 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Middle East Fertility Society Journal, Vol. 10, No. 3, 2005, pp. 231-237 Outpatient minihysteroscopy and conventional hysteroscopy: a comparative study Gamal A. Kassem, M.D., Wael H. El-Brombly, M.D., Ahmed M. El Huseiny, M.D. Hysteroscopy
Unit, Department of Obstetrics and Gynecology, Zagazig University, Egypt Received January 11, 2005; Code Number: mf05040 ABSTRACT Objective: to compare the success of 3.5-mm
minihysteroscopy to conventional 5-mm hysteroscopy as outpatient procedure. Key words: minihysteroscopy, conventional hysteroscopy, pain, acceptability. Diagnostic hysteroscopy is now accepted as the gold standard investigation for diseases involving the uterine cavity (1). Other methods utilized in this clinical situation such as dilatation and curettage, transvaginal ultrasound or sonohysterography represent either blind, indirect measures or need general anesthesia to be performed. In contrast hysteroscopy allows direct visualization of the uterine cavity, and this explains its superior diagnostic accuracy (2-4). Diagnostic hysteroscopy has been performed about two decades ago with the conventional endoscope. Its diameter is 4-mm with an external sheath of 5- or 5.5-mm in diameter. Light general or local anesthesia was required in some cases.
Table 1. Indications for hysteroscopy in both groups.
IUCD = Intrauterine contraceptive device, US= Ultrasound Mini = minihysteroscopy However, it is clear that pain remains a significant problem for those having outpatient hysteroscopy with conventional one (5). Many trials have been done to reduce such pain during outpatient hysteroscopy like application of intracervical anesthetic gel, intracervical anesthesia, paracervical anesthesia and premedication with analgesic drugs (6-8). Recently, transcutaneous electrical nerve stimulation device was also tried (9). The success of these methods in alleviation of pain and anxiety during the procedure is limited. Paracervical block is even more painful than hysteroscopy itself (6-8). Minihysteroscopy using 2.7-mm telescope with 3.5-mm external sheath was introduced few years ago with encouraging results of decreasing pain and increasing acceptability (10). The aim of the present study was to compare the success of 3.5-mm mini-hysteroscopy to 5-mm conventional one as outpatient procedure. MATERIALS AND METHODS This prospective randomized study was conducted at the Hysteroscopy Unit, Department of Obstetrics and Gynecology, ZagazigUniversityHospitals from March 2003 to December 2004. The study included 740 patients referred to the unit for hysteroscopy. Patients were randomized to 5-mm rigid hysteroscope, Hamou II; model 26157 B, Karl Storz, Germany (group I) or 3.5-mm minihysteroscope, model 700-060, Tekno, Germany (group II). Illumination was provided by xenon light source XL-A 300 which has 300-Watt power. All the procedures were monitored using video camera, Storz, Telecam Pal 20210020, USA and 20-inch monitor, Sony model PVM 2043MO, USA connected to videocassette recording, Samsung model SV- A40G. Distention was conducted by glycine 1.5%. Change of the focus of the camera was done when shifting from one type of hysteroscope to another. After taking the history and clinical examination, hysteroscopies was done in a standard manner. The procedure was explained shortly to the patient whenever needed. After bimanual examination to detect the size and direction of the uterus, the hysteroscope was introduced gently into the cervical canal under direct vision. Verbal communication with patients during the procedure was done. The monitor was placed to be seen by the patient to be familiar with the hysteroscopic findings. Hysteroscopic examination was considered successful when the uterine cavity was entered and it was considered normal when the whole uterine cavity was seen free including both tubal ostia. When cervical dilatation was needed, it was done under local anesthesia by intracervical injection of 2- 3 ml of lignocaine 2%. If dilatation was difficult or painful the procedure was stopped and planned to be done under general anesthesia. Patients who experienced pain or anxiety and asking for sedation were received diazepam 10 mg very slowly intravenously. Pain was assessed according to Clark et al., in 1996 (6), using 4-digit score: almost no pain or discomfort, discomfort, painful but tolerable and intolerable pain. The procedure was stopped immediately if intolerable pain was occurred. After the examination patients were asked to remain in the lithotomy position for few minutes where they were observed for vasovagal reaction. During writing the report, patients were asked to sit on a chair in front of the physician for further observation. After that, patients were kept under observation in a waiting room for 30 minutes at least and they were asked to notify any complaints. Table 2. Hysteroscopic findings in both groups
* and †17 and 10 patients were excluded from group 1 and group 2 respectively (failure). Patients experienced vasovagal attacks were managed immediately. After stabilization of the general condition, they were admitted to the Day Surgery Unit (DSU) where they observed for at least 2 hours before discharge. Patients who received diazepam were also admitted to DSU for at least two hours. Duration of the procedure was calculated from start of entry of the hysteroscope into the cervical canal till its removal. Time of injection of local anesthesia or dilatation of the cervix was excluded. Table 3. Outcome in both groups
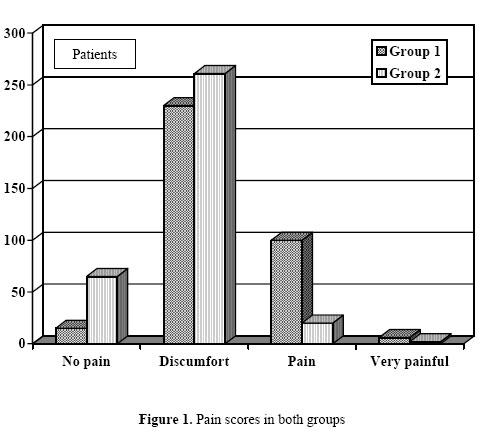
* 370 patients Statistical methods Equal randomization of the patients was done by a computer program. Data were expressed as mean ±SD. χ2 was used to compare figures of the two groups. p values < 0.05 were considered significant. RESULTS No statistically significant differences were found between the two groups regarding age and parity. Mean age was 31.2±6.1 and 30.8±7.9 years for group I and group II respectively, (x2 = 0.77, p > 0.05). Mean parity was 2.9±1.3 and 2.8±1.4 for group I and II respectively (x2 = 1.07, p > 0.05). As shown in Table 1, indications for hysteroscopy were comparable in both groups. Infertility was the most common indication followed by abnormal uterine bleeding. As shown in Table 2, no statistically significant differences were found between the two groups regarding normal and abnormal findings. Normal findings were found in 70% and 66.4% of group I and group II respectively, (x2 = 1.05, p = 0.3). Endometrial polyps were the most common abnormal hysteroscopic findings in both groups followed by intrauterine adhesions. As shown in Table 3, cervical dilatation under local anesthesia was required in 27 (7.3%) and 5 (1.4%) patients of group I and II respectively (x2 = 15.81, p < 0.001). Diazepam was required in 10 (2.7%) and 1 (0.3%) patients of group I and II respectively (x2 = 7.47, p = 0.006). Vasovgal attack was observed in 5 (1.4%) and 1 (0.3%) patients of group I and II respectively (x2 = 1.52, p = 0.2). All cases of vasovagal attacks occurred while the patients still lying on the examination table, 3 cases occurred during- and the other 3 occurred shortly after finishing the hysteroscopic procedure. Failure of the procedure occurred in 17 (4.6%) and 10 (2.7%) patients in group I and II respectively (p = 0.16). Causes of failure are shown in Table 4. According to the 4-digit score of pain, 18 (4.9%) patients in group I experienced the procedure with almost no pain versus 82 (22.2%) patients in group II (x2 = 47.36, p < 0.001). Two hundred thirty eight (64.3%) patients experienced it as discomfort versus 261 (70.5%) patients in group II (x2 = 3.26, p = 0.07). One hundred eight (29.2%) patients reported it as painful in the group I versus 25 (6.8%) in the group II (x2 = 63.15, p = < 0.001). Six (1.6%) in the group I experienced it as very painful versus 2 (0.5%) patients in group II (x2 = 1.15, p = 0.28);Figure 1. As shown in Figure 2, mean time of the hysteroscopy was significantly shorter in group II than that of group I (84±5 versus 155±9 seconds, p < 0.001). Table 4. Causes of failure
DISCUSSION Many advantages can be gained if diagnostic hysteroscopy can be conducted as outpatient procedure including absence of anesthesia and inpatient admission. In most cases, a clear diagnosis can be obtained in few minutes and the patient can go home or work. The main limitation of its wide spread use is pain and low patient tolerance (11). A recent study conducted in United Kingdom reported that patients with appointments to outpatient hysteroscopy experienced much anxiety before the procedure. The investigators believed that this anxiety would increase the like-hood of intolerance to the procedure (12). The present study shows that minihysteroscopy is less painful than conventional one. It was observed that 22.2% of patients have experienced minihysteroscopy almost always without pain or discomfort. This figure is significantly higher than that in the conventional hysteroscopy (4.9%). Moreover, it was observed that only 6.8 % of patients experienced minihysteroscopy as painful procedure, which is significantly less than that in the conventional one (29.2%). It was observed also that diazepam was required for alleviation of pain and anxiety during conventional hysteroscopy in 2.7 % of patients which was ten times more than that required for minihysteroscopy. Pain and anxiety represent an important issue in outpatient hysteroscopy. Clark et al (6) noticed that without use of local anesthesia, 39% of their patients described conventional hysteroscopy as painful procedure. Giorda et al in a comparative study between three groups of patients reported that intolerable pain was found in 17% of the first group where conventional hysteroscope was used. In the second group, only 6% experienced the procedure as painful when paracervical anesthesia was used with conventional hysteroscope. Complete absence of pain was observed when the minihysteroscope was used in the third group (13). It seems that reduction of the diameter of the hysteroscope is the most effective way to reduce pain of procedure. Smaller diameter instruments can traverse the cervix more easily increasing the compliance of the patient and makes completion of the procedure is acceptable (13). Since the introduction of the conventional hysteroscopes early in the 1980s, it was believed that its 4-mm diameter telescope is the least diameter, which can produce the sharpest and the deepest view (14). Thanks to developments in telecameras with zoom abilities and the use of large-sized monitors, it was possible to gain comparable view using the narrower-diameter instruments (15). In the present study cervical dilatation under local anesthesia was required in 1.4 % of patients when minihysteroscope was used. This was significantly less than that required for conventional one (7.3 %). The use local anesthesia with conventional hysteroscopy is common. Some used it as a routine (1). Others used it to achieve cervical dilatation or alleviation of pain during the procedure or both (16). Besides its variable success, many complications were reported with its use like bleeding from injection sites and intravasation. Some patients reported that local anesthesia is more painful than hysteroscopy itself (6-8, 15, 17). Therefore minihysteroscopy can reduce the need for local anesthesia avoiding its complications. The present study showed that the mean time required for the procedure was significantly shorter in the minihysteroscopy group. It could be expected that passage through the cervix as well as side-to-side movements inside the uterine cavity can be conducted in shorter time with instruments smaller in diameter. Similar results were reported (18, 19). Minihysteroscopy demonstrates its safety as an outpatient procedure, in the present study vasovagal attacks occurred very rarely (0.3%) in the minihysteroscopy group and it was less than that in the conventional one (1.4%). It is quite expected that shorter and less painful procedure will eventually yields less vasovagal reaction (18). Minihysteroscopy is not immune against failure. In the present study, failure rate of minihysteroscopy less than that the conventional one (2.7%.versus 4.6 %). This low failure rate confirms the superiority of the minihysteroscopy as outpatient procedure (18,19,20). Pain, cervical stenosis and poor view are the most common causes of failure mentioned in the literature as well as in the present study (10,16). On the other hand, one possible disadvantage of the minihysteroscopes is the higher cost. These endoscopes are more delicate and wear off in shorter time than larger instruments (19). They may also require more expensive accessory instruments like high-resolution monitors and xenon light sources. Further studies to evaluate these issues are suggested. In conclusion: Outpatient 3.5-mm minihysteroscopy is more successful than 5-mm conventional one. It is less painful and can be conducted in shorter time. It is safe procedure with low failure rate. REFERENCES
© Copyright 2005 - Middle East Fertility Society The following images related to this document are available:Photo images[mf05040f1.jpg] [mf05040f2.jpg] |
| |||||||||

{kind=link}
{kind=link}