 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
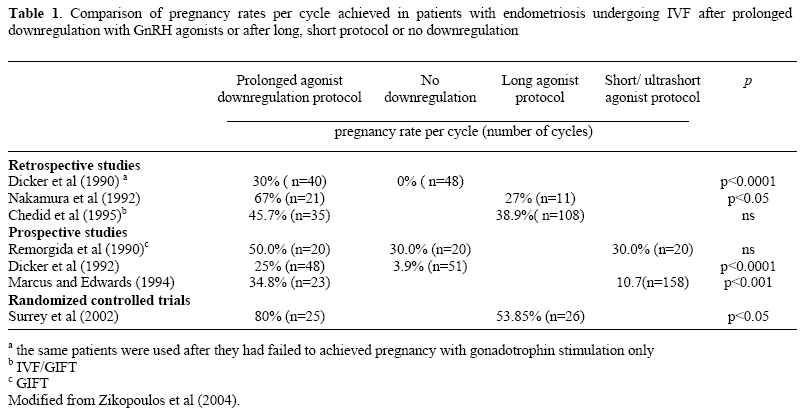
DEBATE Is it of value to treat endometriosis prior to IVF? Comment by: Efstratios M Kolibianakis, M.D.,Basil C Tarlatzis, M.D.,Thessaloniki, Greece Code Number: mf06003 INTRODUCTION Although endometriosis is a common finding in infertile women (1), the mechanism by which it is associated with infertility remains unclear. Not unexpectedly, the optimal treatment for women with endometriosis, who wish to become pregnant, is debatable. Women, who suffer from infertility and are diagnosed with endometriosis, may undergo surgical or medical treatment with the aim to enhance their reproductive potential or proceed immediately to IVF. In the first case, expectant management is advocated for a variable period of time. If conception does not occur, IVF is usually the proposed method of treatment, although ovarian stimulation with intrauterine insemination might be an option in certain cases with mild or minimal endometriosis. On the other hand, IVF may be immediately selected as the preferred mode of treatment, either due to other coexisting factors (e.g. severe male infertility, tubal infertility, female age etc) or because treatment of endometriosis is considered as not beneficial, and in cases where it involves destruction of ovarian tissue, as potentially harmful. It is not the purpose of the current review to discuss which the best treatment strategy is for infertile patients diagnosed with endometriosis (medical or surgical treatment and follow-up or immediately IVF treatment). A solid answer to the above dilemma requires data form prospective randomized trials in which infertile patients with endometriosis are allocated to proceed immediately to IVF treatment for a certain number of cycles or undergo surgical or medical treatment and expectant management for a certain period of time. Although such trials currently do not exist, indirect evidence, suggest that the fecundity is not improved with medical vs. placebo treatment (2) in patients with endometriosis. Moreover, it appears that the use of laparoscopic surgery in the treatment of minimal and mild endometriosis improves success rates (3), while pregnancy rates after laparoscopic treatment of endometriomas vary from 23-67% in follow-up studies (4-6).The question the current review focuses on is whether medical or surgical treatment of endometriosis is of value in patients for whom a decision has been taken to proceed to IVF in order to achieve pregnancy. Is there a need to treat endometriosis in patients undergoing IVF? The meta-analysis by Barnhart et al (7) showed that the chance of achieving pregnancy after IVF was significantly lower for patients with endometriosis (odds ratio, 0.56; 95% confidence interval, 0.44-0.70), as compared to those with tubal factor and it was accompanied by a decrease in fertilization rates, implantation rates and in the number of oocytes retrieved. Moreover, the probability of pregnancy was reduced in women with severe endometriosis as compared to those with mild disease. Although the above meta-analysis did not consider whether patients analyzed had been treated with medical or surgical treatment prior to IVF, it is reasonable to assume that if the probability of pregnancy after IVF is significantly decreased, then treatment of endometriosis immediately before the IVF cycle might be associated with an improved outcome. Medical treatment of endometriosis prior to IVF Medical treatment of endometriosis involves use of several agents, including oral contraceptives, or progestins. However, available studies evaluating medical treatment prior to IVF have so far focused on prolonged GnRH agonist treatment or use of danazol or gestrinone. Prolonged treatment with GnRH analogues The assumption for using prolonged GnRH analogue treatment, beyond the period of two-three weeks used in the classic long protocol, is that, in this way, initiation of ovarian stimulation is performed after significant remission of endometriotic disease has been achieved. This is mediated through the interference of GnRH agonists with paracrine and endocrine mechanisms, which are implicated in the pathogenesis of endometriosis (8). Several retrospective and prospective studies have evaluated the prolonged use of GnRH agonist downregulation in patients with endometriosis (Table 1). The control group in these studies received either no downregulation or was treated according to the short or long agonist protocol. Moreover, patients analyzed were diagnosed with various stages of endometriosis, while it is not clear if and what kind of treatment was applied prior to inclusion in the study. The majority of retrospective studies conclude that the reproductive outcome in women with endometriosis undergoing IVF is improved after prolonged downregulation with GnRH agonist before starting ovarian stimulation (Table I). This is also supported by two prospective studies performed and by one randomized controlled trial (RCT) (9), which compared prolonged downregulation to the long agonist protocol. The quality of that RCT, however, is questionable since the two groups of patients compared differed in the severity of endometriosis present, while the pregnancy rates achieved were unusually high. It is evident from the above that there is a need for well designed prospective RCTs that will address the question whether prolonged downregulation with GnRH agonists is associated or not with an increased probability of pregnancy. On the basis of the current low-quality evidence, it appears that such an intervention is beneficial. What needs to be accurately reported and taken into consideration in the design of future relevant trials is whether the patients allocated to receive prolonged downregulation have been treated already with surgical or medical therapy and the severity of endometriosis disease at the time of diagnosis and treatment initiation. It has to be noted though that prolonged administration of GnRH agonist results in hypo-estrogenemia which is associated with hot flushes, sweating, headache, mood changes, atrophy of secondary sexual tissues, and, most importantly with decrease in bone mineralization (10). The need for an add back therapy is considered necessary in these cases (11). A promising way to achieve prolonged downregulation appears to be the use of GnRH antagonists in weekly depot doses. Although antagonists have not been used as a treatment of endometriosis in patients scheduled to undergo IVF, they have been successfully used in the treatment of endometriosis associated pain. Their immediate action in combination with the lack of need for add back therapy (when used in weekly depot doses) brings them in an advantageous position as compared to GnRH agonists. Sequential treatment maintains basic estrogen production during treatment, while it does not influence the regression of the disease. Suppression of endometriosis prior to IVF without the use of GnRH analogs Suppression of endometriosis prior to initiation of ovarian stimulation for IVF has also been implemented with the use of danazol or gestrinone (12). However, no difference was shown in pregnancy rate after pretreatment for 6-9 months as compared to untreated patients with endometriosis (21% vs. 15%). Should endometriomas be removed in patients who are going to be treated by IVF? During investigation of infertility, diagnosis of endometriomas can be performed via laparoscopy and at the same time endometriomas can be removed. Endometriomas, however, can also be diagnosed by ultrasound without the need for a laparoscopy (13). Various methods have been employed for removal of endometriomas (14), including total resection and cauterization of the cyst wall. To show reliably, however, that treatment of endometriomas in patients scheduled for IVF has a beneficial effect on reproductive outcome, a prospective randomized trial in which patients with endometriomas are allocated to undergo removal of endometriomas or IVF needs to be performed. Such data do not exist to date. In the design of such a study, patients should be stratified according to whether the endometriomas present have already been treated and are not anymore present, have recurred following treatment or have never been treated. In addition, stratification should occur according to cyst size or localization to one or both ovaries. Arguments in favor of removing endometriomas
Studies to support removal of endometriomas prior to IVF Available data are based on retrospective studies comparing the reproductive outcome of patients with endometriomas who undergo surgical treatment to that of patients with no endometriosis (20-23) and appear to support that removal of endometriomas does not compromise IVF outcome. Moreover, Yanushpolsky et al (24) suggested that the presence of endometriomas at the time of oocyte retrieval is associated with increased rates of early pregnancy losses. A retrospective study by Suganuma et al. (25) compared treatment of endometriomas prior to IVF either by laparotomy/laparoscopy or aspiration with or without alcohol fixation to no treatment. A higher fertilization rate was observed in the group of patients treated with aspiration as compared to those treated with surgery or those who did not receive treatment. Arguments in favor of not removing endometriomas
Studies to support that removal of endometriomas is not necessary prior to IVF There is support from retrospective studies that IVF in the presence of endometriomas is not associated with a compromised outcome (30-33). On the other hand, evidence exists to support that surgery for ovarian endometriomas may damage ovarian reserve, potentially resulting in poor ovarian response to COH (34). In a prospective study Pabuccu et al (35) compared women with endometriomas resected, aspirated at the time of oocyte retrieval or left untreated and women with tubal factor infertility. No difference in the probability of pregnancy after IVF was observed between the groups compared. Moreover, removal of endometriomas was compared to non-removal by Garcia-Velasco et al (36) in a retrospective, matched case-control study. It was suggested that removal of endometriomas was associated with lower E2 and a higher requirement of FSH as compared to non-removal, and no differences in pregnancy rates (25.4% vs. 22.7%, respectively). CONCLUSIONS On the basis of retrospective studies, it appears that the use of prolonged GnRH agonist downregulation is beneficial in patients with endometriosis. No benefit from medical suppression of endometriosis by gestrinone or danazol prior to ovarian stimulation for IVF has been shown. A promising approach for medical treatment of patients with endometriosis prior to initiation of an IVF cycle appears to be the use of GnRH antagonists. There is a need for prospective randomized trials in which patients with endometriomas undergo surgical treatment or not to evaluate the usefulness of their removal prior to ovarian stimulation. Currently, it is not clear whether endometriomas should be removed or the patient should proceed immediately to IVF, although the latter may be the case, where recurrence of endometriomas occurs after previous excision (37). REFERENCES
Efstratios M Kolibianakis, M.D. Copyright © Middle East Fertility Society The following images related to this document are available:Photo images[mf06003t1.jpg] |
| |||||||||

{kind=link}