 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Diclofenac for analgesia in assisted conception: a prospective cohort study* Mashael Al Deery, M.D., A.B.O.G.,Kamal Jaroudi, M.D., F.R.C.S.C.,Saad Al Hassan, M.D., F.R.C.O.G., M.M.S.ci. (ART).,Rima Bazzi, M.D.,Abdulaziz Al Shahrani, M.D.,Khalid Awartani, M.D., F.R.C.S.C., F.A.C.O.G. Division of Reproductive Medicine, Department of Obstetrics and Gynecology, KingFaisalSpecialistHospital and Research Centre, Riyadh, Kingdom of Saudi Arabia To whom correspondence should be addressed: Khalid Awartani, MD, Department of Obstetrics and Gynecology, KingFaisalSpecialistHospital and Research Centre, MBC 52, P.O. Box 3354Riyadh11211, Kingdom of Saudi Arabia, Phone: 966-1-4427392, Fax: 966-1-4423765, Email: kawartani@kfshrc.edu.sa *This study was not funded. Received on May 18; 2005; Code Number: mf06008 ABSTRACT Objective: To assess the effectiveness of diclofenac in pain experience
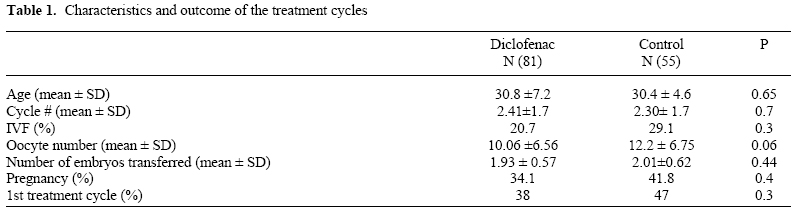
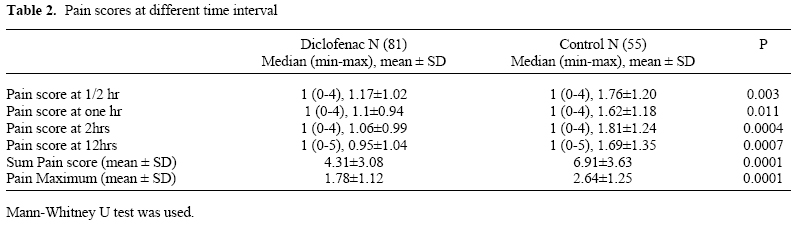
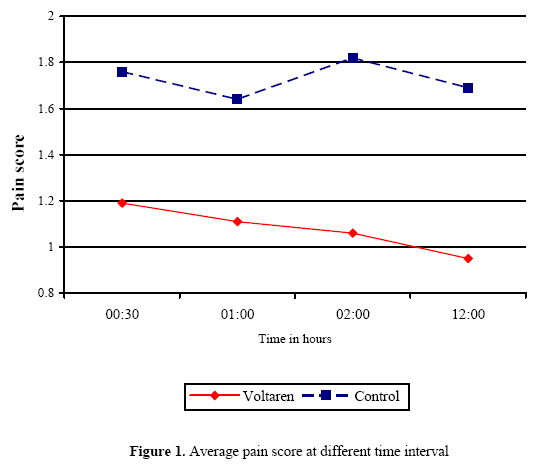
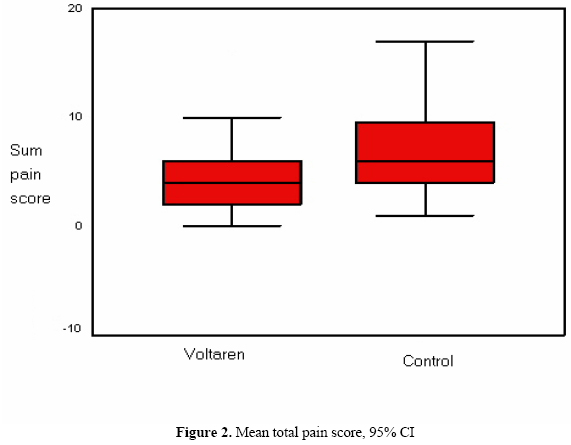
following oocyte retrieval under conscious sedation. Key Words: Analgesia, ART, Diclofenac, IVF In vitro fertilization is based on the ability to retrieve oocytes. Ultrasound guided trans-vaginal follicle aspiration is considered the standard of care for oocyte retrieval in assisted reproductive technologies (1) this technique for follicle puncture causes little trauma and few side effects (2). This is an outpatient day procedure performed either under general, regional, local anesthesia, conscious sedation or no anesthesia at all (1). The pain experienced during the procedure varies from individual to individual (2). Effectiveness of pain control after the procedure is an element of its successfulness (3). Hence, it is imperative to define forms of anesthesia/analgesia that minimize drug administration and unwanted side effects. Not less important for the patient is to have a positive experience with the anesthetic/analgesic regimen, in order to reduce procedure-associated stress in future occasions (4). Diclofenac sodium; is an intervention of proven value in post-operative pain control in day surgery practice (3). In minor gynecological surgery under general anesthesia, patients complaints complaints about post-operative pain and need for post-operative analgesia were less frequent in patients who received pre-operative intra-muscular nonsteroidal anti-inflammatory drugs, as compared to placebo (5). Although diclofenac has been commonly used for analgesia in some IVF centers (6), there is no published experience showing its effectiveness. The objective of this study was to assess the effectiveness of diclofenac when given as pre-medication for post-operative pain experience following oocyte retrieval under conscious sedation. MATERIALS AND METHODS This is a prospective non-randomized study, included 136 patients treated with IVF or ICSI, in the tertiary infertility unit at KingFaisalSpecialistHospital and ResearchCenter in Riyadh, Kingdom of Saudi Arabia, between September-December 2002. Patients were distributed into two groups according to the analgesia protocol given by their physicians, as practiced in our unit that all OPU procedures each day are done by one physician, the practice of half of our physicians is to give diclofenac to all the patients undergoing OPU in their assigned days, where the others do not give diclofenac. Group A (study group) received diclofenac (Tabiflex(r), Tabuk, Saudi Arabia) 100 mg per rectum 30 minutes prior to OPU, while group B did not (control); otherwise both groups were treated equally. Both study and control groups had alfentanil (Rapifen, Buckinghamshire, UK) 0.5 mg IV. Patients' allocation to study group or control group would depend on their procedure day. A FACES rating scales (7), is a pain rating scale consisting of six points (0-5) were 0 is no pain, and 5 is the worst pain (it is a subjective pain scoring system as the patient score her pain according to the facial expressions drawn in the scale paper given to her it is a reliable test). This scale has been the standard scale for pain assessment used in our institution. The recovery nurses instructed the patients on the OPU day how to use this pain recording scale, and then they were collected at the embryo transfer day (ET). FACES rating scales was used to evaluate the abdominal pain level 30 minutes, one, two, and 12 hrs post OPU. No extra analgesia was given to any patient of the two groups from pre-OPU till ET day. Our unit detailed patient stimulation protocols, oocyte retrieval, semen preparation, embryo culturing, and embryo transfer been published previously (8). Statistical analysis performed using S-plus 2000. Two-tailed t-test was used for parametric data, Mann-Whitney test for non-parametric data, and Chi-square test for binomial data. Sample size was calculated based on prior assessment of average pain score from a pilot project using the same analog pain scale, reduction of pain score by 30% in studied group compared to control group considered significant, and upon this calculated sample size was 53 patients in each arm, giving a power of 80% and P<0.05 was considered statistically significant. RESULTS In this prospective non-randomized study, 81 patients received pre-procedure diclofenac and 55 patients did not. The difference in number of patients between study and control group is from the model of patient distribution to the groups; which is depending on the different physician's assignment. Both groups had the same diagnosis categories. No difference in proportion of patients who had IVF treatment as the first cycle. Table 1 shows the characteristics of the women undergoing IVF/ICSI ET cycles. No differences in age, prior IVF treatment cycles, number of retrieved oocytes and number of embryos transferred, or pregnancy rate were found between the two groups. Table 2 shows the pain scores at different time intervals. The study group had significantly lower average pain score at 30 minutes post OPU (1.17) compared to the average pain score in the control group (1.76), P=0.003. This lower pain score in the study group continued to be observed at one hour (1.1 vs. 1.62, P=0.011), two hours (1.06 vs. 1.81, P=0.0004), and at twelve hours post OPU (0.95 vs. 1.69, P=0.0007). This reflect that the improvement in pain tolerance in the study group started immediately following the procedure and last up to a minimum of twelve hours post OPU when compared to the control group (Fig1). One patient in the control group had no ET because of total fertilization failure. The rate of multiple pregnancies was similar in both groups. (Figure 2) DISCUSSION Post-operative pain control is very important factor in patient satisfaction, especially in repeated procedure. In IVF/ICSI treatment; commonly the procedure needed to be repeated for more than one time, as the success rate around 30% per treatment cycle, with most of the programs advising their patients as this is a three cycles treatment outcome (9). Dropout of treatment cycles is not uncommonly seen (10), while other factors involved but positive patients experience might help in reducing this risk. Diclofenac is a non-steroid anti-inflammatory drug, been used empirically in many IVF programs without any control trails to prove efficacy (6). Both in animals and humans, prostaglandins are needed for successful implantation of the embryo through their own effect and interaction with platelet activating factors and cytokines, both in the uterus and in the embryo (11-13). Suppression of prostaglandin biosynthesis by NSAIDs in peripheral tissues, including those of the reproductive system, could therefore lead to abnormal implantation that predisposes an embryo to miscarriage, on the other hand the relaxing effect of NSAID on uterine contractility could be helpful for the embryo implantation (14). Although in humans NSAID use have been suggested to affect the implantation and the rate of pregnancy loss (15,16), but analysis of data from that report indicate that NSAID use for less than one week was not associated with increased risk of miscarriage (16), on the other hand low dose aspirin use in assisted reproduction was assessed in randomized controlled trials and did not show any deleterious effect on the pregnancy outcome (17,18). In our study no effect could be seen on the pregnancy rate in the patients used Diclofenac compared to control. Our data showed that 100 mg of diclofenac rectally 30 minute prior to OPU, reduced post OPU pain, without any significant side effect. This effect of diclofenac has been proven in other day surgery settings (3). Based in our data, we conclude that pre OPU diclofenac is an effective medication for post procedure pain control. And since that time diclofenac pre-OPU medication is the practice in our unit. REFERENCES
Copyright © Middle East Fertility Society |

{kind=link}
{kind=link}
{kind=link}
{kind=link}