 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Middle East Fertility Society Journal, Vol. 10, No. 3, 2005, pp. 244-249 Reduction of early postoperative pain after diagnostic laparoscopy with local bupivacaine: a randomized placebo controlled study Ashraf M. N. Refaie, M.D., M.R.C.O.G.*, Mowafy M. Khatab, M.D.† Departments of Obstetrics and Gynaecology,
and Anesthesia, ZagazigUniversityHospital, Zagazig, Egypt Received on February 20, 2005; Code Number: mf05042 ABSTRACT Objective: To evaluate the effects of preincisional
infiltration and intraperitoneal instillation of bupivacaine on early relief of
pain after diagnostic laparoscopy. Key words: Diagnostic laparoscopy, postoperative pain relief, local anesthetics Diagnostic laparoscopy has become a very common day case procedure. An essential advantage of the day case unit is the short period of hospital stay which is usually few hours. Before the patient goes home, an adequate pain relief should be achieved to make sure that the need to parentral analgesia is less likely (1,2). Laparoscopy is associated with some discomfort or pain, with most women requiring postoperative analgesia for abdominal and/or shoulder pain. The reported frequency of pain after diagnostic laparoscopy varies from 35% to 65% (3). Reducing this pain to a level at which narcotic analgesics are no longer required is an important step toward performing laparoscopy as day case procedure (4,5). This pain, is secondary to peritoneal stretching and diaphragmatic irritation. It contributes to patient morbidity by increasing analgesic requirement. The need for analgesia was identified as the most important factor in postponing resumption of normal daily activity (6). Several strategies are advocated to reduce postoperative pain after laparoscopy such as infiltration into cannula sites, intraperitoneal instillation or injection of local anesthetic into fallopian tubes during laparoscopic sterilization. Results of these studies on this subject are conflicting. In some studies these measures were shown to be effective in reducing the amount of pain but not such effective in others (7-12). We designed this randomized, placebo, controlled double-blind study to evaluate the effects of preincisional infiltration and intraperitoneal instillation of bupivacaine on early postoperative relief of pain after diagnostic laparoscopy. MATERIAL AND METHODS Subjects Sixty three infertile women (age range 19-38 yrs) undergoing diagnostic laparoscopy were included in this study. The study was approved by the hospital ethics review committee, and every patient provided informed consent. Indication for laparoscopy was unexplained infertility. Before surgery, each patient underwent a complete clinical history, physical examination and laboratory investigations to exclude metabolic and cardio-respiratory disorders, morbid obesity, history of pelvic operations, and allergy to protocol drugs or general anesthesia. Also excluded were those who had a condition that required operative laparoscopy, laparotomy, or more than two punctures for laparoscopy. Patients were prospectively randomized by a house officer to one of two groups using standard random numbers table. Women in treatment group (group I) included 32 patients aged 31.5±6.2 yrs with body mass index (BMI) 24.4±4.4 kg/m2. Group II (control group) included 31 patients aged 30.4±5.7 and BMI 25.2±3.6 kg/m2. Bupivacaine or saline was prepared by the anesthetist. Operative technique All patients received pre-induction with 0.01-0.02 mg/Kg atropine sulphate intramuscularly (I.M) and 2-4 mg midazolam intravenously (I.V). After pre-oxygenation, anesthesia was induced with 2mg/Kg propofol and 1-2 mg/Kg fentanyl. Tracheal intubation was facilitated by administration of 1-2 mg/Kg succinylcholine IV. The maintenance of anesthesia was achieved with 1-2% isoflurane and 50% nitrous oxide in oxygen. Rocuronium was used to ensure complete muscle relaxation throughout the surgery. In group I, the sites of trocar insertion (umbilical, suprapubic) were infiltrated with 5-7 ml of 0.25% bupivacaine before incision. Diagnostic laparoscopy was carried out in the usual manner with two reusable trocars. The main umbilical one was 10 mm in diameter and the ancillary one was 5 mm. Carbon dioxide was used for insufflation. Intraabdominal pressure was maintained below 13 mm Hg. In group I, at the end of procedure, 40 ml of 0.125% bupivacaine was instilled into the pelvic cavity and the under surface of diaphragm using an irrigator advanced through the ancillary port site under direct vision. Group II received equal volumes of saline instead of bupivacaine at the trocar sites and into the peritoneal cavity. At the end of procedure, the abdomen was deflated and trocar sites were sutured using vicryl stitches. The anesthetist also reverses muscle relaxation with 0.04-0.08 mg/Kg neostigmine sulphate and 0.01-0.02 mg/Kg atropine sulphate IV. The surgeon, anesthetist, and recovery personnel were blinded to the substance instilled as all these drugs are colorless and labeled "local anesthetic". Only the SHO knew what drug was given. Pain evaluation All patients were prescribed postoperative analgesia of pethidine 15 mg I.V. as necessary. Recovery personnel, who were blinded to intraperitoneal substance, gave analgesics again when requested by the patient. Modified McGill pain intensity scores (13) (0 = no pain, 5 = very severe pain at rest that requires analgesia) was administered for patients' self assessment of pain 1,2 and 3 hours postoperatively. Patients remained in the recovery room until they were alert, when their condition was assessed by recovery personnel and confirmed by a physician. They were discharged if they had stable vital signs, were ambulatory with minimal assistance, tolerated oral fluids, and had voided spontaneously. Time from extubation to discharge and time to first analgesic in minutes were measured. All patients stayed for at least 3 hours to complete the assessment of pain, however, those patients who felt that they can be discharged from the hospital 2 hours after surgery were recorded and then allowed to go home after completion of assessment. Table 1. Clinical characteristics and operative time in group I and group II
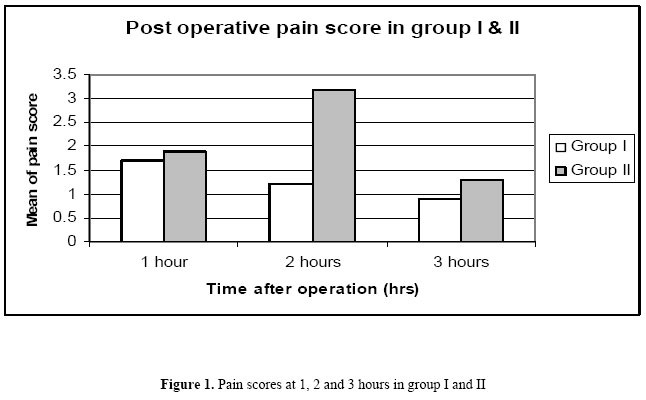
Statistics analysis Data were presented as percentages, means and standard deviations. Data were analyzed with Med Calc software. Student t test was used for comparison of means. The (chi)2 was used for comparison of proportion. Significance was determined at <0.05 RESULTS The clinical characteristics and operative time were similar in the patient and control groups regarding age, BMI, parity and operative time (Table 1). Pain scores at one, two and three hours were significantly lower in patient group compared with control group (P< 0.05). Pain scores were 1.7±0.2, 1.2±0.1 and 0.9±0.2 in group I at one, two and three hrs respectively Vs 1.9±0.2, 3.2±0.2 and 1.3±0.3 in group II (Figure 1). Table 2. Post operative outcome in patient and control group I and II
The number of patients who needed postoperative analgesia in group I was significantly lower than group II (7 out of 32 Vs 19 out of 31) (P<0.05). The time in minutes to first analgesic in patient group (42.5±4.6) was significantly higher compared with control group (32.2± 2.8) (P <0.05). The number of patients who were felt they can be discharged 2 hours after operation in group I was significantly higher compared with group II (22 out of 32 Vs 10 out of 31) (P<0.05) (Table 2). DISCUSSION Adequate postoperative relief of pain early after diagnostic laparoscopy is an essential goal to be able to perform this operation as a day case procedure and thus help the patient to go home early in a stable condition with no or minimal assistance. Postoperative pain associated with diagnostic laparoscopy is due to peritoneal stretching, diaphragmatic irritation, or, to a lesser extent, abdominal puncture. The receptors involved seem to be susceptible to blockade with a relatively low dose of local anesthetic (7). Results of studies on this subject show some controversy (14-18). Such differences in results could be due to many reasons, such as heterogeneity of patient populations, number of surgeons, inclusion of women undergoing diagnostic laparoscopy or other operative procedure such as tubal sterilization, and lack of study power (8). In this series of patients the intensity of pain in the bupivacaine group was significantly lower compared with control. The need for escape postoperative analgesics and time to discharge, also were reduced in the bupivacaine group. Our findings are in agreement with other reports (7,19,20). Parsanezhad et al in their comparative double-blind randomized placebo controlled study on 134 women undergoing diagnostic laparoscopy reported significant pain relief both early and 24 hours after operation when bupivacaine was instilled in the peritoneal cavity and lidocaine was infiltrated into the trocar site. The authors recommended irrigation of bupivacaine to both hemi-diaphragm and pelvis at the completion of the procedure (7). On the other hand, another randomized studies noticed that the effect of local administration of bupivacaine before incision and intraperitoneally was effective in reducing pain immediately after operative laparoscopy but not beyond 30 minutes, so they did not recommend its routine administration (1,8). The explanation of the conclusion drawn by this later study is most probably due to the fact that the patients had operative laparoscopy and pain could have originated from sites that were manipulated, cut, or coagulated. The timing of administration of local anesthetic is another point of controversy. Infiltration of anesthetic agent before incision is known as preemptive analgesia. Some studies showed that this type of analgesia is more effective in preventing afferent signals from reaching the spinal cord and thus more beneficial in reducing postoperative pain significantly compared with giving the local anesthetic at the completion of procedure (21,22). Another group also reported that visual analog pain scores and consumption of analgesics were significantly lower in patients receiving intraperitoneal bupivacaine immediately after creation of pneumoperitoneum than at the end of surgery (23). In our subjects, the possibility of a similar outcome with instillation of bupivacaine solution at the beginning of surgery was not assessed; because many of our patients had tubal patency test as a part of diagnostic procedure using dye which necessitated irrigation or suction of the dye from pelvis with of course removal of the local anesthetic if it was instilled earlier. In addition, intraperitoneal instillation of bupivacaine effectively reduced postoperative pain even if it was administered at the end of the procedure. In this present study, bupivacaine was found to be most helpful in reducing the pain in the early few hours after the operation. This is the period in which the pain is at its highest intensity and the patient needs adequate pain relief to be able to be discharged (24). This effect is expected as the drug's half-life is only 2.7 hours (range 1.2-4.6 hrs) (8). One study showed a beneficial effect of using bupivacaine instillation for a longer period of time. The authors claimed that pain score was significantly lower 24 hours after diagnostic laparoscopy compared with controls (7). Although we did not assess the pain score after the patients being discharged, we feel that it is unlikely that this relief of pain after 24 hours is due to the effect of bupivacaine alone. Intraperitoneal instillation and trocar site infiltration with local anesthetic was found to be beneficial in reducing postoperative pain in patients having diagnostic microlaparoscopy when performed under local anesthesia with conscious sedation. The authors noticed significant lower pain scores immediately after surgery and 1, 3, and 6 hours afterwards in the treatment group compared with the controls. The authors therefore recommended this regimen of analgesia with microlaparoscopy(25). Many studies also reported this beneficial effect of local anesthetics in reducing postoperative pain in other gynecological operative laparoscopy such as sterilization, ovarian cystectomies, diathermy coagulation of endometriosis and hysterectomy (3,8,26). The same protocol also is advocated to be useful by surgeon performing laparoscopic cholecystectomy (15,27). In conclusion; this protocol of using intraperitoneal instillation and trocar sites infiltration of local anesthetics was found to be useful in reducing early postoperative pain and the need to postoperative analgesia after diagnostic laparoscopy. It also helps to increase the rate of patients who can be discharged within few hours after the procedure and hence, get the maximum benefit from using the day case unit. REFERENCES
© Copyright 2005 - Middle East Fertility Society The following images related to this document are available:Photo images[mf05042f1.jpg] |
| |||||||||

{kind=link}