 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Middle East Fertility Society, Vol. 10, No. 1, 2005, pp. 72-77 Role of oocyte morphology on fertilization and embryo formation in assisted reproductive techniques Mohammad A. Khalili, Ph.D.*, Mahdieh Mojibian, M.D.†, Abdul-Munaf Sultan, Ph.D.‡ Fertility & Infertility Research Center, Isfahan University of Medical
Sciences, Isfahan and Department of Obstetrics & Gynecology, Yazd University
of Medical Sciences, and Dr. Mojibian Hospital, Yazd, Iran; and ART Center,
Qatar Women's Hospital, Qatar Received on August 7, 2004; Code Number: mf05014 ABSTRACTObjective: To assess the influence of MII oocyte morphology on the
fertilization outcome and embryo development in ART cycles. Since, age may
affect the quality of oocyte, the role of women's age was also evaluated following
IVF or ICSI cycles. Key Words: Oocyte morphology, Human Embryo, IVF, ICSI, Infertility In assisted reproductive treatment programs, controlled ovarian hyperstimulation for multiple follicular development has become widely used. This allows the recovery of numerous preovulatory oocytes for ART treatment program (1). The influence of metaphase II oocyte quality on the outcome of IVF as well as ICSI programs has already been studied, however with controversial results (2-4). Serhal et al. (1997) reported that retrieval of mature oocytes with normal morphology is correlated with better embryo development and implantation rates in ICSI procedure (2). While, others have demonstrated that oocyte quality or morphology has small impact, if any, on embryo development and implantation potentials (4). Effort has been made to correlate the morphological quality of oocytes to the successful outcome of ART treatment cycles. Veek (1988) reported that good quality MII oocytes should contain the morphological features of clear, moderately granular cytoplasm, a small PVS, and a clear ZP (6). Morphological anomalies in oocytes retrieved from ART cycles have been studied by several investigators (2, 6-9). These include: fragmented PB, wide PVS, non-spherical shape of oocyte, anomalies in ZP layer, cytoplasmicgranulation, vacuolated ooplasm, and refractile bodies. The main objective of this prospective study was to assess the influence of MII oocyte morphology on the success rates of fertilization and embryo development from conventional IVF and ICSI cycles. Since, age may affect oocyte quality, the role of women's age in fertilization and embryonic development was evaluated following IVF or ICSI cycles. MATERIALS AND METHODSPatient Selection
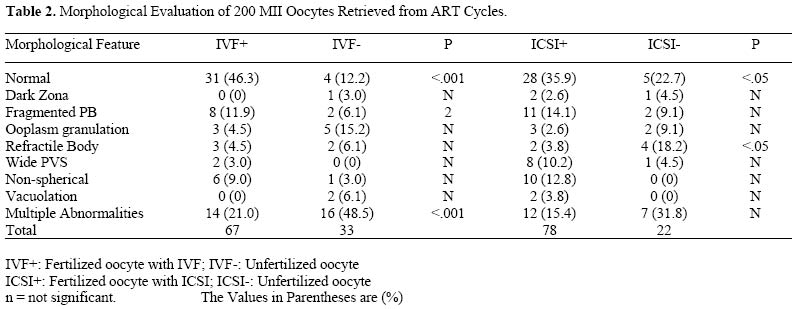
In this prospective clinical trial study, the morphological feature of 200 metaphase II oocytes from 30 IVF and ICSI cycles were evaluated and compared. In addition, the morphology of oocytes that were fertilized in IVF cycles (IVF+) was compared with failed fertilization (IVF-). The oocytes were similarly categorized in the ICSI procedure (ICSI+ and ICSI-). Patients chose to undergo conventional IVF treatment because of tubal infertility; while the ICSI group consisted of patients with male factor infertility. Couples with other forms of infertility were excluded from this study. All females were <40 years old. In all patients, controlled ovarian hyperstimulation was carried out with human menopausal gonadotrophin (hMG, i.m.), followed by the injection of 10,000 IU of human chorionic gonadotrophin (hCG, i.m.). The ovarian response was monitored by serial transvaginal and serum estradiol concentration. Transvaginal ultrasound-guided oocyte retrieval was performed approximately 36 hr post hCG injection. Semen Analysis and Sperm Preparation Semen analysis was done according to WHO criteria (10) Sperm count and motility were evaluated using Makler Chamber and light microscopy at x200 magnification. Motility was expressed as a percentage of progressive and non-progressive spermatozoa. Geimsa staining was used for evaluating sperm morphology. All sperm preparations were performed using the swim-up technique (11). Briefly, 1ml of semen was mixed with 3ml of Ham's F10 medium (Seromed Co., Germany) supplemented with serum substitute substance (SSS, Irvine Scientific Co, USA). After gentle mixing, the sample was centrifuged twice (2,000 rpm for 10 and 5 min, respectively). Following the removal of the supernatant, 0.2-1.0 ml of the culture medium was added depending on the size of the pellet and the quality of the original sample. The suspension was then incubated at 37C in 5% Co2 until use. IVF Procedure Following retrieval, the oocytes were cultured individually in droplets covered with washed mineral oil (Sigma Co., USA) at 37 C in 5% Co2 for 4-5 hr. The oocytes were inseminated with about 100,000 sperms with progressive motility. After incubation for 2 h, the corona cells were removed using drawn-out Pasture pipettes. Following evaluation, each oocyte was then transferred individually into 100 droplets of culture medium overlaid by mineral oil and was incubated at 37oC in 5% Co2 (Forma Scientific Co., USA). Fertilization of each oocyte was checked and recorded 15-18 hr after insemination that was confirmed by presence of two pronuclei. Fertilized oocytes were transferred individually into fresh culture medium (12). ICSI Procedure ICSI protocol was done as previously described (12-13). Following semen analysisand sperm preparation as described for IVF procedure, the samples were incubated until use. The oocytes were incubated for 4 hr and then denuded from cumulus cells using 80 iu hyaluronidase/ ml (Sigma Chemical Co., USA) along with mechanical aid of Pasture pipettes. Each of the MII oocyte was rinsed in culture media and then the morphological features were evaluated as described for IVF group. Thereafter, each oocyte was injected with a mechnically immobilized spermatozoan as described elsewhere (12). The injected oocytes were rinsed twice and then placed individually in fresh droplets covered with mineral oil. They were then incubated followed by fertilization evaluation as described for the IVF protocol. Both IVF and ICSI procedures was performed by the same embryologist (M.K.). Oocyte Evaluation The morphological feature of each oocyte was evaluated with the aid of inverted microscope. The criteria employed for the morphological evaluation of oocytes were: a. normal oocytes showed clear cytoplasm with homogenous fine granularity; b. granular oocytes, dark with granularity either homogenous in whole cytoplasm or concentrated in the central portion of oocyte; c. cytoplasmic inclusions comprised vacuoles presumed to be of endocytotic origin; d. anomalies of ZP, e. fragmented polar body of different sizes; f. non-spherical shape of oocyte; and g. wide PVS. Embryo Evaluation and Transfer
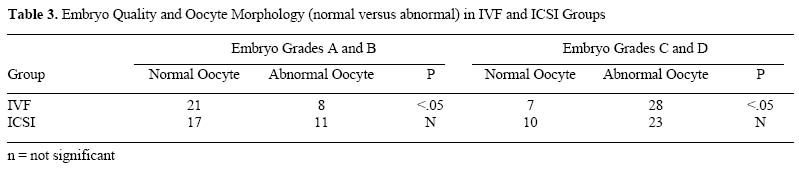
Approximately 48 hr after insemination/ injection, the cell number and morphology of each embryo were scored according to Hill et al. (14). The grading was as follows, Grade A: equal size blastomeres without fragmentation, Grade B: slightly unequal blastomere, up to 10% cytoplasmic fragments. Grade C: unequal sized blastomeres up to 50% fragments and large granules. Grade D: unequal blastomeres with significant fragmentation and large black granules. Day 2 embryos were transferred to respective patients according to the guidelines of the American Society of Reproduction. Excess good quality embryos were cryopreserved. Statistical Analysis Data are presented as means ± standard deviation. For statistical analysis the χ2 and Fisher's exact tests were used. Statistical significance was set at p<0.05. RESULTSThe mean age of the women was 30.0±3.9 years (18-38) for IVF group and 29.9±4.2 years (22-39) for ICSI patients. Also, duration of infertility in both groups of IVF and ICSI was similar (10.2±3.9 years versus 10.0±3.4 years). Table 1 shows the percentage of normal as well as abnormal oocytes in two age groups of women <30 and >30 years old. The results showed that there was a significant difference between total number of normal and abnormal oocytes in failed fertilization in IVF and ICSI cycles. Table 2 demonstrates the morphological features of 200 MII oocytes retrieved from 30 ART cycles. A total of 67 and 78 oocytes were fertilized in IVF and ICSI cycles, respectively. 46.3% and 35.9% of fertilized oocytes were shown with normal morphology in IVF and ICSI cases, respectively. There were no differences between the IVF and ICSI groups in terms of mean number of embryos transferred (3.3±0.4 versus 3.0±0.9). In IVF+, fragmented PB was the highest rate of single abnormality with 10.9%, while cytoplasmic granulation was the least type of morphological abnormality. Also, multiple abnormalities were observed in 21.0% and 48.5% of oocytes in IVF+ and IVF-, respectively (P<.001). In addition, 15.4% and 31.8% of the oocytes from ICSI+ and ICSI- were presented with more than one abnormality. In ICSI+, 35.9% of the oocytes presented with normal morphology; while, 22.7% of the oocytes in ICSI- showed normal morphological feature (P<.05). The highest rate of single abnormality in ICSI+ was fragmented PB (14.1%). In addition, the abnormalities such as vacuolation, or non-spherical shape were not observed in any oocytes in ICSI- group. However, refractile bodies were the highest type of single abnormality (18.2%) in ICSI- group (Table 2). Table 3 presents the embryo quality in relation to oocyte morphology (normal versus abnormal). It demonstrates that in ART cycles, the highest rates of good quality embryo formation (grades A & B) were obtained from oocytes with normal morphology. DISCUSSIONControlled ovarian stimulation protocols produce oocytes of great heterogeneity in both number and quality (1). Now-a-days, skillful embryologists have the tools to assess the oocyte quality during IVF and ICSI treatment programs. However, oocyte quality and its influence on fertilization rate and embryo development is still a matter of controversy in ART cycles. Kahraman and colleagues (2000) reported oocyte morphology to be an important prognostic factor in the successful treatment of ICSI cases (7). In contrast, De Sutter et al. (1996) observed no correlation between oocyte morphology and fertilization success rate in ICSI program (4). Therefore, this study was undertaken to evaluate the relationship between the oocyte morphology and fertilization rate/ embryo development in both IVF and ICSI. Also, oocyte morphological features were evaluated and compared in both fertilized as well as unfertilized oocytes from ART cycles. In addition, role of women's age in fertilization success rates following IVF or ICSI treatments was assessed as well. The results generated from our IVF cases demonstrate that ooplasm granulation was the most single abnormality observed in failed fertilization oocytes. This may be due to the fact that only patients with female factor infertility underwent IVF cycles. We have also shown that oocytes with vacuoles in cytoplasm can have normal fertilization. However, the highest rates of abnormalities in this group were related to multiple morphological abnormalities in oocytes. This may indicates that in general oocytes with multiple abnormalities are related with higher rates of failed fertilization in IVF. In addition, our results clearly showed that oocytes with normal morphology not only significantly improve the fertilization and cleavage rates, but also involve with generating good (grades A & B) cleaving embryos in ART program. Another finding was the refractile bodies that were the most single anomaly found in ICSI with failed fertilization. These structures were assessed by Veek (1991), who suggested a poor prognosis with very low fertilization in IVF cycles in affected oocytes (4). We have demonstrated that some oocytes with refractile bodies can achieve normal fertilization. However, their number was higher in oocytes with failed fertilization. In addition, over 31% of failed fertilizations in ICSI cases were shown with multiple abnormalities. Some have reported that oocyte abnormalities such as vacuolization, fragmented PB, and refractile bodies were found to correlate with lower fertilization and cleavage rates (15, 16). In addition, Kahraman and associate (2000) noticed that cytoplasmic granulation was involved with lower implantation and on-going pregnancy. Cytoplasmic granulation may develop from stimulated cycles (7). Therefore, a comparable study comparing the rate of granulation in oocytes derived from stimulated with unstimulated natural cycles may explain their role in ART success rates. De Sutter et al. (1996) study supported ours that oocytes with normal morphology represent only one-third of all collected oocytes. In other words, more than half of the oocytes showed some type of morphological anomalies (4). Recently, cytoplasmic fragments in PVS have been also investigated by Farhi et al. (2002). They noted that while fertilization rate and embryo quality were not affected, but significant reduction in pregnancy rates and implantation were occurred in oocytes with fragments in the PVS (8). Also, the relationship between PB morphology and 70 consecutive ICSI results was investigated by Ebner et al. (2000). In contrast to our data, they observed a significant correlation between non-fragmented PB morphology and high fertilization rate and embryo quality. They also reported 84 oocytes with refractile bodies, 17 with irregular shape, 159 fragmented PB in 538 eggs from ICSI cycles. Also, 300 oocytes showed no anomalies at all. The role of PB morphology was further investigated by Ciotti et al. (2004) in ICSI cases with male infertility. They noticed that PB fragmentation was not related to the fertilization rate, embryo quality, or implantation potentials (17). In addition, the results generated from our study showed that age factor is probably responsible for the higher rates of morphological abnormalities of oocytes in women over the age of 30 years. The above findings indicate the adverse effects of age on the success rates of ART treatment. Our findings support that the age of patients undergoing ART is related with the quality of oocytes as well as fertilization rates. This correlation has been also supported by Lee and associates (2001), who observed that women's age correlates with oocyte quality as well as fertility potentials (18). Selva et al. (1991) reported that 30% of unfertilized oocytes demonstrated abnormalities in numerical chromosomes (19). Therefore, the possible relationship between oocyte ability to fertilize and chromosomal abnormalities need to be further elucidated in clinical setting. Furthermore, the genetics of oocytes with normal morphology should be compared with each type of morphological abnormalities in oocytes after ART cycles. In conclusion, the present data indicate that oocyte quality should be considered as one of the main parameters in ART setting. This was shown by a significantly higher fertilization rates and good quality embryo formation from oocytes with normal morphology in young patients undergoing ART. Also, our findings suggest that multiple abnormalities were observed in almost half and one-third of failed fertilization following IVF and ICSI, respectively. Therefore, the quality of MII oocytes plays a significant role in fertilization process as well as cleaving embryo formation. ACKNOWLEDGEMENTThe authors would like to thank Dr. Jaffar Ali from Qatar women's hospital for his critical review of this manuscript. REFERENCES
Copyright © Middle East Fertility Society The following images related to this document are available:Photo images[mf05014t3.jpg] [mf05014t2.jpg] [mf05014t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}