 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Middle East Fertility Society, Vol. 10, No. 1, 2005, pp. 59-62 Biochemical markers for prediction of pregnancy outcome in cases of recurrent pregnancy loss Amal Darwish, M.D., Nabil Ghorab, M.D., Hazem El-Ashmawy, M.D., Manal Kamal, M.D., Ahmed Soliman, M.D. Department of Obstetrics and Gynecology, Cairo University, Galaa Teaching
hospital, Cairo, Egypt Received on October 24, 2004; Code Number: mf05011 ABSTRACTObjective: To predict pregnancy outcome by studying the relation between
serum βHCG, progesterone and CA125 and the occurrence of miscarriage in the
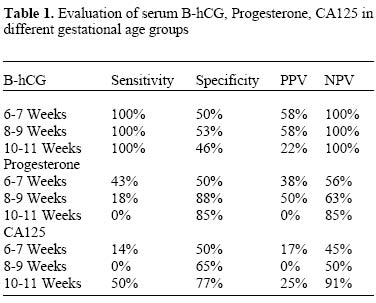
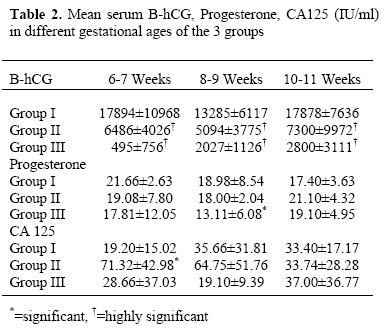
first trimester, in cases with history of recurrent pregnancy loss. Keywords: Recurrent pregnancy loss, abortion, CA125, B-hCG, progesterone The rate of fetal loss in clinically evident gestations has been reported to be approximately 10-15%. The rate will be obviously higher if we consider the preclinical losses diagnosed by β-HCG levels starting 3 weeks following the last menstrual period (1). Accordingly, the expected probability for a woman to have three consecutive abortions should be in the range of 0.3% to 0.4%. The actual frequency of habitual abortion, however, is significantly higher, being in the range of 0.4% to 0.8%. This difference suggests that not only random causes but also some specific factors must be involved in this type of reproductive failure (2). Beta-HCG and Progesterone titers are widely used to assess the risk of miscarriage at the early stages of pregnancy. (3-5). Serum levels of CA125 turned out to be a valuable parameter not only as a marker of ovarian carcinoma but also in other fields of Obstetrics and Gynecology (6). The aim of the study is to evaluate the relation between serum HCG, progesterone and CA125 as biochemical markers at different gestational ages in the first trimester for predicting pregnancy loss. MATERIALS AND METHODSThe study was carried out on 60 pregnant women of comparable age and gestational age in Kasr Al-aini and Galaa hospitals. They were divided into 3 groups. The control group comprising 20 normal pregnant women with no history of miscarriage (Group I), the recurrent aborters group comprising 20 pregnant females with history of two or more 1st trimester pregnancy losses (GroupII) and the last group of 20 patients who failed to complete the 1st trimester of pregnancy (aborting for the first time) during the study (Group III). All were singleton pregnancies of 6-11 weeks of gestation. All groups were subjected to history taking and thorough physical examination. Serial maternal serum levels of βHCG, progesterone and CA125 were determined. Further subdivision according to the gestational age within each age group was done. [6-7 weeks group: / 8-9 weeks group: / 10-11 weeks group]. This subdivision was done in an effort to limit the variability and increase the comparability of the results of the studied cases. Biochemical studies The level of B-hCG was estimated by a single sample at the time of ultrasound scan. Blood was collected by veinipuncture, allowed to clot and serum separated by centrifugation at room temperature. The sera were collected and stored in deep freeze (-70o C) to be assessed quantitatively when suitable. The technique used in the present work is the diagnostic kit prepared by Eurogenetics: Belgium (Headquarters Tessendrlo- Belgium) using βHCG Elisa coated microtiterstrips. Estimation of Progesterone in serum was carried out using the kit manufactured by Spectria Progesterone [I] 125 coated tube Radio immunoassay. (Orion Diagnostica Espoo, Finland). The technique is principally based on the widely used radioimmunoassay method. A sample containing an unknown amount of the substance to be assayed (unlabelled antigen) is added to a standard amount of a labeled derivative of the same antigen (labeled antigen). The labeled and unlabelled antigens are allowed to compete for the limited number of the high affinity binding sites of the antibody. After washing away the free (unbound) antigen, the amount of labeled antigen in the sample is inversely proportion to the concentration of unlabelled antigen. The actual concentration in unknown sample is obtained by means of a standard curve based on known concentration. Determination of Cancer antigen CA 125 was obtained by using a special kit for the detection of CA 125 based on a new antibody (monoclonal) that binds to CA 125 specifically. The quantitative determination is a one step immunoenzymatic assay (IEMA) based on the formation of a sandwich between the analyte to be detected and two specific monoclonal antibodies directed to different epitopes on the CA 125 molecules. Expected values for the test by the manufacturers in normal conditions are less than 37 IU/ml. in serum. Statistical analysis An IBM Compatible PC was used to store, manipulate and analyze the data obtained and to provide graphical representation of important results. Data were statistically described in terms of range, mean, standard deviation (±S.D.), median, mode and frequencies (number of cases) and relative frequencies (percentages). Comparison between different groups in the present study was done using Student t test for comparing continuous data when normally distributed and Mann Whitney U test when not normally distributed. For comparing categorical data, Chi square (X2) test was performed, Yates correction was used instead when the frequency is less than 10. A probability value (P value) less than 0.05 was considered significant. All statistical calculations were done using computer programs Microsoft Excel version 7 (Microsoft corporation, NY, USA)and SPSS (Statistical Package for the Social Science; SPSS Inc. Chicago, IL, USA) statistical program. RESULTSTwenty (100%) cases in group III were below the cutoff value for the serum B-hCG against 3 cases (15%) in group I with a highly statistically significant difference (P < 0.01). Hence, serum β-hCG showed a sensitivity of 100%, a specificity of 50%, a positive predictive value (PPV) of 50% and a negative predictive value (NPV) of 100%. Evaluation parameters regarding serum b-hCG in different gestational age groups are shown in table (1). Five (25%) cases in group III were below the cutoff value for the serum progesterone against 4 cases (20%) in group I with no statistically significant difference (P > 0.05). Hence, serum progesterone showed a sensitivity of 25%, a specificity of 78%, a PPV of 36% and a NPV of 67%. Evaluation parameters regarding serum progesterone in different gestational age groups are shown in table (1). Two (10%) cases in group III were above the cutoff value for the serum CA125 against 4 cases (20%) in group I with no statistically significant difference (P > 0.05). Hence, serum CA125 showed a sensitivity of 10%, a specificity of 65%, a PPV of 13% and a NPV of 59%. Evaluation parameters regarding serum CA125 in different gestational age groups are shown in table (1). Concerning the serum CA125 level, there were statistically significant differences between the control group and group II at 6-7 weeks and also between group II and group III at 8-9 weeks. DISCUSSIONIt is clinically important to predict the outcome of patients with history of recurrent abortion at an early stage of gestation. The prognostic predictive value of maternal serum CA125 measurement was investigated in different studies with conflicting results. In one study, the mean serum CA125 level of the patients with an unfavorable pregnancy outcome was significantly higher than that of the patients with a favorable outcome. When the cut-off level of maternal serum CA125 was taken as > 65 IU/ml in the first and > 60 IU/ml in the second measurements of the study group, the risk of termination of the pregnancy by spontaneous abortion was 83.3% in the patients with elevated serum CA125 levels (7). In another study, it was found that At 4 to 8 weeks of gestation the mean value for serum CA125 in patients with successful outcome was significantly higher than that in patients whoaborted. Although ultrasonographic examination is effective after 8 weeks of gestation, serum CA125measurement is useful in predicting early abortion (8). In the present study, the serum CA125 in the control group showed no significant differences between different gestational age groups (Table 1). The comparative data between the 3 groups showed a significant increase between group I and group II at 6-7 weeks and a significant decrease from group II to group III at 8-9 weeks (table 2). Serum CA125 showed a sensitivity of 10%, a specificity of 65%, a PPV of 13% and a NPV of 59% with best values at 10-11 weeks. On the other hand, in the present study, serum B-hCG showed highly statistically significant differences (P < 0.01) between the control mean value and that of the second and third groups at all gestational ages being highest in the control group and lowest in group III. Serum B-hCG showed a sensitivity of 100%, a specificity of 50%, a PPV of 50% and a NPV of 100% with relatively equal values in different age groups. This matches well with other investigators who found that the best predictor of ongoing pregnancy was βHCG concentration (5). In the present study, in the control group mean progesterone values were within the normal ranges described. Moreover, serum progesterone showed no significant difference in serum levels of women of different gestational ages in the control group. However, the level in group III was found to be significantly lower than in the control group (P<0.05) at 8-9 weeks. Serum progesterone showed a sensitivity of 25%, a specificity of 78%, a PPV of 36% and a NPV of 67%. The effectiveness of progesterone estimation obviously wouldn't depend only on absolute levels or even rising levels during pregnancy. At least, the effectiveness would also depend on endometrial and vascular bed receptivity to progesterone and probably also on the original basic structure of the tissue in question. (4). These data suggests that progesterone measurement is of some, but limited use in the assessment of early pregnancy complications and that a cutoff value on which we can evaluate 1st trimester pregnancies cannot be devised (9). In the present study, it is necessary to mention that sample size is a limiting factor (20 participants in each group). But it should always be kept in mind that it is not possible to identify the cause of the recurrent early pregnancy loss in approximately half of the cases and this could be the limiting factor for any biochemical marker (10). In conclusion, the value of CA125 in recurrent abortions is still unclear and cannot be recommended on routine basis. On the other hand β-HCG is highly sensitive as a single serum measurement for the prediction of pregnancy outcome. REFERENCES
Copyright © Middle East Fertility Society The following images related to this document are available:Photo images[mf05011t2.jpg] [mf05011t1.jpg] |
| |||||||||

{kind=link}
{kind=link}