 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Middle East Fertility Society Journal, Vol. 10, No. 2, 2005, pp. 116-124 Ultrasonically diagnosed polycystic ovaries in asymptomatic women with normal hormonal profile does not affect their fecundity Amal Shohayeb, M.D., Amany Shaltout, M.D. , Adel Farouk, M.D., Mohamed Eid, M.D., Mona Mostafa, M.D., Akmal Elmazny, M.D. Department
of Obstetrics and Gynecology, Faculty of Medicine, Cairo University, Cairo,
Egypt Received July 4, 2004; revised and accepted August 23, 2004 Code Number: mf05022 ABSTRACT Objective: To evaluate the effect on fertility of
ultrasonically diagnosed polycystic ovaries in asymptomatic women with normal
basal hormonal profile. Key Words: Infertility, polycystic ovaries, polycystic ovarian syndrome, three dimensional ultrasonography. Polycystic ovary (PCO) syndrome is a very common endocrine disorder. Among women who present with oligomenorrhoea, 87% have PCO, and, of women with regular menstrual cycles who present with hirsutism, 92% have PCO (1,2). Over 50% of patients who presents with recurrent miscarriage have PCO (3). Despite a large amount of epidemiological, clinical, laboratory and experimental studies, the etiology and pathophysiology of the syndrome remains still fragmentary obscure and probably multifactorial (4). Polycystic ovarian syndrome may result from disturbances of various endocrine systems but there is increasing evidence that PCO is an oligogenic disorder, with the interaction of a small number of key genes with environmental factors determining the clinical and biochemical manifestations (5,6). There is a wide spectrum of clinical and biochemical features associated with polycystic ovary syndrome which span the spectrum from the presence of PCO only to the syndrome characterized by obesity, hyperandrogenism, menstrual disturbance, and anovulatory subfertility, that is, Stein-Leventhal syndrome (7,8). Menstrual disturbances with the syndrome included, oligomenorrhea (40 days or longer between the menstrual periods), amenorrhea (absence of menstruation for > 3 months without being pregnant), or erratic bleeding (loss of the cyclic menstrual pattern) (7,8). A range of endocrine disturbances including serum LH levels that are disproportionately higher than FSH levels, raised estrogen levels, low sex hormone-binding globulin levels, hyperinsulinemia, and hyperandrogenemia are common (14,15), but not essential diagnostic features of the syndrome (16). Using ultrasound scanning techniques, the diagnosis of PCO is generally made when the ovaries appear enlarged with increased ovarian stroma and volume with thickened capsule (13) and contain > 10 cysts, each < 10 mm in diameter scattered around or through an echodense thickened stroma (9,10). The recent advent of three-dimensional ultrasonography allows more accurate detection of uterine and ovarian structures (11,12). Stroma and volume determinations can be obtained more accurately than by traditional ultrasonography. Three-dimensional ultrasonography not only facilitates noninvasive evaluation and volume calculation but also completes the examination in a short time without increasing patient discomfort (13). The volume measurement in 3D ultrasonography is accurate and highly reproducible. The volume of the follicle can be determined precisely and the volume of the ovary from 3D ultrasonography correlates better with direct measurement of the surgical specimen than that from 2D ultrasonography (13). The diagnostic criteria of polycystic ovary syndrome remain debatable because of its heterogeneity (17,18). Ovarian morphology, as detected by scanning has been suggested to be the most sensitive marker of the syndrome (19, 20), but many women who have PCO appearance do not have features of the syndrome (21), and not all of those who appear clinically to have the syndrome have the ultrasound appearance of PCO (22). PCO appearances is found in 21%-33% of women of reproductive age depending on ultrasound criteria (23-27), while estimates of the incidence of polycystic ovary syndrome vary between 4% and 10% (28-30), depending on the criteria used for anovulatory subfertility (31). As anovulation accounts for 20% of cases of subfertility (32) that occur in 15% of the couples of reproductive age (33), <3% of the women of reproductive age develop anovulatory subfertility because of the syndrome despite the high incidence of PCO, so the incidental finding of PCO appearance in asymptomatic women is not uncommon (34). The impact of polycystic ovary syndrome on reproductive and general health is well known (35,36), but the effect of PCO appearance without features of the syndrome is unclear. This study aimed to evaluate the detrimental effect on fertility of the ultrasonically diagnosed PCO in women who have no symptoms of polycystic ovary syndrome with normal basal hormonal profile. MATERIAL AND METHODS During the period from February, 2000 to April, 2002, 96 patients planning to get pregnant presented to Gynecology clinic at Samir Abbas Medical Center, scanned for pre-conceptional evaluation without any gynecological or endrocinogical complaints, were enrolled in this study. The duration since the last delivery ranged between 18-32 months History was taken from the selected women regarding their menstrual pattern, previous pregnancies, features of pco (menstrual disturbances, obesity acne or hirsutism) and health related problems to PCO (diabetes mellitus, hypertension, lipid abnormalities, and cardiovascular disease) Inclusion criteria for all patients included;
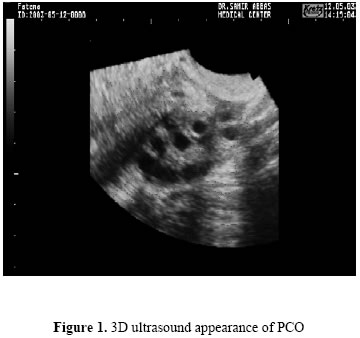
Informed consent was obtained from each patient in this study. None of them had received any ovarian hyperstimulation regimen or steroid hormone within 6 months before ultrasonographic evaluation. Two dimensional ultrasonography scanning was performed using a 7.5-MHz transvaginal transducer (Medison, Voluson 530D, Kertz, Austria), cases with enlarged ovaries where scanned with three dimensional ultrasonography using a 7.5-MHz transvaginal transducer (Medison, Voluson 530D, Kertz, Austria) for proper evaluation of the ovarian volume. The scanning was performed by one sonographer to avoid the inter observer variability. Three rotatable perpendicular planes of bilateral ovaries could be displayed simultaneously to obtain the largest dimensions, the 3 D volume was measured using the formula for a trapezoid. At the same time, the number of follicles in one section allowed an accurate diagnosis. Once the largest area of the ovary was localized, the distance (one dimension), area (two dimensions) and volume (three dimensions) were calculated. The stroma, cystic areas, and total ovarian areas were measured by outlining meticulously the regions of interest. The volume of the ovary was measured by outlining the areas of multiple parallel sections at different distances from the ovary and was calculated using trapezoid formula. At least 10 serial slices were taken across the ovary for volume measurements. The specific ultrasound diagnosis of PCO was based on Kurjak classification 1994 (4) depending upon visualization of enlarged ovaries (ovarian volume ≥12 cm3) with >10 cysts in a single plane, each measuring <10 mm in diameter scattered around or through an echo-dense thickened stroma (Figure 1, 2). Cases where the number or diameter of the cysts or the appearance of the stroma did not fit these criteria were excluded. Table 1. Age (years), weight (kg), height (cm) and body mass index (BMI) of both groups
Of the study and the control group 7 cases has been lost in the follow up period, 2 cases changed their plans and used contraceptive methods and 7 cases started to use induction of ovulation, 70cases only completed the follow up period. Two subgroups were identified;
Patients were followed for up to 12 months to determine Time to pregnancy (TTP), defined as the time of exposure to regular unprotected intercourse till conception, which was used to measure fecundity. Data were statistically described in terms of range, mean, standard deviation (SD), and median. Comparison between different groups in the present study was done using Student t test for comparing continuous data when normally distributed and Mann Whitney U test when not normally distributed. A probability value (p value) less than 0.05 was considered significant. All statistical calculations were done using computer programs Microsoft Excel version 7 (Microsoft Corporation, NY, USA) and SPSS (Statistical Package for the Social Science; SPSS Inc., Chicago, IL, USA) statistical program. RESULTS Seventy patients planning to get pregnant were included in this study. 3D ultrasound showed features of PCO only in 35 cases the others 35 showed no ultrasound features of PCO. Statistical evaluation of the results of both groups showed no significant statistical difference between study group and the control group concerning; age (29.3±4.9 versus 29.4±4.8 years), weight (70.6±14.9 versus 75.7±9.5 kg), height (160.3±4.6 versus 162.1±5.9 cm) or body mass index (BMI) (27.5±5.6 versus 28.9±4.5), (Table 1). There was no significant statistical difference between study group and the control group concerning; Duration of marriage (4.4±3.5 versus 4±2.9 years), parity (1.2±1.4 versus 1.4±1.5) or number of abortions (0.7±0.9 versus 0.7±1), (Table 2). Table 2. Duration of marriage (years), parity and number of previous abortions of both groups
Table 3. Duration of menstrual flow (days), length of menstrual cycle (days) of both groups
There was no significant statistical difference between study group and the control group concerning; Duration of menstrual flow (5.3±1.4 versus 5.1±1 days), length of menstrual cycle (28.5±1.3 versus 27.3±3.8 days) (Table 3). There was no significant statistical difference between study group and the control group concerning the following hormones; serum FSH day 2 (5.8±1.7 versus 6.3±1.3 mIU/ml), serum LH day 2 (4.3±2.2 versus 4.6±2.1 mIU/ml), serum E2 day 2 (55.1±18.9 versus 48.9±13 pg/ml) (Table 4). The right and left ovarian volumes of the study group (28.8±8.5 and 28.6±4.9 mm3 respectively) were significantly higher than right and left ovarian volumes of the control group (8.1±1.7 and 7.5±1.5 mm3 respectively) (Table 5). TTP of the study (PCO) group was not significantly longer than the control group (6.7±3.2 versus 8.1±3.3 years). Without symptoms or endocrine disturbances of polycystic ovary syndrome, polycystic ovarian appearance has shown not to have significant detrimental effect on fertility (Table 6). DISCUSSION There are different definitions for PCO. PCOS is defined by chronic anovulation plus clinical or biochemical signs for hyperandrogenism with exclusion of other etiologies (79). Recently the Rotterdam revised diagnostic criteria for PCO include (2 out of 3), oligo and/or anovulation, clinical and/or biochemical signs of hyperandrogenism, polycystic ovaries and exclusion of other etiologies (congenital adrenal hyperplasia, androgen secreting tumor, Cushing's syndrome) (79). Polycystic ovary syndrome is a heterogeneous disorder. A wide range of reproductive problems (oligoamenorrhea, subfertility, endometrial carcinoma [37]) has been associated with polycystic ovary syndrome. General health problems (diabetes mellitus [38] hypertension, lipid abnormalities [39,40], and cardiovascular disease [41-43]) are also common, and the impact of the syndrome on the woman's quality of life and psychological status may be profound (44-46). The appearance of PCO on ultrasound scanning is common. Only a fraction of those with PCO appearance, however, have the clinical or endocrine features of polycystic ovary syndrome (47, 48). It is, therefore, essential to evaluate the effects on fertility and long-term consequences when PCO appearance is incidentally found in asymptomatic young women. A hospital population was used because the study was designed in a way to simulate the common clinical scenario when PCO appearance is incidentally found in women scanned for reasons irrelevant to polycystic ovary syndrome. Strict criteria were used for selecting the study group, and women in the control group were selected in a way that would ensure randomization. Table 4. Day 2 serum FSH(mIU/ml), day 2 serum LH(mIU/ml), day 2 serum E2(pg/ml) of both groups
Table 5. Ovarian volume (3 mm) between of both groups
TTP was used to measure the effect on fecundity (49). More women with PCO than normal ovaries, however, are expected not to have conceived and the effect on TTP could be flawed (50, 51). Thus, the subfertile proportions in both groups were compared to ensure actual evaluation of the effect. In this study, the appearance of PCO has been shown to have no significant impact on fertility in asymptomatic women with normal basal hormonal profile. The TTP of women with PCO was not significantly longer and they were not more likely to be subfertile than women with normal ovaries. Clayton et al. (24) suggested that PCO should not necessarily imply altered fertility potential. This has been substantiated in our study, which further leads to the conclusion that appearance of PCO without features of the syndrome are not associated with a detrimental effect on fertility and that an effect appears only when the combination of PCO appearance and symptoms exists. In a study by Hassan and Killick (52), comparing the effect of symptomatic disease on fecundity in women with PCO and those with normal ovaries, significant reduction in fecundity was detected only when PCO appearance was associated with the symptoms of the syndrome. Similar symptoms in women with normal ovaries were not found to be associated with a significant effect on fecundity. Without such symptoms, women who had PCO appearance were not found to be less fecund than those with normal ovaries. Furthermore, Hassan and Killick (52) concluded that prolongation of the TTP with increasing number of symptoms in women with PCO appearance would indicate that the effect of symptomatic disease on fecundity is progressive with its severity. The absence of a similar effect in those with normal ovaries would confirm that the detrimental effect on fecundity occurs only when PCO appearance and symptoms coexist. A higher prevalence of symptoms in subfertile women with PCO appearance would confirm the association of such symptoms with reduced fertility in these women, while the absence of a similar finding in subfertile women with normal ovaries would confirm the specificity of such an association with women with PCO. It is necessary to differentiate between the mere presence of PCO appearance and its association with the clinical or endocrine features of the syndrome. Universally acceptable definitions of PCO and polycystic ovary syndrome are yet to be agreed upon (53). In the 1990 conference of the National Institute of Child Health and Human Development on polycystic ovary syndrome (54), the attempt to establish more specific criteria for the syndrome had limited success, largely because of the lack of understanding of its pathogenesis and the diversity of its presentation. Universally approved diagnostic criteria are necessary so that results from various studies can be compared, which may lead to a better understanding of the syndrome. Despite the well-known long-term consequences, women with the syndrome tend to be inadequately treated (55). The current ultrasound criteria of PCO (56), which still very much in use (57, 58), do not seem to be a specific marker for the syndrome. Table 6. TTP (years) between the study group and the control group
Prerequisites for ultrasound diagnosis of PCO need to be reset (59). More restrictive criteria such as a higher number of cysts with more objective assessment of the stromal thickness and ovarian volume should be used (60-64). Furthermore, it has been shown that the ultrasound appearances of PCO have limited predictive value for the endocrine parameters (65, 66). Inclusion of such biochemical criteria as diagnostic prerequisites of the syndrome is, therefore, necessary to reflect its pathological features (67-69). For example, high LH level (70, 71), hyperinsulinemia and high free androgen levels (72, 73) in women with polycystic ovary syndrome closely correlate to the clinical symptoms (74, 75). Whether the isolated finding of PCO in normal ovulatory women, without any of the clinical or endocrine features of the polycystic ovary syndrome, is a normal variation (26) or an intermediate stage between normality and the syndrome (76, 77) remains controversial (78). A follow-up study of asymptomatic women with PCO appearance is, therefore, recommended to estimate their risk of developing the syndrome and the long-term effect on fertility. CONCLUSION Without symptoms or endocrine disturbances of polycystic ovary syndrome, PCO appearance has been shown not to have a significant detrimental effect on fertility. Appearances alone are not indicative of the clinical or endocrine features associated with polycystic ovary syndrome, and additional diagnostic criteria should be considered. More studies on the association of hormonal disturbances with symptoms in women who have PCO and the effect on their fertility are required. The incidental finding of PCO appearance in otherwise asymptomatic healthy women should not be considered as a sign of reduced fertility. Longitudinal follow-up studies of these women are recommended to evaluate the effects on future fertility and long-term consequences. REFERENCES
© Copyright 2005 - Middle East Fertility Society The following images related to this document are available:Photo images[mf05022f2.jpg] [mf05022f1.jpg] | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| |||||||||

{kind=link}
{kind=link}