failure may result if the ovaries are not moved far enough out of the radiation field or if they migrate back to their original position. Ovarian failure following transposition may also be due to compromising the ovarian vessels from surgical technique or radiation injury to the vascular pedicle (90). Ovarian transposition is of limited value in patients over 40 as they have an intrinsically reduced fertilization potential as well as a much higher risk for ovarian failure despite transposition (91). Another concern with ovarian transposition is the development of symptomatic ovarian cysts. The mechanism causing the cysts is unknown (92). Laparoscopic approach Currently, it has been recommended that ovarian transposition should be performed laparoscopically just prior to initiating radiation therapy. This will eliminate unnecessary laparotomy in the majority of cervical cancer cases where radiation therapy is not required. An important advantage of laparoscopic ovarian transposition is that radiation therapy can be initiated immediately postoperatively preventing failure due to the ovaries migrating back (56,93-95). In cases of vaginal or cervical cancers being treated by brachytherapy, laparoscopic ovarian transposition can be performed under the same anesthetic for inserting the brachytherapy device (96). Staging laparotomy and splenectomy is no longer required for Stage I and II Hodgkin's disease (56). This eliminates the need for laparotomy as ovarian transposition can be performed laparoscopically with the benefits of being an outpatient procedure with more rapid recovery, less discomfort, better cosmesis and lower cost. Nearly all women with Stage I and II Hodgkin's disease treated with radiation alone or with minimal chemotherapy following laparoscopic ovarian transposition retain their ovarian function and fertility (56). Morice et al reported that 79% preserved ovarian function after laparoscopic ovarian transposition and radiation therapy for various indications (97). Reproductive functions of transposed ovaries The transposed ovaries produce estradiol and progesterone at pretreatment levels (98). The endometrium has been shown to function after brachytherapy and external radiation, though the effect of radiation on the endometrium was not clearly defined (99,100). Critchley studied 10 patients with ovarian failure following whole abdominal radiation. The uterine length was significantly reduced; most had no uterine blood flow detectable by Doppler ultrasonography and 30% showed no endometrial response to hormone replacement therapy. The radiation effect on the uterus was unpredictable but higher doses were more likely associated with vascular and uterine damage (101). Term pregnancies have been reported after intracavitary radiation for cervical cancer (82). Morice et al noted a 15% pregnancy rate after brachytherapy with or without external radiation for vaginal clear cell carcinoma compared to 80% for those treated with external radiation only for dysgerminomas and pelvic sarcomas (102). The much lower rates with vaginal clear cell carcinoma were attributed to DES associated genital malformations and possibly to the effects of brachytherapy on the endometrium. Interestingly, 89% of the pregnancies were spontaneous with 75% occurring without repositioning the ovaries. The ovaries were only repositioned in cases of infertility and 11% of those patients conceived with IVF (97). Tulandi and Al-Took (103) reported a case of laparoscopic lateral ovarian transposition in a patient with rectal adenocarcinoma whereby the utero-ovarian ligaments were divided but the ovaries remained attached to the distal fallopian tubes potentially improving the chances for ovum pickup. The patient achieved a spontaneous pregnancy (95). Several papers addressed the concerns regarding pregnancy outcomes after pelvic irradiation. There was no increase in fetal wastage or birth defects in women treated for Hodgkin's disease (82). Swerdlow et al confirmed that there was no excess of stillbirths, low birth weight, congenital malformations, abnormal karyotypes or cancer in the offspring of women treated for Hodgkin's disease (104). However, Fenig et al cited an increase in low birth weight and spontaneous abortions especially if conception occurred less than a year after radiation exposure. They advised delaying pregnancy for a year after completing radiation therapy (105). There is only 1 case report of superovulation and oocyte retrieval for IVF with transposed ovaries that were not repositioned. A cervical cancer patient underwent laparoscopic lymph node dissection, unilateral ovarian transposition and chemotherapy followed by brachytherapy and external radiation before radical hysterectomy. Transabdominal ultrasound-guided needle aspiration after superovulation with gonadotropins yielded 5 oocytes. The resulting embryos were transferred to a gestational carrier who delivered normal live born twins. It was noted that oocyte retrieval was possible due to the superficial location and lack of mobility of the ovary (106). To facilitate oocyte retrieval, as well as the diagnosis and treatment of ovarian cysts, the ovaries have been transposed subcuticularly. This has the disadvantages of requiring a laparotomy and an additional abdominal incision and may also be associated with a higher rate of cyst formation. Transient ovulatory pain was reported by 81.5% of the patients and 15.4% required needle aspiration (107). IVF with donor oocytes has also been reported in 6 women with ovarian failure following treatment for Hodgkin's disease. All conceived with pregnancy and implantation rates per cycle of 37 and 17% respectively (108). Complications of oophropexy Despite proper shielding, the transposed ovaries are still subjected to a significant amount of radiation, consequently ovarian failure could still happen. Moreover, Fallopian tube infarction, chronic ovarian pain, ovarian cyst formation, and migration of ovaries back to their original position before radiotherapy are all reported complications of oophropexhy (1,56). Anderson et al. (109) reported subsequent oophorectomy in nine of 51 patients (17.5%) for the management of painful ovarian cysts after a mean duration of 46.8 months from the procedure. Spontaneous pregnancy may not be possible, unless a second procedure is performed to relocate ovaries back to pelvis (102). One study found that there was no increased risk of ovarian metastasis in patients with Stage IB cervical carcinoma without gross extracervical disease (110). Another study confirmed no significant difference in 5 year survival rates in cervical cancer patients with and without retained ovaries (111). However, those with tumors >3 cm are at higher risk for metastasis to the ovaries and are not candidates for ovarian transpostion (91). The rate of ovarian metastases was not correlated with histologic type (91,110). Ovarian metastases occurred in 0.5% with Stage IB squamous cell cervical carcinoma and 1.7% with adenosquamous carcinoma (110). For comparison, the risk of ovarian cancer after hysterectomy for benign disease is 0.2% (112). In addition to the very low rate of ovarian metastasis with early stage cervical carcinoma, there is a concern of inducing ovarian cancer due to radiation exposure. No excess cases of ovarian cancer was observed in 2068 women who received 500-1000 cGy to the ovaries for the treatment of menorrhagia followed up for a mean of 19 years (113). Oocyte cryopreservation In single women, freezing mature or immature oocytes may be the only ethically accepted practical option. The main factor that may influence the outcome in oocyte cryopreservation is its structural complexity. Oocyte subcellular organelles are far more complex and perhaps more sensitive to cryopreservation-thawing injury than in preimplantation embryos (114,115). An ideal oocyte cryopreservation protocol should appreciate the essential role of cytoskeletal elements as well as plasma membrane functions in subsequent development (116). Despite the resounding success of mouse mature oocyte cryopreservation (117), these results could not be duplicated in the human scenarios with the same success profile. Among the alternative strategies to nullify the damaging effects of the freezing trauma on M II oocytes is to cryopreserve earlier stages before resumption of full maturation. The relatively inactive metabolism, absence of zona pellucida and lack of the meiotic spindle makes the cryopreservation insult the lowest at the primordial follicle levels (118). On the other hand, antral follicles contain oocytes either in the prophase -1 or metaphase-II stage, and their oocytes are much more liable to cryodamage (119). Both prophase-1 and metaphase-II stages have zona pellucida but MII oocytes have large cell size and which makes cryoinjury more pronounced in M II oocytes. Moreover the meitotic spindle, a unique feature of M-II oocytes, is of particular importance as variations in the temperature may lead to its permanent damage (120). Fewer pregnancies have been reported out of frozen-thawed germinal vesicles oocytes (121-123). In a study to evaluate the cryopreservation of immature human oocytes obtained from unstimulated ovarian tissue, immature prophase I oocytes were obtained from unstimulated follicles and were either cryopreserved or cultured as controls. Rates of cryosurvival and maturation to metaphase II were compared between control oocytes and cryopreserved oocytes with 2 different methods. Lower cryosurvival and maturation rates were demonstrated in cryopreserved-thawed immature oocytes compared to control ones (124). The fair success of cryopreservation is partially attributed to the cryoinjury. A wide spectrum of subcellular damages might happen as a consequence of the freeze-thaw trauma. These include meitotic spindle damage {Pickering, 1990 #142} that may lead to chromosomal instability. Other injuries include destruction of the microtubules, which are an essential component for polar body extrusion, pronuclear migration and cytokinesis (125,126). Furthermore, aneuploid embryos have been obtained from oocytes exposed to 1.5 M DMSO without cooling, which suggests CPA induced DNA damage (127). Other reported abnormalities from cryopreservation of oocytes include hardening of zona pellucida by alteration of its glycoproteins particularly ZP2, which might lead to failure of hatching and implantation (128,129) and abnormalities in cortical granules causing a premature cortical reaction {Schalkoff, 1989 #146}. Better choice of CPA, efficient instrumentation and refinement of the available cryopreservation protocol could minimize or even prevent cryoinjury. Oocyte cryopreservation is currently used electively in patients with ovarian hyperstimulation syndrome. Given the improved cryosurvival, fertilization rates, pregnancies and births, oocyte cryopreservation can be used in cancer patients as a fertility preservation procedure. Despite the early disappointing results with low survival, fertilization, and pregnancy rates after IVF of thawed oocytes (130), recent studies suggesting increased success rates (131-133). Vitrification using ethylene glycol and dimethylsulphoxide (DMSO) as cryprotectants (131,133) are being used successfully by many groups. The mean survival and fertilization rates are 68.4%, 48.5% respectively. However the pregnancy rate is 1.7% per vitrified-thawed oocyte. Once the oocyte cryopreservation technology becomes established with post-thaw survival rates, fertilization rates and pregnancy rates matching those of embryo cryopreservation; it will represent an effective ethically approved strategy for adolescents facing POF. IVF and cryopreservation of preimplantation embryos Results of cryopreservation of preimplantation embryos Embryo cryopreservation was introduced to maximize the conception chances from a single cycle. Delivery rates per embryo transfer utilizing cryopreserved embryos are reported by SART (134) to be 18.6 %. The post-thaw survival rate of embryos range between 35 and 90%, implantation rates between 8 and 30%, and cumulative pregnancy rates can be >60% (135,136). However, this option may not be acceptable to prepubertal, adolescent and women without a partner. If acceptable, long-term data is available about the outcome of children born from these procedures. Ovarian stimulation protocols in estrogen-sensitive cancers Typically a standard IVF protocol is used. Because of time constraints, this is usually a short flare protocol (137). However there is some concern that in patients with breast cancer the high estrogen levels obtained in a standard IVF cycle may impact the long-term survival negatively. For this reason, some centers have offered natural cycle IVF that is oocyte aspiration in an unstimulated cycle. However cancellation rates are high and the pregnancy rates are very low (7.2% per cycle and 15.8% per embryo transfer) (138). The time window between surgery and chemotherapy is main determinant before adopting this policy. This window is around 6 weeks in breast cancer patients, which would be adequate to perform ovarian stimulation and IVF. Given the fact that, conventional COH is associated with significant rise of serum estrogen, which might affect the overall prognosis (139), other ovarian stimulation protocols are more appropriate. Consequently, tamoxifen, a non-steroidal anti-estrogen, commonly used as a breast-cancer chemopreventive agent, was recently investigated for ovarian stimulation and IVF in breast cancer survivors (140). Tamoxifen 40-60 mg was started on day 2 or 3 of the cycle and given daily for 5-12 days and the tamoxifen group was compared to a natural cycle-IVF group. The tamoxifen group had a significantly higher numbers of mature oocytes, peak estradiol, and embryos (mean of 1.6 embryos versus 0.6 embryos) than the natural cycle group (140). In certain group of patients tamoxifen could not be used due to well-known effects on cancer growth as in endometrial carcinomas. Some authors proposed the use of aromatase inhibitors for in these patients (17). Aromatase P450 stimulates the conversion of androgenic substances to estrogens. Letrozole is a potent and highly selective third generation aromatase inhibitor that was developed in the early 1990s. It competitively inhibits the activity of aromatase enzyme, and has a half-life of 48 h (141). Letrozole significantly suppresses plasma estradiol, estrone and estrone sulphate levels using doses as low as 0.1 and as high as 5 mg/day. Letrozole was even more effective than tamoxifen in the treatment of advanced stage post-menopausal breast cancer (142). Moreover, letrozole was introduced as a promising ovulation induction agent. Repeated clinical studies documented its clinical feasibility in ovulation induction. It could be used independently or in combination with FSH. It was also used for the treatment of poor responders (143-145). Many groups are currently testing the feasibility of ovarian stimulation with aromatase inhibitors in breast and endometrial cancer patients. Recently, a successful pregnancy was reported in a patient after conservative management of endometrial adenocarcinoma. A 29-year-old infertile white woman with grade 1 endometrial adenocarcinoma treated by high-dose progesterone therapy underwent an IVF cycle with transfer of three blastocysts after proven cure. The patient delivered triplets by cesarean section. Laparoscopic-assisted vaginal hysterectomy and bilateral salpingo-oophorectomy was then done. No residual endometrial cancer was evident in the hysterectomy specimen, but a 1.1-cm cystic mixed endometrioid and clear cell-type adenocarcinoma was discovered in the left ovary (146). Ovarian stimulation protocols in non-estrogen sensitive cancers In another study, 69 women underwent 113 IVF/gamete intrafallopian transfer (GIFT) cycles after cancer treatment in one partner, and 13 women underwent 13 IVF cycles for embryo cryopreservation before chemotherapy/radiation. The women undergoing IVF after chemotherapy had poorer responses to gonadotropins than did the women with locally treated cancers even though they were younger. The delivery rates after the women had undergone chemotherapy tended to be lower among the systemic treatment group than it was for the local cancer treatment group. The women who had cryopreserved all embryos before chemotherapy produced more oocytes and embryos than did the women who had had a history of local cancer treatment (147). Recently, a case report depicted the feasibility of IVF for the sake of embryo cryopreservation in a patient with colorectal cancer. Controlled ovarian stimulation, IVF, and embryo freezing were performed before fluorouracil-based chemotherapy. The 28-year-old woman subsequently underwent subtotal colectomy. Three years later, when the clinical and hormonal analysis confirmed ovarian failure, two thawed embryos were transferred to the uterus. She gave birth at term to a 3200g infant (148). Cryopreservation and transplantation of ovarian tissue Ovarian cryopreservation and transplantation is an experimental procedure introduced to preserve fertility in women with threatened reproductive potential (149). Studies investigating the effects of cryopreservation insult on ovarian tissues have been limited compared to those studying the same effects on oocytes (150). Unlike a suspended single cell, tissue cryopreservation presents serious physical constraints related to heat and mass transfer. Furthermore, because it is a multicellular structure for which cell-to-cell interactions are known to exist, the dynamics of cryoprotectant permeation into and out of the tissue during cryopreservation are of utmost importance for subsequent tissue survival. Water will be osmotically drawn to the extracellular spaces and blood vessels from the individual cells under the effect of the hypertonic cryoprotectants. It is this water that is responsible for the formation of ice crystals, which is responsible for the freeze-thaw injury (151). Consequently, better survival is expected from primordial follicles because of their smaller size and lack of follicular fluid. As in other reproductive technologies, animal models have provided useful information in transferring methods to treat human infertility. With the sheep ovary providing a reliable tool, Gosden and associates pioneered the sheep ovarian transplantation model. Using cryopreserved-thawed ovarian cortical strips, they showed follicular survival and endocrine function, as well as restoration of fertility after transplantation of cryopreserved-thawed ovarian cortical strips (152,153). Despite the initial success of orthotopic transplantation of cryopreserved ovarian tissue the longevity of the grafts were very short. This was attributed to freezing small pieces of tissue and the ischemic destruction of the ovarian germ cells. Our efforts to improve on the graft longevity and prevention of ischemic destruction of the ovarian follicles went through a consequential cascade of experimental techniques. First, we have shown that increasing the ovarian cortical specimen size and ischemia time up to 30 minutes did not alter ovarian cortical tissue survival (154). Then, we demonstrated that cryopreservation of an entire ovary with its vascular pedicle is technically possible (155). In order to develop a microvascular anastomosis technique for the ovaries, we proved that the anterior abdominal wall is a suitable recipient site for the ovary. The ovarian vessels were anastomosed effectively to the inferior epigastric vessels using microvascualr anastomosis (156). The same technique worked for cryopreserved-thawed intact ovaries as well (157). However, antiovarian antibodies were induced in some cases by changing the site of the ovary (158). We argued that -in theory- all subcutaneous vessels with a matching caliber to those of the ovarian vessels could be potential recipient sites (159). Finally in our last experiment, two intact human ovaries with their vascular pedicles were cryopreserved, thawed and reassessed in vitro in comparison to cryopreserved-thawed ovarian cortical strips. Matching primordial follicles viability and count were observed using the two techniques (160). There are several potential uses of cryopreserved ovarian tissue. Firstly, the tissue can be transplanted back into patient. The potential for reintroduction of a cancer nidus may limit this use in malignancies that are known to have a predilection for the ovaries as leukaemias and lymphomas. Using present techniques, ischemic injury to the transplanted tissue results in the loss of virtually the entire growing follicle population and a significant number of primordial follicles. This could limit its long- term viability. Alternatively the primordial follicles in the ovarian tissue can be matured in vitro or in an immune deficient animal host. The former cannot be accomplished with present technology and the latter is unlikely to be acceptable to patients with a high likelihood of trans-species viral infections. Autografting of human ovarian tissue Oktay and his associates developed 3 different surgical techniques of ovarian cortical strips transplantation. In their first experimental surgery, they placed ovarian cortical strips beneath the pelvic peritoneum of the ovarian fossa laparoscopically. The patient was 17 when right salpingo-oophrectomy was performed for dermoid cyst and at the age of 28, left salpingo-oophrectomy with subsequent cryopreservation of the cortex as a treatment of intractable menometrorrhagia was performed. Transplantation was performed at the age of 29 where partial viability of the cortical strips was proven by in vitro studies. The cortical strips were threaded and anchored to an absorbable cellulose membrane followed by transplantation to the selected site. The graft establishes its blood supply as early as 3 weeks postoperatively as evidenced by doppler ultrasound scanning. After 24 days, of gonadotrophin stimulation, they were able to document ovulation based on hormonal and sonographic features followed by menstruation 16 days after the first hCG injection (161). Another case of orthotopic transplantation of ovarian cortical strips was reported in 32 years old woman with stage IIIB Hodgkin's lymphoma after high dose chemotherapy (162). Seven month after transplantation, she obtained menopausal symptomatic relief and her E2 level rose up to 100pg\mL with a 2 cm follicle at the transplantation site. Complete cessation of the graft function occurred 9 month after transplantation. The fact that the patient received many chemotherapy cycles before cryopreservation may in part be responsible for early failure of the graft. In their second experimental surgery, Oktay and his group used the forearm as the transplant recipient site in two cases. The first patient was a 35-year-old woman with stage III B squamous cell carcinoma. Fresh ovarian cortical strips were grafted over the fascia of the brachiradialis muscle. A fifteen mm follicle was detected utrasonographically 10 weeks after the procedure. Several oocytes were retrieved percutaneaously after gonadotrophin stimulation. Intracytoplasmic sperm injection was tried in a single oocyte but fertilization did not occur. The FSH level was normal at 18 month follow up. The second patient was a 37-year old woman who underwent oophrectomy for recurrent ovarian cysts. Heterotopic transplantation was performed similar to the first patient. The patient resumed her regular menses and ovulated 3 months later. Her graft was still functioning 10 months after the transplant (163). In a final study by Callejo et al (164), these authors evaluated the long-term function of both fresh (3 patients) and cryopreserved (1 patient) ovarian autografts in four premenopausal patients aged 46-49 who underwent heterotopic ovarian transplantation. Although ovarian function was reestablished in three patients, a 2-7-fold increase in FSH levels was reported. One did not have recovery of ovarian function. The limitation in the study was the age of the study population. However, in their third experimental trial Oktay and his team transplanted frozen-banked ovarian tissue underneath lower abdominal skin in a 36 years old breast cancer survivor. Hormonal functions were restored. Percutaneous oocyte aspiration resulted in the generation of a 4-cell embryo (165). More recently, A 32-year-old Belgian woman has given birth to a healthy baby 7 years after banking her ovarian tissue before starting chemotherapy for Hodgkin's lymphoma. Although she became infertile as a result of the chemotherapy, re-implantation of her ovarian tissue re-started ovulation 5 months later. She became pregnant 11 months after re-transplantation by natural fertilization. This is the first case of a human live birth after success of orthotopic autotransplantation of cryopreserved ovarian tissue, in a patient from whom tissue was collected and cryopreserved before chemotherapy was initiated (166). One of the potential limitations of ovarian tissue cryopreservation and transplantation is loss of a large fraction of follicles during the initial ischaemia after transplantation. Previous work indicated that whereas the loss due to freezing is relatively small (153,167,168), up to two-thirds of follicles are lost after transplantation. Given this limitation, it has been recommended that ovarian tissue freezing (17), should be restricted to patients <35 years of age. Research should focus on refinement of the cryopreservation protocols, better cryoprotectants and transplantation techniques that decrease ischemia particularly the use of vascularized grafts (156,157,169). Selection of the transplantation site should consider easy simple and minimally invasive surgical technique. Moreover, amble blood supply to the recipient site is important for graft establishment, survival and long-term function. Subsequent manipulations of the grafted ovary as in follicle aspiration should be made simple. Xenografting of human ovarian tissue Transplantation studies performed in SCID mice have provided extremely important information that is useful in understanding many technical and laboratory aspects of ovarian tissue banking. An important finding was the demonstration of improved follicle growth upon administration of exogenous FSH to the recipient mice. Oktay et al. (170) xenografted human ovarian tissue under the kidney capsules of hypogonadal SCID mice to study the early stages of ovarian follicular growth in vivo. In the absence of FSH, after 17 weeks of grafting, the most advanced follicles contained two layers of granulosa cells. Follicular growth up to the antral stage was significantly improved by employing a daily injection of 1 IU of FSH. In another study, the same group grafted human ovarian cortical strips under the kidney capsule of eugonadal SCID mice without subsequent administration of FSH. Twenty-two weeks later, the grafts were recovered and histopathological examination showed that significant numbers of the follicles had initiated growth (171). In a similar work by Weissman and associates (172), they attempted to evaluate the development of follicles in human ovarian cortex grafted under the skin of non-obese diabetic SCID mice. Exogenous gonadotropin administration 12 weeks after transplantation resulted in follicle growth in 51% of the grafts. Similarly, several groups showed follicle development, ovulation and corpus luteum formation after stimulation of xenografted human ovarian tissue using gonadotrophins in immunodeficient mive (173,174). Concerns regarding retroviral infections may limit the use of this option in clinical practice. CONCLUSIONGnRh analogues are the only available medical protection means for gonadotoxic chemotherapy. However, to be recommended for routine use, their benefits should be substantiated by prospective randomized trials. Laparoscopic ovarian transposition is viable option if radiotherapy is to be used. Oocyte cryopreservation is gaining popularity as a treatment option. The recent improvement in the post-thaw survival, fertilization, implantation and pregnancies rates adds to the practical potential of this option. So far, embryo cryopreservation is the most successful fertility preservation modality. However, it is not applicable in unmarried women due to ethical considerations. Despite the recent reports of embryo development, pregnancy and delivery after transplantation of cryopreserved-thawed ovarian tissue, the technique remains experimental. Because not enough clinical evidence is available today and the demand usually requires urgent answers, a first careful counseling is very important for the best management of the patients. Given the desire of many individuals to preserve fertility after cancer, chronic illness, iatrogenic complications of treatment or simply with advancing age, the ESHRE Task Force on Ethics and Law considered ethical questions and specific dilemmas surrounding the cryopreservation of gametes and reproductive tissue. In view of the transition time during which research becomes therapy, the taskforce stops short of giving recommendations in anticipation of the availability of new evidence, specifically in the case of cryopreservation of reproductive tissues, in-vitro maturation and in-vitro follicle culture. Consent needs to be obtained within a research context rather than for therapy or preservation of fertility per se (176). Finally, all oncologists, gynecologists, and reproductive endoncrinologists should be aware of the available fertility preservation strategies. A multidisciplinary approach is ideal for the management of chemotherapy and /or radiotherapy-induced gonadal failure. REFERENCES
Copyright © Middle East Fertility Society |

{kind=link}
{kind=link}
{kind=link}
{kind=link}