 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Middle East Fertility Society Journal, Vol. 10, No. 3, 2005, pp. 250-257 A prospective comparative study to assess the accuracy of MRI versus HSG in tubouterine causes of female infertility Khaled Abdel Malek, M.D.* ,Mohamed Hassan, M.D. * ,Ahmed Soliman, M.D. *, Heba El-sawah, M.D. *, Amr Osama Azab, M.D.† Departments of Obstetrics and Gynecology, and Radiodiagnosis, Cairo University,
Cairo, Egypt Received on March 14, 2005; Code Number: mf05043 Abstract Objective: To evaluate the role of magnetic resonance imaging versus
hysterosalpingography during investigating infertile women due to uterotubal
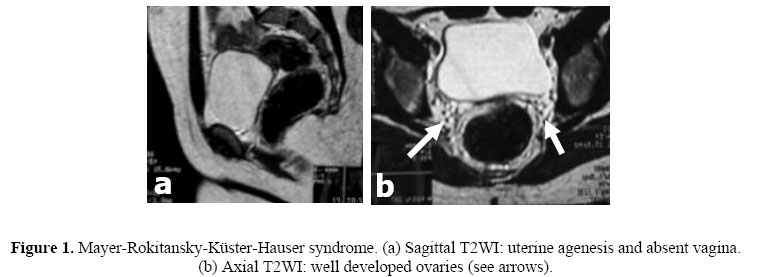
causes of infertility Key words: hysterosalpingography, magnetic resonance imaging, laparoscopy, infertility INTRODUCTION Infertility is defined as one year of unprotected intercourse that does not result in pregnancy (1). Uterine abnormalities were detected in 15-27% of infertile women (2). Hysterosalpingography (HSG) is the most widely used method of evaluating the uterus and fallopian tubes, however, it is invasive and inconvenient to women. Many patients request anesthesia to perform HSG. It might even introduce infection as Chlamydia (3). When uterine abnormality is suspected, laparoscopy is often required. On the other hand, Magnetic resonance imaging (MRI) produces images with exquisite anatomical details that are clearer than those obtained with ultrasonography or radiography, and -as far as we know- it is safe (4). MRI has the potential to replace HSG / laparoscopy in the diagnosis of abnormalities of the female genital tract, being non-invasive, with no hazard from ionizing radiation, improved soft tissue contrast resolution and its capability of multidirectional imaging, simultaneous imaging of multiple sections, along with its visualization (5,6). Disorders of the Fallopian Tubes MR imaging aids in noninvasive assessment of tubal dilatation and peritubal disease. Dilated fallopian tubes manifest as fluid-filled ducts, which appear as retort-, sausage-, C-, or S-shaped cystic masses at MR imaging. Thin, longitudinally oriented folds along the interior of the tube represent incompletely effaced mucosal or submucosal plicae (7). MR imaging can also be helpful in assessment of pelvic inflammatory disease by showing tubo-ovarian abscesses, dilated fluid-filled tubes, and free pelvic fluid (8). On T1-weighted images, a high-signal-intensity rim in the innermost portion of a tuboovarian abscess has been reported. This rim shows marked enhancement on post contrast images and is believed to correspond to granulation tissue admixed with hemorrhage (9). Moreover, dilated fallopian tubes with high signal intensity on T1-weighted images, which correspond to hematosalpinx, reportedly correlate with one of the effects of endometriosis (7). Nevertheless, MR imaging is as yet of little use in assessment of adhesions. Uterine Disorders 1. Müllerian Duct Anomalies Multiplanar MR imaging is useful for documenting uterine anomalies (10-13) Bicornuate uterus appears in MR imaging as follows:(a) divergent uterine horns with an intercornual distance exceeding 4 cm and (b) concavity of the fundal contour or an external fundal cleft more than 1 cm deep (14). While, Septate uterus is demonstrated as low signal intensity on T2-weighted images, whereas a septum composed of abundant muscular tissue shows intermediate signal intensity. The external uterine contour is normally convex, flat, or minimally indented by less than 1 cm (14), in contrast to that of a bicornuate uterus. 2. Leiomyoma The diagnostic MR imaging finding for leiomyoma is a sharply marginated mass that typically has lower signal intensity than the myometrium on T2-weighted images (15). In addition, MR imaging is a highly accurate modality for differentiating leiomyomas from adenomyosis in cases of enlarged uterus, with a reported accuracy of 99% (16). In the latter, the abnormality is ill defined causing swelling of the affected wall that shows punctuate foci of abnormal high T2 signal with thickening of the junctional zone (17). The objective of this study is to assess the accuracy of MRI compared to hysterosalpingography (HSG), which used to be a mainstay in the diagnosis of tubal and uterine causes of female infertility. MATERIAL AND METHODS The present study included 94 women who were admitted to the Department of Obstetric and Gynecology, Kasr El-Aini Hospital between June, 2002 and Dec., 2004. They were admitted complaining of inability to conceive for more than one year. Each patient was asked about the duration of infertility whether 1ry or 2ndry. A detailed menstrual history and obstetric history were taken with emphasis on previous pregnancies, history of any abortions and gynecological history with emphasis on abnormal vaginal bleeding and any D&C done. Detailed general, abdominal and pelvic examinations with provisional clinical examinations were performed. A husband's semen analysis was a pre-requisite before admission. All women underwent ultrasonography. When ultrasound showed or suspect abnormality, patient was recruited in the study. Laparoscopy was performed to confirm different findings, being considered the gold standard for diagnosis. All hysterographies were performed during the early follicular period of the menstrual cycle. The sterile instrument tray was inspected checking the presence of a radiolucent vaginal speculum & a cervical plug to prevent reflux. Fractionated technique under fluoroscopic guidance using iodinated water-soluble contrast medium (Telebrix). The initial x-ray was taken after the injection of 3-4 ml of contrast material. 2-3 serial films were taken. Another control film was taken 20 minutes later. Magnetic resonance imaging (MRI) was performed with 1 or 1.5-T superconducting magnet (Signa; GE Medical Systems, Milwaukee, Wis or Philips, Gyroscan machine respectively). Oral administration of water for bladder distention was not performed. Either the body coil (GE machine) or a synergy-body coil (Philips machine) was used. First, fast spin echo T2-weighted images (WI) were performed in the axial, oblique coronal and sagittal planes with a repetition time (TR) of 4,000-5,000 msec. and an echo time (TE) of 100-110 msec, three signals acquired, an echo-train length of eight, and a 156x160 matrix. The section thickness was 5-7 mm with a 1 mm intersection gap and a 28 cm field of view. Then, spin echo T1-WI 600/15 msec (TR/TE) were obtained in the axial plane with two acquisitions, 192x256 matrix, 5-7 mm section thickness, and 1 mm interscan gap extending from the lower abdominal aorta down to the end of the pelvis. Statistical analysis Statistical analysis was performed to evaluate the sensitivity, specificity and diagnostic accuracy of hysterosalpingography and MRI in correlation with Laparoscopic findings as the gold standard. RESULTS The study population comprised 96 patients complaining of infertility, with their age ranged from 21-45 year with a mean age of 28 years and 7 months. Seventy five patients complained of Primary infertility, 21 patients complained of secondary infertility and 8 patients complained of secondary infertility and repeated abortions. Sixteen women were found to have congenital anomalies of the genital tract, 23 patients suffered from fibroids, 5 patients suffered from intrauterine synechiae, 8 patients suffered from uni- or bilateral hydrosalpinx, and 26 had peritubal adhesions. Patients with congenital anomalies were as follow: One patient suffered from complete failure of development of the Müllerian system (Meyer- Rokitansky- Küster- Hauser syndrome) and complained of primary infertility for 1 year. Another patient had ovarian dysgenesis, hypoplastic uterus and breasts and hirsutism. She complained of primary amenorrhea and primary infertility for 2 years. The patient received replacement therapy after marriage. Four patients had bicornuate uterus: One of them had bicornuate uterus, left hydrosalpinx and left peritubal adhesions. One patient had bicornuate uterus and fused pelvic kidneys. Another one had a unicornuate uterus and tubal block. She complained of primary infertility. Five Patients had septate uterus: two of patients had septate uterus & peritubal adhesions in addition and complained of primary infertility. One patient had PTA & fundal myoma and complained of primary infertility. Four patients had subseptate uterus: They complained of secondary infertility and repeated abortions DISCUSSION In recent years, demand for infertility services and treatment of infertility have increased. Laparoscopy, hysteroscopy, and hysterosalpingography are the most effective techniques currently used to evaluate female pelvic disorders related to infertility. Magnetic resonance (MR) imaging has also been used for over 10 years to evaluate problems associated with female infertility. MR imaging is well known to provide accurate information for differentiation of congenital uterine anomalies and detection and localization of uterine leiomyomas. One of the main advantages of hystero-salpingography is that it provides documented films for the findings whether normal or abnormal. On the other hand, this technique has several inherent disadvantages including exposure to ionizing radiation, exposure to iodinated contrast material and limitation of the investigation to include only the inner contour of the upper genital tract (3). Although HSG is accepted as a first diagnostic modality in infertility, it is performed without any sedation or anesthesia and, therefore, the patient is not relaxed (18). Hence, the rate of tubal spasm at the cornua and, therefore, false positive tubal blockage, is said to be higher than usual. Laparoscopy is usually indicated when an abnormality is detected. On the contrary, the major advantage of MR imaging is the nonuse of ionizing radiation, which is an important consideration in women of reproductive age. Another advantage is that MR imaging is less invasive and less observer dependent than the classic imaging techniques. Furthermore, recent advances in MR imaging with the phased-array coil have created further imaging possibilities, resulting in excellent spatial and tissue contrast resolution, multiplanar capability, and fast techniques. This rendered MRI a safe non invasive imaging modality and its use as an alternative diagnostic tool is an attractive option. The disadvantages of MR imaging are limited to its relatively high cost and long examination time; it is contraindicated in patients with pacemakers, cochlear implants, and certain metallic objects. The aim of this study was to assess the sensitivity and specificity of MRI as a relatively non invasive modality in the detection and differentiation of tubal and uterine causes of female infertility used to be detected with hysterosalpingography. In the present study, out of 94 patients examined, 16 patients had congenital anomalies of the FGT and only one patient showed complete failure of the Müllerian duct development or the Meyer- Rokitansky- Küster- Hauser syndrome (Figure 1). Also, a single patient had unicornuate uterus. Unicornuate uteri are caused by the unilateral failure of Müllerian migration and account for approximately 10% of Müllerian developmental anomalies (19). In this study the unicornuate uterus was definitely diagnosed by HSG. MRI was only suggestive. Table 1. Accuracy of MRI vs. HSG regarding different findings
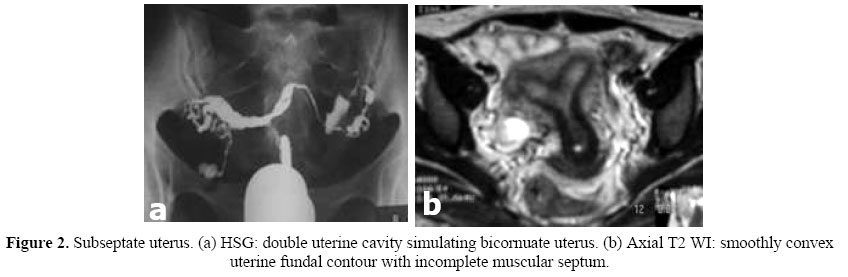
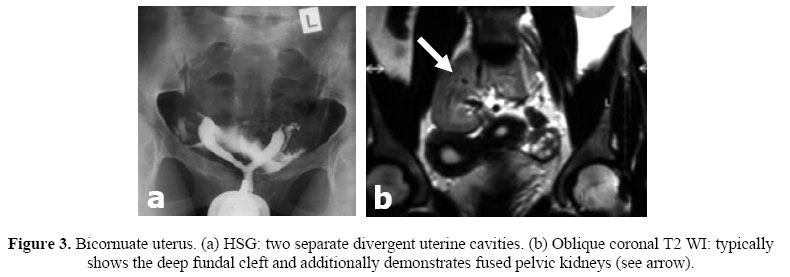
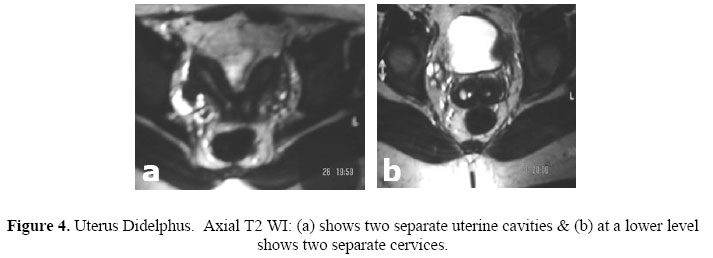
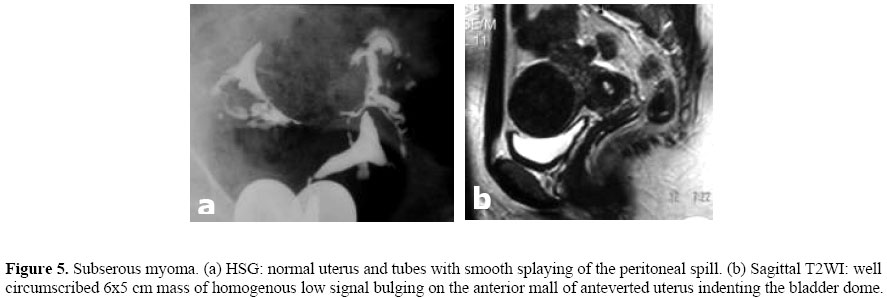
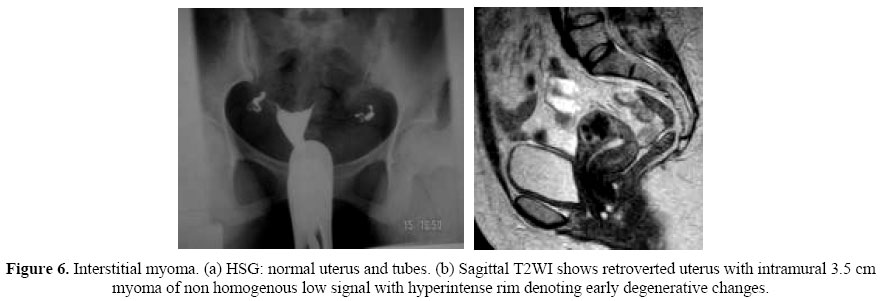
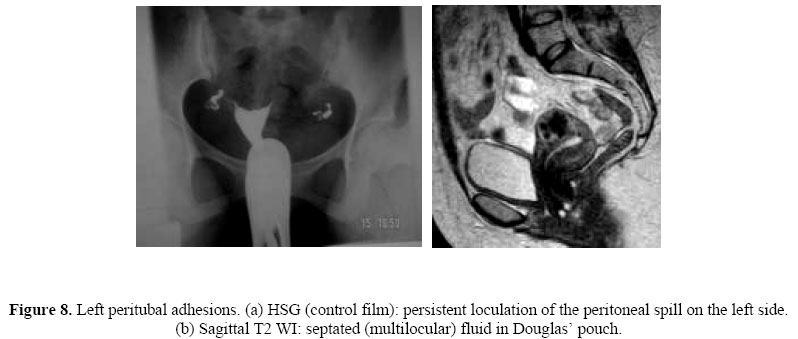
PPV = Positive Predictive value NPV = Negative Predictive value Bicornuate uterus was found in 4 patients in this study; the investigations were carried out using HSG and MRI and confirmed by laparoscopy. The incidence of septate uterus varies between 20% and 80% of Müllerian developmental anomalies, depending on the series (20-22). The large variation in the reported incidence is most likely related to the difficulty in distinguishing bicornuate and septate uteri before the advent of MR imaging. Although it is noted that the cornu of the septate uterus frequently create a more acute angle than seen with a bicornuate uterus, the degree of overlap on a HSG is uncertain (23). On MRI, the bicornuate & septate uterus appeared as a uterus with 2 cavities. However, they can be differentiated by the deep (> 1 cm) fundal cleft present in the bicornuate uterus on coronal oblique images of the uterus and widened intercornual distance > 4 cm. The septate uterus had a convex, flat or minimally indented (< 1 cm) outer fundal contour on coronal oblique images of the uterus (Figure 2). Homer et al ;(2000) reported that the most common major uterine anomaly in women with recurrent pregnancy loss is subseptate uterus (24). The results of Salim et al; are similar, showing that the subseptate uterus was the most common major uterine anomaly, accounting for 77% of cases suffering from repeated abortions (25). The present study included 5 patients with septate uterus. HSG and MRI were performed and the end result was confirmed by laparoscopy. In this study one patient with bicornuate uterus had fused pelvic kidneys (Figure 3, 4) and another patient with subseptate uterus had a left pelvic kidney. MRI failed to diagnose all the five patients with intrauterine synechiae that were detected on hysterosalpingography. Twenty three women suffered from fibroids, 5 patients had a fibroid ≥ 5cm and the remaining myomas ranged 1-3.5 cm. MRI missed two submucous myoma (1cm). According to Murase et al, magnetic resonance (MR) imaging is an accurate imaging technique for detection and localization of leiomyomas (26). On T2-weighted images, non-degenerated leiomyomas appear as well circumscribed masses of decreased signal intensity (Figure 5); however, cellular leiomyomas can have relatively higher signal intensity on T2-weighted images and demonstrated enhancement on contrast material-enhanced images. Degenerated leiomyomas have variable appearances on T2-weighted images according to the type and extent of degeneration (Figure 6). Regarding tubal pathology, MRI had an accuracy of 99.1%, sensitivity of 87.5%, specificity and PPV of 100% and NPV of 99% in diagnosing hydrosalpinx (Figure 7). This study included 13 patients with peritubal adhesions and HSG had an accuracy of 95.3%, while MRI failed to show these adhesions. In only one of these cases, MRI showed fine septation within fluid in Douglas pouch (Figure 8). CONCLUSION MR imaging is a useful noninvasive modality as an adjunct for routine infertility work-ups. In infertile women with suspected uterine anomalies, magnetic resonance imaging is the study of choice because of its high accuracy and detailed elaboration of uterovaginal anatomy. Moreover, MRI has the advantage of extending the diagnostic information to detect the frequently associated anomalies of the urinary tract. Laparoscopy and hysteroscopy are reserved for women in whom interventional therapy is likely to be undertaken REFERENCES
© Copyright 2005 - Middle East Fertility Society The following images related to this document are available:Photo images[mf05043f7.jpg] [mf05043f2.jpg] [mf05043f1.jpg] [mf05043f5.jpg] [mf05043f8.jpg] [mf05043f4.jpg] [mf05043f3.jpg] [mf05043f6.jpg] | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}