 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Middle East Fertility Society Journal, Vol. 10, No. 2, 2005, pp. 142-149 Characteristics of polycystic ovary syndrome with and without insulin resistance and the role of insulin sensitizing drug (metformin) in its management Ashraf M. N. Refaie, M.D., M.R.C.O.G. *, Gehan A. K. Ibrahim, M.D.†, Saad Al Oash, M.D.‡ Departments
of Obstetrics and Gynaecology, Internal Medicine, and Clinical Pathology, Zagazig
University, Egypt Received January 8, 2005; revised and accepted March 13, 2005 Code Number: mf05026 ABSTRACT Objectives: To define the clinical and biochemical
characteristics in polycystic ovary syndrome (PCOS) patients with and without
insulin resistance (IR); and to evaluate the role of metformin as an insulin
sensitizing drug in infertile IR PCOS patients with regard to both reproductive
and metabolic functions. Key words: Polycystic ovary, insulin resistance, insulin sensitizing drugs Polycystic ovary syndrome (PCOS) occurs in approximately 4% to 6% of the female population and may be the leading cause of infertility in those of reproductive age. PCOS presents clinically with a variety of signs and symptoms; the most common being menstrual irregularities, hyperandrogenism, infertility, and obesity. The true pathophysiology has not been clearly elucidated; however, there is growing agreement that gonadotropin dynamic dysfunction, hyperandrogenism, and insulin resistance (IR) are key features (1). PCOS is not a benign condition. It may lead to complications involving glucose metabolism, type 2 DM, dyslipidemias, cardiovascular disease, and endometrial cancer. The goals of treatment should focus on restoring menstrual regularity, decreasing androgen excesses, and decreasing IR (2). It has been suggested by some investigators that IR is present in all PCOS patients (3). However, others have reported that IR is not a universal finding, but rather is present in no more than 40-70% of PCOS patients (4). A ratio of fasting glucose (G) to fasting insulin (I) has been qualified as a simple and useful predictor of insulin resistance in women with PCOS (5). Other, more invasive tests such as insulin-glucose clamp studies, intravenous glucose tolerance tests, and qualitative model indices, were also described to diagnose insulin resistance (4). It has been shown in many worldwide studies, that the use of insulin sensitizing agents such as metformin can improve both reproductive and metabolic parameters in IR-PCOS patients. Metformin may help to improve menstrual irregularity, and restore spontaneous ovulation. It may improve the response to CC and other ovulation induction drugs and decrease the rate of hyperstimulation and early pregnancy loss. In addition, metformin is being evaluated for its potential long-term disease-modifying effect, such as prevention of impaired glucose tolerance, gestational diabetes, overt diabetes, dyslipidemia, hypertension and increased risk of cardiovascular disease (6,7). The objectives of this work are firstly, to characterize PCOS patients with and without IR, and secondly, to evaluate the possible beneficial role of insulin sensitizing agent (metformin) in the management of PCOS patients with IR regarding both reproductive and metabolic functions. MATERIAL AND METHODS This work was carried out at the departments of obstetrics and gynecology, internal medicine and clinical pathology, faculty of Medicine, Zagazig University Hospitals, after receiving the approvals from the departments involved in this study and after getting the consents from the patients. A total of 55 infertile women with PCOS were included in this study. The diagnosis of PCOS was made on the basis of at least two of the following three criteria:
Male factor was excluded by performing semen analysis. Tubal and peritoneal factors were also excluded by hysterosalpingography/laparoscopy. Other presentations along with infertility in those 55 patients included obesity (58%), hirsutism (54.5%) and AN (14.5%). All patients were classified according to the presence or absence of insulin resistance using (G/I ratio <4.5 mg/104 U) into two groups: Group I (IR-PCOS): included 34 infertile PCOS. The mean age was 29± 4 years. Patients in group I were further randomly subdivided into two groups according to the treatment protocol into: Group Ia (n=20): who were given insulin sensitizing (metformin) 1500 mg daily by mouth in addition to 50 mg CC daily by mouth for only five days starting from day 2 of the period or progesterone induced menses. Group Ib (n-14): who were given CC alone in the same regimen as group Ia. Group II (non IR-PCOS): included 21 infertile PCOS patients. The mean age was 27±5 years. All of them were given CC in the same regimen as group Ia. Table 1. Clinical characteristics of 55 patients with PCOS.
*S: significant Table 2. Biochemical profile in IR (group I) and non-IR patients (group II) with PCOS.
The treatment continued for six months or until pregnancy occurred. Patients who failed to ovulate or conceive received an incremental dose of 50 mg up to 150 mg for five days. The clinical and biochemical parameters were assessed initially and at end of treatment. All patients were subjected to:
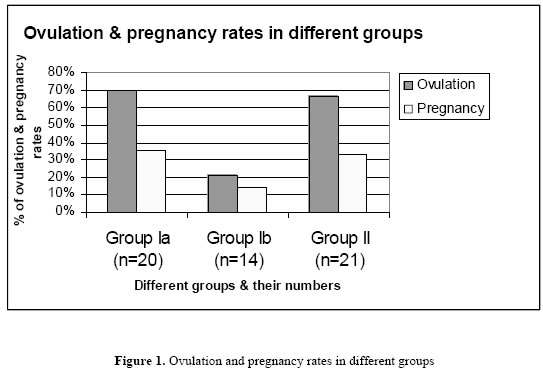
Ovulation was determined by midluteal serum progesterone of > 10 (ng/mL). The clinical and biochemical parameters were assessed initially and at end of treatment. Statistical analysis Data were presented as percentages, means and standard deviations. Data were analyzed with Med Calc software. Student t test was used for comparison of means. The (chi)2 was used for comparison of proportion. Significance was determined at <0.05 RESULTS On the basis of G/I ratio < 4.5 mg/104 U, 34 women (62%) had IR (group I) and 21 (38%) had no IR (group II). The clinical characteristics of the patients in the two groups were similar regarding age, gravidity, and parity. Mean BMI, obesity, hirsutism and AN were significantly higher in group I than group II (P < 0.05) (Table 1). Mean levels of LH, LH/FSH, and T, were significantly lower in group I compared with group II (P<0.05) while fasting (I) was significantly higher in group I compared with group II (P<0.05) (Table 2). After six months of treatment, ovulation rates in group Ia and II were significantly higher than group Ib (P >0.05). Pregnancy rates were also higher in groups Ia and II compared with group Ib but not to a significant level (Figure 1). Table 3 shows pre- and post-treatment parameters in group Ia who were on metformin + CC. There was significant improvement in ovulation, LH, LH/FSH, T and pregnancy rates (P<0.05). There also was significant improvement in mean levels of fasting (I), BMI, TG and TC (P< 0.05). Table 3. Comparison between pre- and post-treatment with metformin + CC for six months in IR-PCOS (Group Ia)
Table 4 shows pre- and post-treatment parameters in group Ib who used CC alone. No significant improvement was noticed in either reproductive or metabolic parameters (P>0.05). Table 5 shows the post-treatment parameters in group Ia and Ib regarding both reproductive and metabolic functions. There was a significant improvement in reproductive parameters (ovulation, LH, LH/FSH, T) and metabolic parameters (I, BMI, TG, TC) (P >0.05) in group Ia compared with group Ib but no significant difference in the pregnancy rates or hirsutism. Table 4. Comparison between pre- and post-treatment results with CC for six months in IR-PCOS (Group Ib)
DISCUSSION PCOS is a common cause of female infertility (8). Recently, IR has been recognized as a significant finding in this syndrome (9). The incidence of IR in patients with PCOS was found to be variable in different studies. Dunaif et al (11) demonstrated reduced insulin action in 38% of PCOS patients while Legro et al (5) demonstrated IR in 53% of non-Hispanic obese PCOS women. Table 5. Comparison between post-treatment results in IR-PCOS patients after the use of metformin +CC (group Ia) and CC alone (group Ib) for six months.
IR was also found to exist in 41% of PCOS patients as shown by Mor and co-worker (10). In this series of patients we noticed IR in 34 out of 55 patients with PCOS (62%) in Egyptian women. Designating PCOS patients as either IR or non-IR can allow comparison of common parameters between the two groups. Although IR may be found in both obese and lean PCOS patients (11,12) obesity is a well described risk factor for IR (13,14) In this present study mean BMI in IR group was significantly higher than in non IR patients and also the incidence of obesity in IR patients (70.5%) was significantly higher than non-IR ones (38%). The association between obesity and IR is not an incidental one, as excess insulin may increase central obesity, which in turn, worsens IR (15). AN is a specific clinical manifestation of IR. This can be seen in the groin, neck and axilla. AN is due to the effect of insulin on the basal cells of epidermis. The significant association between AN and IR was previously reported (10,16). In this current study AN was significantly higher in the IR group compared with non IR one. The biochemical findings in this series of patients showed a lower circulating total testosterone levels in IR than non-IR. The high insulin levels in IR patients may lower sex hormone binding globulin (SHBG) levels which result in high free testosterone. This free testosterone can explain the greater prevalence of hirsutism in IR group (17). Hirsutism is one of the clinical manifestation of hyperandrogenism. The significant association between hirsutism and IR was observed in this series of patients as well as other studies (17,18). In the current study the levels of LH and LH/FSH ratios were also significantly lower in IR group compared with non-IR one. This low LH levels can also explain lower circulating testosterone levels in the IR group. This finding of low LH levels in association with high insulin levels agrees with prior reports suggesting two possible different subtypes of PCOS patients, a low-LH and high -insulin type and a high-LH and low-insulin type. This observation again supports the need to subclassify PCOS patients into IR and non-IR groups (19). IR and compensatory hyperinsulinaemia can inhibit follicular development and ovulation as a result of hyperandrogenic intraovarian microenvironment and by altering gonadotropin secretion. This state of chronic anovulation explains clearly the low pregnancy rates in PCOS patients (20,21). In this series of patients there was a significant difference in the response to CC and subsequently the ovulation between PCOS patients with no IR compared with PCOS patients with IR when given the same regimen of CC treatment. This means that PCOS patients with IR are more resistant to ovulation induction with CC compared with non-IR patients. This observation was previously noticed in other studies. Mor et al reported that women with IR were more than 5 times as likely to be resistant to CC than women lacking IR (10). These findings suggest that IR should be designated as a unique group in PCOS that may perhaps get a benefit from using insulin sensitizing agent such as metformin to ameliorate the state of hyperandrogenism and chronic anovulation. This beneficial effect was reported by many international studies (22). In this current study, the addition of metformin to CC in IR-PCOS was found to improve significantly the rate of ovulation compared with the same group of patients who were on CC only after 6 months of treatment. Metformin was also found to significantly reduce BMI. Reduction in body weight is a well known effective therapy as both hyperinsulinemia and hyperandrogenism can be improved with weight loss and this will result in improvement of menstrual function. The role of metformin in improving the frequency of ovulation either alone or in combination with CC in PCOS women with IR was previously observed by other authors (22-25). Liu et al (26) reported that metformin in combination with CC improved significantly the ovulation rate and the state of hyperandrogenism in PCOS women with IR compared with controls (CC or metformin alone). The authors concluded that metformin appears to be an efficacious mode of therapy in PCOS patients with IR. Hahn et al (27) also reported that the use of metformin alone can improve significantly hyperandrogenism and insulin resistance in PCOS. Even in PCOS patients with normal insulin sensitivity, Baillargeon et al (28) on their study on 100 PCOS patients suggested that insulin-sensitizing drugs increase ovulatory frequency and ameliorate hyperandrogenemia, even in non-obese women with PCOS who appear to have normal insulin sensitivity. The pregnancy rate in the present study was higher in the group of PCOS patients without IR who were on CC and PCOS patients with IR who were on metformin + CC compared with IR-PCOS patients who had only CC. However, the PR was not significantly different between various groups. Although most studies agree that the combination of metformin to CC increases the pregnancy rate, there is no such agreement about how significant is this increase in the pregnancy rate. Some studies reported significant improvement (25,26,29), while others did not (23,30,31). This discrepancy in the pregnancy rates between different studied could be most probably due to the variation in the study design, the population or the duration of the treatment. When metformin as an insulin sensitizing drug was combined to CC in this current study, there was a significant improvement in both reproductive parameters such as ovulation rates and LH, LH/FSH, T mean levels as well as in metabolic parameters related to IR such as mean levels of I, BMI, TG, TC. This is in contrast to CC which when used alone, failed to improve significantly reproductive parameters and had no effect on the metabolic ones. This means that IR is a key feature in the pathogenesis of some group of PCOS patients. In agreement with our findings, is a recent randomized controlled study that used metformin in combination to CC for treatment of PCOS patients with IR. The authors came to the same conclusion of ours. They reported that identifying those patients of PCOS with IR and treating them with insulin sensitizing drugs is not only an effective way to treat their hyperandrogenic anovulatory problem but also a good option for early diagnosis and management of metabolic disorders related to IR (26). Cheang and Nestler also reported that ameliorating the metabolic syndrome associated with insulin resistance in PCOS with metformin may also prevent long-term cardiovascular and diabetes complications. Based on these data, metformin should be a first-line therapy for women with PCOS (23). Although the use of metformin alone or in combination with CC seems promising in the management of IR-PCOS, most of the previously mentioned studies including ours were conducted on a relatively small number of patients. In addition, the study design and the population differ between various studies. Undoubtedly, the need to a big multicenteric randomized controlled studies is essential to evaluate these new potential benefits of metformin. The clinicians also must counsel women appropriately before the initiation of metformin therapy (7). In conclusion; it appears that routine measurement of IR in PCOS patients to differentiate them as either IR or non-IR could be of help in the fields of academic research and clinical practice. Patients with IR are more likely to be obese, hirsute and have AN. They tend to be more resistant to CC for induction of ovulation. They also have lower LH, LH/FSH ratios, and testosterone levels. It seems that reversal of insulin resistance in PCOS with insulin sensitizing drugs constitutes the fundamental goal in the management of hyperandrogenic anovulatory infertility and also in the prevention of long-term consequences and should be integrated in the spectrum of therapeutic options. So, metformin appears to be a drug with multiple therapeutic effects far beyond its effect on lowering blood glucose in diabetes mellitus. REFERENCES
© Copyright 2005 - Middle East Fertility Society The following images related to this document are available:Photo images[mf05026f1.jpg] |
| |||||||||

{kind=link}