 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Middle East Fertility Society, Vol. 10, No. 1, 2005, pp. 43-48 Out-patient hysteroscopy: findings and decision making for treatment of abnormal uterine bleeding in pre- and post-menopausal women Ashraf M. N. Refaie, M.D., M.R.C.O.G.,Trevor Anderson, F.R.C.O.G.,Sow S. Cheah, F.R.C.O.G. Department of Obstetrics and Gynecology, Erne Hospital, Cornagrade Road,
Enniskillen, UK Received on September 13, 2004; Code Number: mf05008 ABSTRACT Objective: To assess the feasibility of outpatient hysteroscopy for
identifying abnormal findings in uterine cavities of pre- and postmenopausal
women presented with abnormal uterine bleeding (AUB) and how can out-patient
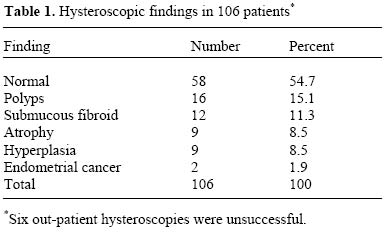
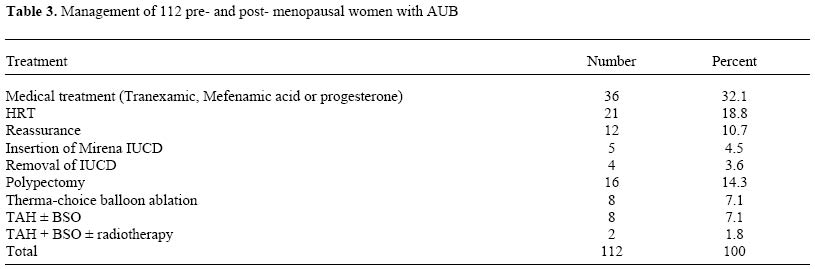
hysteroscopy affect the decision making for treatment. Key words: Hysteroscopy, ultrasonography, abnormal uterine bleeding. Abnormal uterine bleeding (AUB) is a common gynaecological problem. Up to 33% of women referred to gynaecological outpatient clinics have this problem and the proportion raises more in pre- and postmenopausal women. This condition has enormous consequences with regard to social life, morbidity and clinical workload (1-3). Hysteroscopy as an outpatient procedure is an important method for diagnosis of AUB (4,5). This technique has replaced the procedure of dilatation and curettage (D&C), which is a blind technique with a high diagnostic failure rate (6,7). Although the major role of out-patient hysteroscopy in the management of AUB, is diagnostic, there is scope for simple operative procedures such as polypectomy, and targeted endometrial biopsy (5). Transvaginal sonography (TVS) has been studied as an alternative to hysteroscopy in the investigation of AUB, but was found to have a significantly lower sensitivity compared with hysteroscopy and a comparable specificity in premenopausal patients (8). More information is available with regard to TVS in the investigation of postmenopausal bleeding (9,10). Many devices are now available for out-patient endometrial sampling. An example is Pipelle device that can be used for this purpose. The major problem with outpatient sampling procedures alone is that they can miss endometrial polyps or submucous fibroids. This is most important in postmenopausal women where there is a greater incidence of malignant polyps. Hysteroscopy can be of help in guiding biopsy taking (11). MATERIALS AND METHODS One hundred and twelve women with AUB were enrolled in this study over a period of six months. Patients with infertility problems, recurrent miscarriages or missed foreign bodies were not included in this study. The mean age was 49 ± 6 years (range 29-75). At Erne hospital, hysteroscopy is performed in a dedicated clinic within the endoscopy unit. Patients with AUB seen in gynaecological outpatient clinic had history taken and clinical examination performed. A standard letter with specific information about the outpatient hysteroscopy was then sent to the patient. Informed consent was obtained before the procedure. Before seen in the out-patient hysteroscopy, TVS using a multifrequency sector-array (5-10 MHz) transducer (Advanced Technology Laboratories) was arranged to have more detailed information on the uterus and pelvis. The patients with postmenopausal bleeding (PMB) were seen urgently within two weeks. A cut-off level of the endometrial thickness in postmenopausal women in this study was chosen at > 5 mm. Mefenamic acid 500-1000 mg tablets was given to every patient two hours before the procedure as a pre operative preparation. Out-patient hysteroscopy was performed with a Gynecare, Ethicon, disposable 3 mm hysteroscope with 30o. The patient was placed in the lithotomy position, Sim's speculum was inserted and the cervix was grasped using a tenaculum. The hysteroscope was then gently introduced through the cervix into the uterine cavity. Normal saline was used to distend the uterine cavity. Illumination was provided by a Storz cold light source via a fibre-optic cable. Out-patient hysteroscopy was considered successful if an adequate view over the whole uterine cavity was obtained. A Pipelle device (Euro Surgical Ltd, Guildford, UK) was used to obtain tissue for histology. The hysteroscopic findings were recorded in a standardized way. In view of the out-patient hysteroscopic and ultrasound findings as well as the histology, the plan for management is discussed either in the clinic or at a later stage when the histology report is available. RESULTSIn this current study, 63.4% were premenopausal (71/112) while 36.6% were postmenopausal (41/112). Menorrhagia was the most common indication (52 patients) followed by postmenopausal bleeding (PMB) in 40 patients. PMB included patients on hormone-replacement therapy (HRT) and patients who were not on this therapy. Other indications included 16 patients with intermenstrual bleeding (IMB) and 4 patients with postcoital bleeding (PCB). Out of 112 hysteroscopies carried out, six were unsuccessful. This means that the overall failure rate was 5.4%. Two failures were in the premenopausal women (2.8%) and another four failures (9.8%) in postmenopausal. The most common cause of failure was cervical stenosis, especially in postmenopausal women. Twenty four patients underwent repeat hysteroscopy under general anaesthesia at a later stage, either because of failed out-patient hysteroscopy or for other minor procedures such as polypectomy. The most common hysteroscopic findings are shown in Table 1. Normal cavity was seen in almost half of the cases. Endometrial polyps were the most common abnormal hysteroscopic finding in postmenopausal women (26.8% vs. 7% in premenopausal) while submucous fibroids were the commonest finding in premenopausal patients with menorrhagia (12.7% vs. 7.3% in postmenopausal). The endometrium was described as atrophic when looks thin and homogeneous in appearance. Hyperplastic endometrium looks thickened and easily indented by pressure or thick with multipolyp appearance. Adenocarcinoma looks as an irregular growth with or without abnormal vascularization. The ultrasound scan findings were similar to the hysteroscopic ones in most of the cases. Fifty three patients (47.3%) were normal while fibroid and endometrial polyps represented the most common abnormal findings (14.2% and 9.8%) respectively. Atrophy, hyperplasia and adenocarcinoma were seen in 10 patients (8.9%), 19 patients (16.9%) and 3 patients (2.6%) respectively The criteria for abnormal scan in premenopausal women is the one showing (a) distortion of the cavity (b) endometrial thickness more than 16 mm (c) non-uniform endometrial echogenicity (d) myometrium with fibroids > 2 cm or suspected adenomyosis (e) adnexal abnormalities. In postmenopausal women endometrium thickness > 5 mm is considered abnormal. The histology of different lesions is shown in Table 2. The endometrial sampling was insufficient in 19.8% of cases. There were no vasovagal attacks, or significant discomfort. The procedure was easily acceptable by most of patients. Different options of managements are presented (Table 3). Medical treatment such as mefenamic and tranexamic acids, progesterone, HRT and reassurance constitutes two thirds of the treatment. Major surgical procedure such as hysterectomy was performed in only 9% of the patients. Minor surgical procedures such as insertion or removal of IUCD, polypectomy and endometrial ablation represented 29.5% of the whole treatments. DISCUSSION AUB is a common problem and remains an important reason for referral in general gynaecological practice. Hysteroscopy is a superior technique for investigating AUB, with high sensitivity and specificity as intracavitary lesion can be detected under direct view (12,13). Our low overall failure rate in this current study (5.4%) confirmed the feasibility of the technique in a general gynaecological population, and this has been previously reported (14). The 9.8% failure rate in postmenopausal women is acceptable as the patients at this age group may experience higher incidence of stenosed cervicies. Successful out-patient hysteroscopy rate in this series of patients was 94.6% and this agrees with other studies. Decloedt and Fenton (15) reported a 94% successful out-patient hysteroscopies, while a success rate of 96.8% was reported by Alexopoulos et al (16). In this current study direct visualization of uterine cavity by the hysteroscope was superior in detecting all endometrial polyps, submucous fibroids and endometrial atrophies. These entities represent unique conditions where a hysteroscopic diagnosis can be clearly established. The two cases of endometrial cancer were highly suspicious on hysteroscopy and necessitated conventional D&C to confirm the diagnosis by histopathology. Overall abnormal hysteroscopic findings were found in 45.3% (48/106) of all cases in our series of out-patient hysteroscopy. This incidence of abnormal findings justifies using out-patient hysteroscopy in cases of AUB. The incidence and type of abnormal hysteroscopic findings vary according to the age group and presentation. Abnormal hysteroscopic findings were noticed in 73% by Towbin et al (8) in their series of 149 patients with AUB, 91% of them were premenopausal. On the other side Decloedt and Fenton (15) reported an over all abnormal hysteroscopic findings of 32% in patients with AUB but 69% of them were premenopausal and 31% were postmenopausal. Jong et al. (14) found that abnormal hysteroscopic findings to be very uncommon or even rare under the age of 35. In this present series of patients, submucous fibroids were the predominant lesion in premenopausal patients with menorrhagia and intermenstrual bleeding (IMB) (12.7%). Endometrial polyps were a very common finding in patients with postmenopausal bleeding (26.8%). These findings confirm the results published by other authors who reported similar results in their pre- and postmenopausal patients with AUB (6,15,16). In this current study, two patients (1.9%) had endometrial carcinoma as shown by the hysteroscope and confirmed by histopathology. One patient was premenopausal and presented with irregular vaginal bleeding and the other one presented with PMB. The low incidence of endometrial cancer in the postmenopausal patients 2.4% (1/41) is near that reported by other authors and varied between (0.6% to 3.9%) (15-18). The incidence reported in the literature for adenocarcinoma in PMB is usually around 10% (19). Our low incidence of adenocarcinoma in the current study can be explained because the number of postmenopausal patients is not big enough to get meaningful results. A second reason is that the present study included both patients on HRT and those without, where the PMB in patients on HRT could be a withdrawal one. Lastly some postmenopausal patients with PMB may be listed for conventional D&C without being seen in out-patient hysteroscopy clinic. The introduction of TVS has enormously improved the quality of examination of the endometrium and uterus (20). In this present series of patients, ultrasonography diagnosed fibroids and endometrial polyps in 14.2% and 9.8% respectively. The percent of fibroids seen by the ultrasonography was higher than that seen by the hysteroscopy and this can be explained by the fact that ultrasonography can diagnose intramural and subserous fibroids which cannot be seen by the hysteroscope. Ultrasonography is of special importance in postmenopausal women. Simple measurement of endometrial thickness by means of TVS in women with postmenopausal bleeding could be accurately used to discriminate between normal and pathologic conditions (5,20). Several sonographic studies to evaluate a cut off value for endometrial thickness to exclude endometrial cancer have been published (21). An endometrial thickness of >5 mm is most commonly seen in postmenopausal group with malignant changes. In this present study, the adenocarcinoma of the endometrium was encountered in one postmenopausal patient who had an endometrium thickness of 8 mm. The value of ultrasound scan in premenopausal women attending the out-patient hysteroscopy clinic was evaluated by Taylor et al (22) in a group of 264 premenopausal women with AUB. The authors concluded that ultrasound does not appear to be a valuable first-line screen tool prior to hysteroscopy in premenopausal women. This is similar to the conclusion drawn in our series of patients where hysteroscopic findings were found to be more useful for planning for further management. Tissue biopsy performed under direct visualization with hysteroscopy can provide better diagnostic possibilities compared with random sampling where small lesion can be missed (7). Endometrial biopsy was attempted in 106 women in whom the out-patient hysteroscopy was successful. Sufficient material for pathological assessment in this series of patients was obtained in 81% of cases. Endometrial sampling was more likely to be reported as insufficient in the group of women with atrophic endometrium. Management of AUB depends on accurate diagnosis of the cause of bleeding. Medical management with tranexamic and mefenamic acid, progesterone and HRT was the most popular option in patients with normal hysteroscopic findings and normal or atrophic endometrium. Sixty nine women (61.6%) in our patients needed this type of treatment based on the information obtained in the out-patient hysteroscopy clinic. Our observation regarding medical management was also reported by Taylor et al in their study with similar group of patients with normal hysteroscopic findings where 70% of them needed medical treatment (22). Five patients in this series (4.5%) with menorrhagia who needed contraception had the progestogen-only intrauterine system "Mirena". This IUCD releases levonogestrel directly into uterine cavity. It is the contraceptive method of choice in women with heavy period, although not yet officially licensed for treatment of menorrhagia in UK (23). Menstrual bleeding is reduced significantly within 3-6 months of inserting the levonogestrel IUCD probably because it prevents endometrial proliferation. The Royal college of Obstetricians and Gynaecologists "RCOG" has considered progestogen-releasing IUCD as an effective treatment for reducing heavy periods and has recommended its use as an alternative to surgical treatment (24). Out-patient hysteroscopy helped to characterise cases with abnormal hysteroscopic findings that need surgical intervention, either minor or major. Cases with endometrial polyps (16 women) had polypectomy instead of major hysterectomy. Removal of IUCD was performed in four women in whom the IUCDs were displaced as shown by the hysteroscope and sonography. After removal of these devices, the uterine cavity was checked and looked normal. Two women were assured and went on oral contraceptive pills, one had Mirena IUCD and last one had nothing. Endometrial ablation using Thermachoice diathermy was decided in eight patients with intractable AUB in whom the uterine cavity is < 12 cm with no malignancy, atypical hyperplasia or prominent submucous fibroids. Out-patient hysteroscopy is of help in selecting patients for the procedure of endometrium ablation (25). On the other hand, major surgical intervention such as TAH was chosen in eight women with distorted uterine cavities by prominent submucous fibroids. The two endometrial cancers were referred to cancer centre. Major surgical intervention was the option needed by 9% of the whole women included in this current study. As no hospital admission or general anaesthesia was used, out-patient hysteroscopy seems to be cost effective policy. CONCLUSIONOut-patient hysteroscopy appears to be a safe, acceptable and well tolerated procedure that provides useful information about the uterine cavity. Endometrial biopsy improves the diagnostic accuracy of hysteroscopy in detecting endometrial pathology. The accurate diagnosis of the cause of AUB can help to choose the most appropriate treatment without unnecessary major surgical intervention. REFERENCES
Copyright © Middle East Fertility Society The following images related to this document are available:Photo images[mf05008t2.jpg] [mf05008t3.jpg] [mf05008t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}