 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Middle East Fertility Society Journal,Vol. 11, No. 1, 2006, pp.59-63 Intrauterine insemination: pregnancy rate and its associated factors in a university hospital in Iran Zahra Rezaie, M.D.,Ozra Azmodeh, M.D.,Neda Heydari Hamadani, M.D. MirzaKoochakKhanHospital, TehranUniversity of Medical Sciences, Tehran, Iran. Corresponding author: Zahra Rezaie: Department of Infertility, Mirza Koochak Khan Hospital, North Ostad Nejatollahi, Karim Khan Zand Blvd, Tehran 15978, Iran. Phone/Fax: #98-21-890 4172 Email: rezaizah@sina.tums.ac.ir Received on July 2, 2005; Code Number: mf06010 ABSTRACT Objective: To determine pregnancy rate and its
associated factors in Intrauterine Insemination (IUI) in a University ART
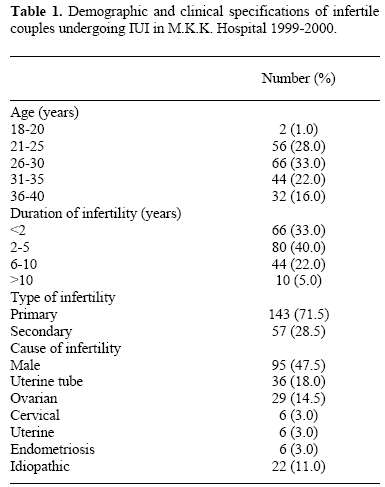
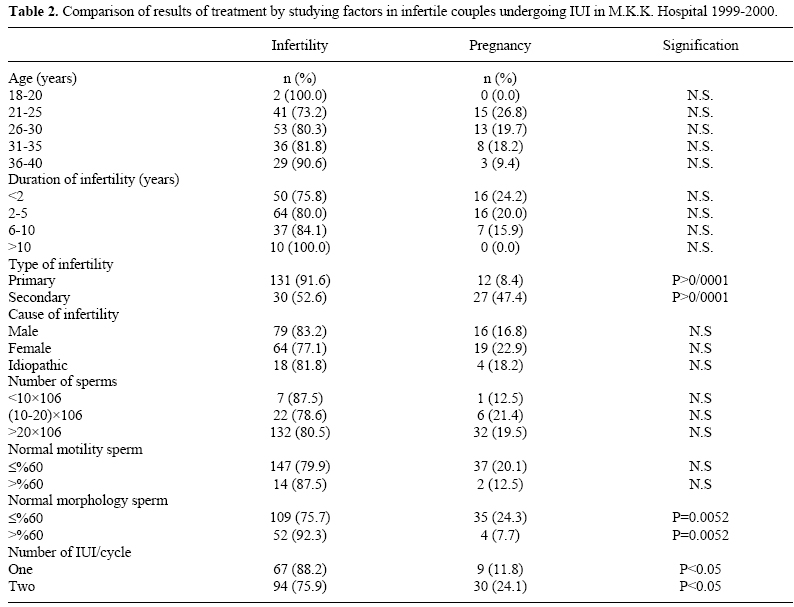
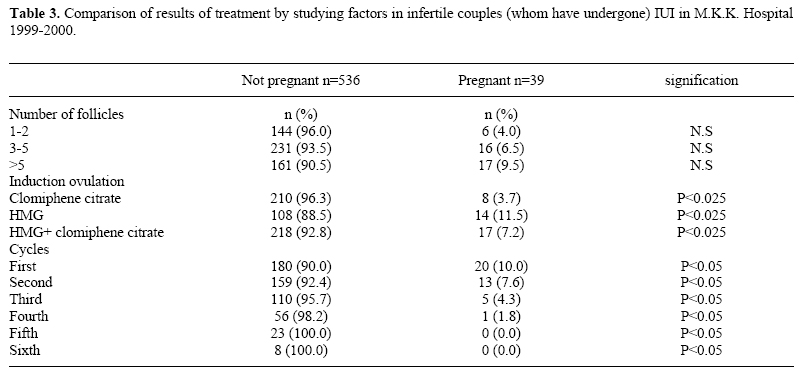
center in Tehran, Iran. Key words: IUI, pregnancy rate, infertility, ovarian stimulation. Intrauterine insemination is a common procedure used for the treatment of infertility. If it is performed based on appropriate indications and accurate protocol, it will be a convenient method (1, 2). IUI is easier, safer and inexpensive in comparison with other ART methods. The outcome of IUI is associated with some factors. Pregnancy rate per cycle of IUI ranges from 2.7% to 11.4 % (1,2). In some studies on IUI procedures, maternal age, number of IUI and cause of infertility were related to the success rate of pregnancy (3). Edward et al. reviewed 18 studies which used IUI and concluded that couples with less than 3 years duration of infertility, had highest chance to conceive (4). Plosker et al. performed 381 IUI cycles for 215 infertile couples, and reported that the pregnancy rate decreased when the maternal age or the number of treatment cycles increased (5). Evaluation of 610 IUI cycles on 174 infertile couples through the years of 1990-91, showed that the pregnancy rate is higher in younger women. Shorter infertility period, secondary and unexplained infertility have a higher rate of success. The number of motile sperms and number of IUI per cycle are other factors associated with success rate of treatment (6). Wang B et al. analyzed 186 patients and 216 cycles of IUI, and reported that IUI is of more applied value for male and cervical factor infertility. With these factors in mind, choosing the most suitable insemination time is the key to increasing pregnancy rate (7). Pregnancy rate was 12.8% per cycle for IUI in Mirza Koochak KhanHospital in the year 1996. Women 21-25 years old had highest pregnancy rate. (8) This study was conducted on 200 infertile couples who had undergone IUI procedure in Mirza Koochak KhanHospital during 1999-2000, to estimate the pregnancy rate in IUI and to determine the related factors for it. MATERIALS AND METHODS This retrospective descriptive study was performed on all infertile couples who had undergone IUI in the ART center of Mirza Koochak KhanHospital during the years 1999-2000. The medical records including, duration of infertility (years), type of infertility (primary, secondary), cause of infertility (male, female, idiopathic) number of sperms, motility, morphology of sperms, number of IUI per cycle, number of follicles, the type of induction of ovulation and the number of IUI cycles of these couples were reviewed then pregnancy rate and its associated factors were compared. The couples were considered eligible for this study if the necessary information were obtained from their medical records. The uncertain or uncompleted medical records were excluded form this study. Missing data from the medical records were completed by asking the subjects by calling their phone, if it was necessary. Every effort was made to maximize privacy of records. Statistical analysis was performed using SPSS software (version 10). The comparisons were performed using Chi-square test (a=0.05). RESULTS Two hundred infertile couples underwent 575 cycle of IUI. Women's ages ranged from 18 to 40 years with a median age of 27 years. The majority of subjects (73%) experienced maximum 5 years duration of infertility. 71.5% had primary infertility and male factor was the most frequent cause of infertility (95 cases, 47.5%) (Table 1). The pregnancy rates were 19.7% (39 cases) and 6.8% per patient and per cycle respectively. The highest pregnancy rate occurred in 21-25 years old women (26.8%) and the lowest occurred in women more than 36 years old (9.4%). There was no pregnancy in women less than 20 years old. The association between age and success rate was not statistically significant (p=0.081) (Table 2). Difference of pregnancy rate between primary (8.4%) and secondary infertility (47.4%) was significant (p<0.0001) (Table 2). The pregnancy rate decreased as the duration of infertility increased (From 24.2% for less than 2 years duration to 0.0% for more than 10 years duration of infertility) (p=0.076) (Table 2). The relationship between pregnancy rate and the cause of infertility was not statistically significant (p=0.076) (Table 2). The highest rate of pregnancy occurred in subjects with uterine factor infertility (33.3%) and the lowest (16.7%) occurred in patients with cervical and endometriosis factor. Pregnancy rate did not have any relation to sperm count and motility, but it was related to sperm morphology. When sperm morphology was more than 60% normal, pregnancy rate was 24.3% comparing to 7.7% when it was less than 60% normal (p=0.005) (Table 2). There was not any association between pregnancy rate and the number of large follicles (Table 3). Pregnancy rate was significantly higher when HMG was used for ovulation induction (11.5%), compared to 7.2% with "clomiphene citrate + HMG" or to using "clomiphene citrate" as the sole medicine for ovulation induction (P=0.025) (Table 3). Pregnancy rate was significantly higher with increasing the number of IUI per cycles, being 24.1% and 11.8% in two IUI per cycles and one IUI per cycle respectively (Table 2). The highest rate of successful pregnancy was achieved in the first therapeutic cycle (20 out of 200 cases, 10%), there was just one pregnancy (out of 57 cases, 1.8%) in the fourth cycle and no pregnancies occurred in the fifth and sixth repeated cycles (p<0.05) (Table 3). In this study 10 twin pregnancies (25.6%) occurred, and 42 (85.7%) of 49 newborns were low birth weight. No fetal congenital malformations occurred in any case. DISCUSSION Findings of this study were comparable to most other studies in this field. Pregnancy rate per couple was 19.7% and it was 6.8% per cycle in this study, comparing to anther study being 22.6% and 8% rates respectively (6). In another Mirza Koochak KhanHospital study, pregnancy rate was 21.6% per couple and 12.8% per cycle (8). In this study the rate of pregnancy decreased with increasing age, which is comparable to a previous study in our hospital (8) and also to other studies (2, 5, 6). Paulmyer LO, et al. concluded in their study that the pregnancy rate decreased with increasing infertility duration (2), which was the same conclusion as our study, and the study of Iberico G et al (9). Highest success rates occurred with infertility due to uterine factor, tubal and ovarian factors respectively. These finding were comparable to other studies such as Plosker SM study. The highest pregnancy rate occurred in women with ovarian factor in one study (5) and in female factor in a previous study in Mirza Koochak KhanHospital (8). In our study the pregnancy rate was more in secondary infertility and this agrees with the results of Edward E, et al. (4). Zhao Y et al. concluded that a forward open progression score of 3 to 4 in a processed specimen is necessary for IUI success (10). The relation between pregnancy rate and the number or motility of sperm was not confirmed in our study, which is not similar to others who reported a relation between pregnancy rate and number or motility of sperm (2, 6 and 11). In our study, the success rate was related to sperm morphology. Wainer R et al. in a retrospective study of 889 couples who did 2564 IUI cycles between Jan. 1991 and Dec. 2000 reported that sperm morphology, assessed before or after preparation, was not in itself a significant factor that affected the likelihood of IUI success (12). We had 9.5% success rate per cycle with more than five mature follicles comparing to 4% with 1 to 2 mature follicles, which was statistically non-significant. However Iberico concluded that the best results would be obtained with 2 or 3 induced follicles (9). Plosker SM, et al. stated that existence of at least two mature follicles is necessary for IUI therapy (5). We got better results with HMG usage for ovulation induction, than with clomiphene citrate + HMG. The least pregnancy rate was obtained when clomiphene citrate only was used for ovulation induction. Plosker SM, et al. also reported that using HMG is associated with better results (5) and Osia SH, showed highest pregnancy rate with HMG + HCG (8). The pregnancy rate was higher when 2 times IUI per cycle was performed, and the highest rate was obtained in the first IUI treatment cycle. These findings confirm previous results (2, 5,6). 25.6% of our pregnancies were twin, and no cases of fetal malformation occurred. This is satisfactory comparing it to Isaksson R, et al. study. They observed 25% of multiple pregnancy in their study and reported 18.2% of partial or complete fetal malformation (13). Finally we conclude that IUI is a convenient procedure for appropriate indications. We can obtain better results from this procedure with cases of secondary infertility, normal sperm morphology ?60% and with the use of HMG as ovulation induction agent. Also performing twice IUI per cycle increases the rate of success. REFERENCES
Copyright © Middle East Fertility Society |

{kind=link}
{kind=link}
{kind=link}