 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Middle East Fertility Society Journal, Vol. 10, No. 3, 2005, pp. 238-243 A prospective comparative study of 3-D ultrasonography and hysteroscopy in detecting uterine lesions in premenopausal bleeding Fouad Abo Haemila, M.D., Dalia Youssef, M.D., Mohamed Hassan, M.D., Ahmed Soliman, M.D., Maha Mossad, M.D. Department
of Obstetrics and Gynecology, Faculty of Medicine, Cairo University, Cairo, Egypt Received on March 22, 2005; Code Number: mf05041 ABSTRACT Objective: to compare the accuracy of 3D ultrasound
in identifying endometrial and intramyometrial lesions in comparison to
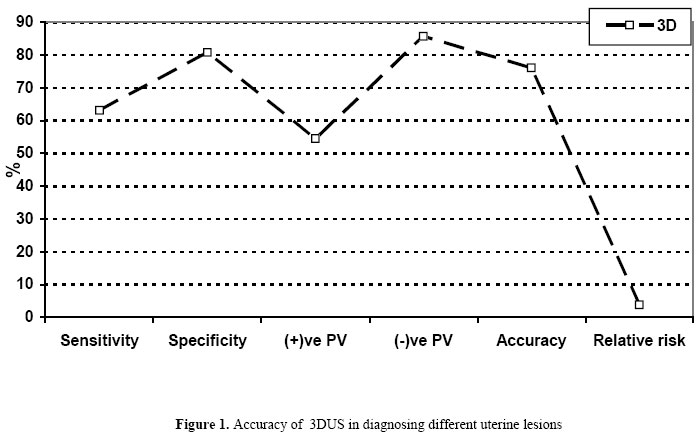
hysteroscopy. Key words: Three-D ultrasound, hysteroscopy, uterine lesions, premenopausal bleeding. Abnormal uterine bleeding is probably the most common symptom in gynecologic practice especially in premenopausal and postmenopausal women (1). Transabdominal ultrasound and later transvaginal two dimensional ultrasonography has been used extensively in cases of abnormal uterine bleeding to evaluate uterine pathology to exclude myomata, polyps and focal lesions and to check the adnexae (2). Three dimensional ultrasound offers new viewing window by allowing for arbitrary plane evaluation through a volume data set acquired from the pelvis (2). In addition, by 3D ultrasound more precise anatomical sections for exploring the endometrial cavity; the relations of myomata and their possible encroachment on the cavity, the diagnosis of endometrial polypi and the measurement of endometrial volume rather than thickness in cases of abnormal uterine bleeding (3). Hysteroscopy was one of the very earliest approaches to the direct study of the uterine cavity. The direct or magnified observation of the uterine cavity by hysteroscopy may offer a more precise diagnosis, a better ground for therapy or verification of results as compared to other methods such as hysterography. Although still hysteroscopy could be considered an invasive diagnostic procedure yet in all studies it is considered as the gold standard for evaluation of the uterine cavity (4). The aim of the present study is to evaluate the accuracy of three dimensional ultrasonography in diagnosis of uterine abnormalities compared to a gold standard (hysteroscopy). Table 1. Site of focal lesion localization as detected by 3D ultrasound & Hysteroscopy.
MATERIALS AND METHODS In the present study, 70 patients were included from those attending the Obstetric & Gynecology outpatient clinic at Kasr AL Aini hospital, CairoUniversity. For all patients full history taking with special attention to the premenopausal condition as regards onset, course, duration, possible etiology and complications. Also complete general and local examination to detect the size of the uterus, its mobility and the presence of any cervical or adnexal masses. Three dimensional vaginal ultrasonography was done to all patients with Voluson 530D MT 3D system, 3D ultrasound was done with a S-VDW 5-8 probe. Once the B - mode had been completed three dimensional volumes were recorded .the volumes were generated by the automatic rotation of the mechanical transducer 360 degrees. The probe was kept steady, the patient was asked to hold breath and volume mode was switched on. With the use of the medium line density, the typical acquisition time was between 4 and 10 seconds, the acquired volume was in the shape of a truncated cone the typical depth of the truncated cone was 4.3-8.6 cm and the angle aloha was 90 degrees. Relation of any focal lesion as myomas and polyps to the endometrium in the three planes with their dimensions. Volume calculation of the endometrium in the three planes to detect the endometrial volume. (Myomas were detected as hypoechoic areas in the myometrium while polyps as echogenic thickening of the endometrium). Hysteroscopy was followed within 48 hours. We used a rigid continuous flow panoramic hysteroscopy 25 cm in length, 4 mm in diameter, with an outer sheath of 5.5 mm & a 30 degree fibro optic lens (Karl Storz, Germany). The light source used in this study was a metal halide automatic light source from Circon Acmi G71A /Germany with a 150 Watt lamp. A fibro optic cable is connected to the light source and to the hysteroscope. Once the cavity was entered, a panoramic view of the uterine cavity to exclude uterine malformations or a deformed cavity. Once the telescope was introduced in the cavity, examination was done systematically, first the fundus, anterior, posterior & lateral walls of the uterus ending by visualization of the uterotubal junctions. If there is any intrauterine pathology detected, the shape, the size and the site of it was estimated. Because of the optical distortion, mental correction was essential to assess the actual size properly. The thickness the color, vasculature and consistency of the mucous membrane covering the uterine cavity was observed and recorded. If endometrial hyperplasia was suspected, a groove was always done with the optic by passing it through the posterior uterine wall and the thickness was estimated. Intrauterine adhesions can be mimicked by flaps or tissue and mucous bands. These were tested by touching them with an instrument; a true adhesion was readily disrupted and offers resistance. At the end of the procedure, the hysteroscope was slowly withdrawn through the cervical canal which was visualized to detect any intra cervical pathology and to observe the shuttering mechanism of the internal os. Statistical methods Data was statistically represented in terms of range mean standard deviation (±SD) & percentages. Comparisons was done using Student t test comparing parametric data. For comparing non parametric data, Chi Square (x2) test was performed. A probability value (P value) less than 0.05 was considered significant. Accuracy was represented using the terms of sensitivity, specificity, positive predictive value, negative predictive value and overall accuracy. All statistical calculations were done using computer programs Microsoft Excel version 7 (Microsoft Corporation, NY, USA) and Arcus quickstat version I. RESULTS The present study included 70 patients complaining of abnormal premenopausal uterine bleeding with age of 45.7 ± 4.1. The most common bleeding pattern was menorrhagia (40%) followed by menometrorrhagia (22.8%) then metrorrhagia (34.2%) then polymenorrhoea (2.8%). Three dimensional ultrasound detected 14 myomas (20%), 8 polyps (11.43%) and an endometrial mass, it was able to differentiate these myomas as 10 interstitial (14.29%) and 4 submucous (5.71%)in relation to the endometrial encroachment (Table 1). Hysteroscopy detected 6 myomas (8.57%) (all submucous), 11polyps (15.72%)and one endometrial mass (1.43%). Three dimensional US localization is comparable to hysteroscopy as shown by a sensitivity of 63.16, specificity of 80.77, positive predictive value of 54.55 and negative predictive value of 85.71, accuracy of 76.06 (Figure 1, 2, 3). DISCUSSION Hysteroscopy is an important method for the diagnosis of intrauterine pathology in several gynecologic complaints including abnormal uterine bleeding. Sensitivity and specificity of hysteroscopy are high in a large series of hysteroscopies performed in postmenopausal patients (98.2%)(5). However, diagnostic hysteroscopy is an invasive and costly procedure, which may be associated with risks such as uterine perforation and ascending genito-urinary infection (6,7). Furthermore, it provides only subjective assessment of fibroid size and indirect information regarding the depth of myometrial extension. Video recording of hysteroscopic findings may be used for quality control purposes, but the recorded data cannot be modified and the final diagnosis is determined by the initial findings at the operation (8). Transvaginal sonography has been studied as an alternative to hysteroscopy in investigation of abnormal uterine bleeding and was found to have a significantly lower sensitivity (54%) compared to hysteroscopy (79%) but a comparable specificity in premenopausal patients (9). Ultrasound enables accurate measurement of the size of the uterine fibroids. However, 2D ultrasound is not an accurate method of assessing the extent of submucous fibroid protrusion into the uterine cavity (10,11). Three-dimensional (3D) transvaginal ultrasound has been commercially available. This technique allows detailed evaluation of pelvic organs by collecting a series of sequential ultrasound images and converting them into an ultrasound volume. This information is digitally stored as a dataset, which may then be analyzed on line. The dataset is reconstructed in such a way as to allow visualization of an organ from any chosen angle and in any arbitrary plane (12). This study showed good overall agreement between diagnostic hysteroscopy and 3D transvaginal ultrasound in the diagnosis of uterine abnormalities. 3D US detected, 8 polyps (11.43%) and an endometrial mass. it was able to differentiate these myomas as 10 interstitial (14.29%) and 4 submucous (5.71%). Hysteroscopy detected 6 submucous myomas (8.57%), 11 polyps (15.71%) which by pathology had been differentiated to 9 adenomatous polyps and 2 fibroid polyps. Pasqualotto et al compared retrospectively similar parameters (submucous fibroid, polyps) on three hundred seventy five patients complaining of abnormal uterine bleeding, main pathology findings were endometrial polyps (172, 45.9%) submucous myomas (105,28%) (13). In the present study, by comparing the 3D US results against hysteroscopy we found that 3DUS has a sensitivity of 63.16 specificity of 80.77, positive predictive value of 54.55 and negative predictive value of 85.71, accuracy of 76.1 and relative risk of 3.82. Pasqualotto et al., while comparing similar parameters on three hundred seventy five patients complaining of abnormal uterine bleeding found that the Sensitivities of the preoperative diagnostic tools specifically for myomas and polyps were for trans vaginal sonography 74% and 39 %, for saline infusion sonography 96% and 96 % and for hysteroscopy 100%, 99% (13). In a subsequent study, while dealing with similar parameters to detect value of sonography in relation to hysteroscopy in diagnosing intracavitary uterine pathology, it was found that sensitivity, specificity positive and negative likelihood ratios were 67%, 87%, 5.15, 0.38 for Trans vaginal sonography and 92%, 95%, 18.4, 0.08 for hysteroscopy (14). The value of three dimensional ultrasound were further supported in many subsequent studies published in the medical literature later in the new millennium (15, 16). Recently, a "virtual endoscopy" technique based on 3D hysterosonographic data was described in a pilot study. Five patients who presented intrauterine abnormalities (polyps, n=2; leiomyomas, n=3) underwent 3D transvaginal hysterosonography. The 3D data set was subsequently processed by using a proper software that creates virtual endoscopy images. After ultrasonographic examination, patients had a conventional hysteroscopy. In all patients intrauterine lesions were easily and reliably detected by computer-reconstructed 3D hysterosonography. Images obtained by this "virtual hysteroscopy" technique, including fine intrauterine details, were remarkably comparable to those obtained by conventional hysteroscopy. Thus, computerized reconstruction of 3D hysterosonography may in the future support the use of 3D ultrasound in characterization of intrauterine lesions (17). CONCLUSION Three dimensional ultrasound can be used in diagnosing uterine focal lesions with results comparable to hysteroscopy. Further research is needed to show whether this increased diagnostic capability of 3D ultrasound could be the option of choice before surgery. REFERENCES
© Copyright 2005 - Middle East Fertility Society The following images related to this document are available:Photo images[mf05041f2a-b.jpg] [mf05041f3a-b.jpg] [mf05041f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}