 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
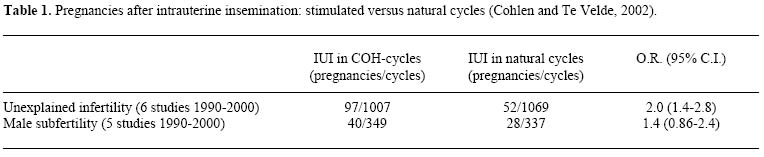
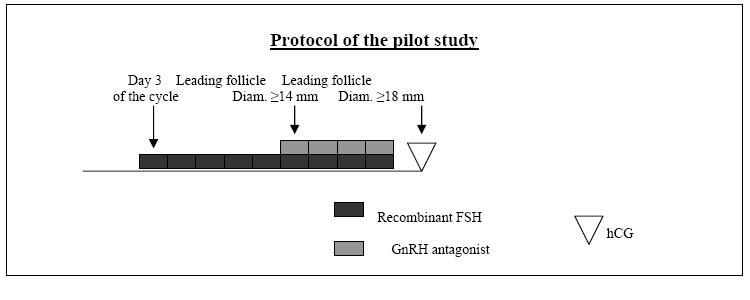
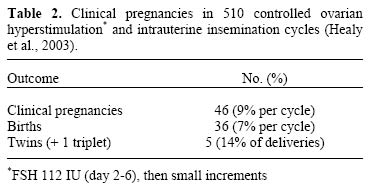
DEBATE The current role of intrauterine insemination for the treatment of male factor and unexplained infertility P.G. Crosignani, E. Somigliana, M. Colombo, A. Riccaboni, and G. Ragni First Department of Obstetrics and Gynecology, University of Milan, Via Commenda 12, Milan, Italy Related Articles: mf05004,mf05005,mf05006, and mf05007Code Number: mf05003 Introduction For couples with male or unexplained infertility, intrauterine insemination (IUI) is more effective than timed intercourse and cervical insemination (Farquhar et al., 2004). In women with idiopathic infertility IUI in stimulated cycles further improves the pregnancy rate compared with natural cycle IUI (Table 1). (Figure 1) The need for milder ovarian stimulation The following have a negative impact on IUI outcome: - duration of infertility - age of the female partner - history of pelvic inflammation - presence of severe male factor(s). Nevertheless, the most important risk associated with IUI after ovarian stimulation is the incidence of multiple gestation that can be as high as 29% (Gleicher et al., 2000). This is why in the presence of more than three follicles it has been suggested the procedure should be stopped or the cycle converted to IVF, but despite this risk the method is still widely used. Milder ovarian stimulation methods have been recently introduced in order to reduce the risk of iatrogenic twin pregnancies. Reduced FSH dose Simply lowering the follicle stimulating hormone (FSH) dose can give an acceptable rate of pregnancy per cycle (≈ 10%) with a lower rate of twins and triplet (Table 2). Low dose FSH + antagonist In a pilot study carried out by our group, the combined use of low-dose recombinant FSH and a GnRH antagonist induced the growth of 1-2 follicles in the vast majority of the cycles (Ragni et al., 2004). Starting on day 3 of the cycle, patients were given recombinant FSH (Puregon(R)) 50 IU per day, and the GnRH antagonist Ganirelix (Orgalutran(R)) at the dose of 0.25 mg per day was started from the day when a leading follicle >14 mm in mean diameter was visualized, until HCG administration. Despite the presence of only one or two follicles IUI produced an unexpectedly high number of clinical pregnancies (11 in 32 cycles). As unexplained infertility is the best diagnosis for IUI and was the indication for treatment of the majority of patients in this study, this could be the reason for the high rate of pregnancies. Nevertheless, taking into account that in idiopathic infertility after multifollicular ovarian stimulation the expected rate of pregnancy after IUI is 10%, and considering the small number of mature follicles (1-2), an improvement in the quality of oocytes could be another reason for the success rate. A better quality of follicles stimulated by low-dose FSH and controlled by the antagonist is also suggested by a recent study in previously poorly responsive ICSI patients (12) observed during a second "spontaneous" ICSI cycle. These women were treated when the follicle reached a diameter of 14-15 mm with low-dose FSH and a GnRH antagonist (for a few days) and the new method of pharmacological treatment normalized the ovarian response, leading to a good normo-responder success rate (Ubaldi et al., in press). Similarly the use of a GnRH antagonist improved the IVF-ICSI results in patients who had already undergone ovarian hyperstimulation in previous cycles (Somigliana et al., 2004).
To corroborate the findings of the pilot study a multicenter European trial has been recently started and if its results confirm these data the rigid rule\ “more oocytes, more pregnancy” will be broken and it will be possible to achieve good clinical results without the unacceptable risk of multiple pregnancies. REFERENCES
Copyright © Middle East Fertility Society |

{kind=link}
{kind=link}
{kind=link}