 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
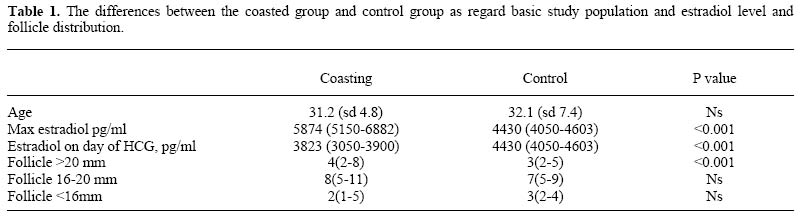
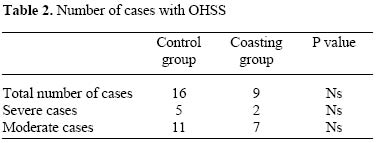
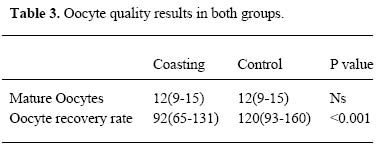
Effect of late coasting used in the prevention of ovarian hyperstimulation syndrome on oocyte quality Amany Shaltout, M.D., Amal Shohayeb, M.D., Adel Faruk, M.D., Mohamad Eid, M.D., Mona Mostafa, M.D., Ashraf Eldaly, M.D. Samir Abbas Medical Center, Jeddah, KSA. Received on October 10, 2004; Code Number: mf05013 ABSTRACTObjective: To detect the effect of late coasting on oocyte quality. Ovarian hyperstimulation syndrome (OHSS) is a potentially fatal iatrogenic complication of gonadotrophin administration used in IVF procedures (1) its incidence ranges from 0.5 to 10 % in all ovarian stimulation treatment cycles and up to 20% in high-risk cases (2). The factors leading to this syndrome have not been explained, it seems that there is release of vasoactive substances secreted by the ovaries under HCG stimulation, playing a key role in triggering this syndrome. The hall mark of this condition is a massive fluid shift resulting in profound intravascular depletion and haemoconcentration. (3). Risk factors for developing OHSS include PCOS, young (less than 35 years), lean patients, with high serum estradiol levels. Several methods for preventing ovarian hyperstimulation syndrome or reduce its side effects has been suggested, one of which is coasting. Coasting means withholding gonadotrophins whilst continuing GNRH administration for pituitary down regulation until serum E2 concentrations drop below a given threshold (4). The reported efficacy has not been uniformly consistent probably due to different criteria to apply coasting with estradiol rise more than 3000 pg/ml - 6000 pg/ml, or leading follicle size ranging from 16 mm to 20 mm with a coasting duration ranging from 1-11 days (5). The coasting strategy reduces or entirely avoids the need to abandon the cycle or cryopreserve all the embryos, reduces the cost, and patient distress (6). The fall in estrogen during coasting may be due to partial atresia of granulosa cells (7) as granulosa cells are more susceptible to gonadotrophin withdrawal and atresia than are developing oocytes (8). Additionally FSH has been demonstrated to be a potential inhibitor of granulosa cell apoptosis, therefore, by withdrawing FSH, apoptosis may be enhanced (9). Coasting popularity is probably related to its simplicity rather than to definite evidence to its efficacy. It has been suggested that atresia occurring during prolonged coasting maybe associated with impaired outcome of IVF treatment (10). The aim of this study is not only to detect the efficacy of coasting in the prevention of OHSS but mainly also to detect the effect of coasting on oocyte quality. MATERIALS AND METHODSOur study is a retrospective study in which data was collected for IVF patients attending Dr Samir Abbas Medical Center, (Jeddah) during the period between 1-10 -2002 till 30 - 9- 2003.The patients were divided into 2 groups, including Group 1 coasting group consisting of 86 patients, while Group 2 control group consisting of 100 patients In both groups, pituitary desensitization by GNRH agonist (Decapeptyl, Ferring, Germany) starting from mid luteal phase of preceding menstrual cycle then gonadotrophins 2-4 ampoules/day (Menogon 75 I.U., Ferring, Germany) was initiated when serum estradiol level was less than 50 pg/ml, dose was adjusted according response. When at least 2 follicles reached 18 mm in diameter, HCG (Pregnyl Organon, Netherlands,) 10,000 I.U. was administered intramuscular. In the coasting group, coasting was applied when estradiol level was more than 4000 pg/ml with 30% of follicles more than 18 mm in diameter. Daily measurement of estradiol was done till it became less than 4000 pg/ml the HCG was given and oocytes retrieved after 32-38 hours. The coasting duration was up to 3 days, as all patients had decrease in estradiol level to less than 4000 pg/ ml by that time. Intracytoplasmic sperm injection was performed in both groups. The oocyte recovery rate was defined as the total number of oocytes obtained divided by the number of follicles having the diameter of at least 16 mm on the day of HCG administration. Oocyte maturity was diagnosed by the extrusion of the first polar body, with a fluffy expanded cumulus; corona radiata still associated to the zona and with a clear or sometimes homogenously granulated cytoplasm. Ovarian hyperstimulation syndrome was diagnosed according to the classification of Golan et al 1989, including it as early and late onset moderate and severe OHSS (11). Differences between coasted group and control group were assessed using student t test, logarithmic transformation of variables was performed in order to normalize distribution, other wise, nonparametric tests was used, including Microsoft excel, results are expressed as a mean with standard deviation or as a median with percentile range of 25%-75%). RESULTS As regard the age distribution, there was no statistical significance with, a mean of 31.2 for the coasting group and 32.1 for the control group, yet the maximum estradiol level in the coasting group was 5874 pg/ml as a median which is high in comparison to that of the control group which has a median of 4430, with a p value of less than 0.001. However, the estradiol level on the day of administration of HCG in the coasting group has a median of 3823, which is lower than that of the control group, which has a median of 4430 with a p value of less than 0.001 (Table 1). As regard the folliculometry in both groups especially in measuring follicles more than 20 mm, difference between both groups was statistically significant with a median of 4 in the coasting group and a median of 3 in the control group. Yet the follicles from 16-20 mm and those less than 16 mm. There was no statistical significance between both groups. As regards the incidence of OHSS, only 9 patients developed OHSS, 7 of which was moderate, and only 2 severe cases in the coasting group, while 16 patients developed OHSS in the non coasted group, 5 of which were severe and 11 moderate cases. Although the number of OHSS patients was less in the coasting group, yet this difference was not statistically significant (Table 2). Number of mature oocytes was identical in both groups However, the oocyte recovery rate was significantly higher in the control group (120) than the coasting group (92) as shown in table 3. DISCUSSIONOvarian hyperstimulation syndrome (OHSS) is the most serious complication of ovarian stimulation and its severe form can even be life threatening. Due to the availability of GnRH agonists in the last two decades, and with the resulting lack of feedback from the down-regulated pituitary, this has led to cases of exaggerated overstimulation of the ovary. The prerequisite for development of the syndrome is the triggering of ovulation with exogenous HCG, while the condition is further aggravated by endogenous HCG in cases where pregnancy occurs. Few approaches singly or in combination, can be taken in an attempt to avoid OHSS. Among them are: decreasing the amount of exogenous HCG (12), using GnRh agonists for triggering of ovulation (13), canceling the cycle by aspirating follicular contents prior to HCG administration (14), aspirating oocytes after ovulation induction but withholding embryo transfer (15), intravenous albumin injection on day of oocyte retrieval (16,17) and withholding gonadotrophins whilst continuing GNRH administration for pituitary down regulation until serum E2 concentrations drop below a given threshold, termed coasting (4). In our study late coasting was used to prevent OHSS .Our coasting duration was up to 3 days, yet the mean duration of coasting in other series, was shorter than 2 days (18,19), while others, was shorter than 3 days (10,20,21). Although coasting was associated with significant high serum estradiol level and increased number of follicles, however OHSS occurred in only 11 % of coasted population yet other studies showed that the incidence of OHSS in a high-risk population was between 20 % and 80 % (22,23). This means that coasting did effectively reduce the incidence of OHSS. We observed that coasting is associated with greater number of large follicles but a lower oocyte recovery rate than in the control group this can reflect the alteration in the oocyte -cumulus complex development with fall in estradiol level. These results agree with those of Egbase et al 1999 (14), and Dhondt et al, 1998 (19), which found the same results. In our study, this arrest in development was documented but it did not affect oocyte quality as the number of mature oocytes were the same in the two groups. These results agree with other studies (10,14,19). In spite of the smaller number of oocytes retrieved than follicles visualized. Yet these oocytes are of good quality which can be explained by the fact that large follicles contain more FSH receptors continue to enlarge despite coasting to yield more mature oocytes (14). CONCLUSIONCoasting is an effective approach for the prevention of OHSS without adverse effect on oocyte quality and should be applied in cases at high risk of developing OHSS and without the need to cancel the cycles. REFERENCES
Copyright © Middle East Fertility Society |

{kind=link}
{kind=link}
{kind=link}