 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Middle East Fertility Society Journal,Vol. 11, No. 1, 2006, pp.64-69 Luteal phase support in in-vitro fertilization Shamma Thwaini Al Inizi, M.B.Ch.B., M.R.C.O.G., C.A.B.O.G. ,Magdy Asaad, M.B.B.Ch., F.R.C.O.G.,Juergen Schick, M.D., Ph.D., D.Sc. Department of Obstetrics and Gynecology, Fertility clinic, Tawam Hospital, Al Ain, Abu Dhabi, United Arab Emirates (UAE). Corresponding Author: Dr. Shamma Thwaini Al Inizi, Flat 1, Moor house, Abbey way, Barrow in Furness, Cumbria, LA14 1BP, UK. Tel. +44 7821708743 Email address: shammainizi@hotmail.com Received on May 18, 2005; Code Number: mf06011 ABSTRACT Objective: To compare the clinical pregnancy rate
after the use of human chorionic gonadotropin (hCG) injections (Profasi, Serono
Pharmaceuticals), to that after the use of oral Duphaston (Duphaston, Solvay
Pharmaceuticals B.V., Weesp, The Netherlands) , or vaginal Cyclogest
(Cyclogest, Cox Pharmaceuticals, Barnstaple, Ex32 8NS, England) used for luteal
phase support in in-vitro fertilization-embryo transfer (IVF-ET) cycles using
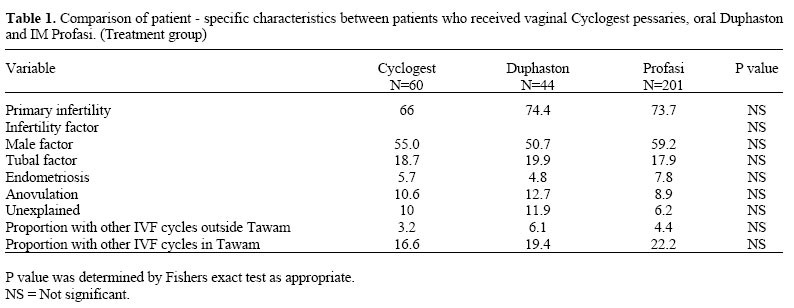
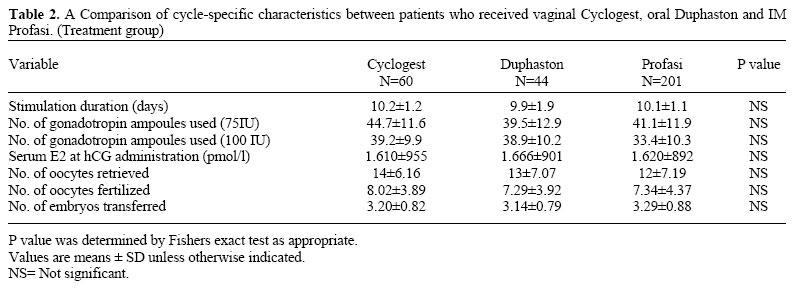
gonadotropin- releasing hormone agonist. Key words: luteal phase support, clinical pregnancy rate. Implantation is a complicated process that involves adequate preparation of the endometrium. An important contributor to this preparatory process is the corpus luteum; the primary function of which is to secrete progesterone to induce secretary transformation of the endometrium so that implantation can occur and the necessary support can be provided for the pregnancy during the early stages of its development (1). Adequate production of progesterone by the corpus luteum requires continuous stimulation by Luteinizing hormone (LH), which in pregnancy is produced by the action of hCG on LH receptors (2). Two mechanisms contribute to the need of luteal phase support, either by progesterone or by hCG to stimulate the corpus luteum to produce progesterone. This need is mainly caused by luteal phase disruption produced by aspiration of granulosa cells during oocyte retrieval. The second mechanism of luteal phase deficiency is caused by gonadotropin releasing hormone agonist (GnRH-a) used in the ovarian stimulation regimen to prevent premature LH surge. This results in persistent block of the LH output for at least ten days after discontinuing GnRH-a, which can result in impairment of progesterone secretion by the corpus luteum (3). This increases estrogen/ progesterone ratio, which is associated with an inhibitory effect on embryo implantation. All these factors indicate that luteal phase support with different modalities would be beneficial. There had been a debate about which type of luteal phase support is the most appropriate for IVF-ET cycles. Some authors suggested IM progesterone-in-oil as the best method of luteal phase support (4). Others suggested vaginal progesterone (5) while some claimed that both hCG and intra-vaginal progesterone are equally effective (6). Although a meta-analysis of randomized trials of luteal support has shown a preference for hCG (7), it can not be recommended in high responders at risk of ovarian hyperstimulation syndrome (OHSS). This study was conducted to compare the efficacy of different modalities of luteal phase support including oral, vaginal progesterone and hCG injections by comparing clinical pregnancy rates between the three groups. MATERIALS AND METHODS A retrospective cohort study was conducted at Tawam Hospital Fertility Clinic which included a total of 305 consecutive IVF-ET cycles. All patients included in this study were <40 years of age who had a stimulation cycle between January and May 2000. Patients undergoing ovulation induction cycles with or without insemination or frozen-thaw ET were excluded from the study. The three groups of patients were treated in an identical manner. All patients underwent down regulation with GnRH-a, Decapeptyl 3.75 mg IM (DTRP6, Decapeptyl, Ferring, Malmo, Sweden), given at day 21 of the preceding menstrual cycle. In oligo-ovulatory patients, GnRH-a was given after the initial treatment with oral Duphaston to induce withdrawal bleeding. Gonadotropin therapy was started after confirmation of adequate ovarian down regulation (no ovarian cysts of > 18 mm in diameter and estradiol (E2) levels of < 150pmol/l on day 2-3 of the cycle). Urinary or recombinant FSH or urinary HMG daily injections were used for ovarian stimulation in doses of 150-300 IU/day initially and were modified later according to the response. Profasi 10,000 IU was given IM. Once the diameter of the leading follicle reaches 18 mm oocyte retrieval was scheduled at 36 hours after hCG administration. All patients underwent trans-vaginal ultrasound- guided oocyte retrieval. Oocytes were inseminated with 0.25×0.35×106 motile sperm per milliliter if no male factor was present. Intra-cytoplasmic sperm injection (ICSI) was undertaken in cases of moderate to severe male factor infertility as previously reported (8). In mild male factor infertility or unexplained infertility the oocytes were divided into two groups for IVF and ICSI. Human tubal fluid supplemented with 10% synthetic serum substitute (Irvine scientific, Santa Ana, CA) was used for oocyte culture, fertilization and embryo culture. ET performed at 3-5 days and the remaining suitable embryos were frozen if the couple chose so. Our policy was to limit the number of embryos transferred to two, except in older women (age>37 years) or in case of multiple failures of implantation; three embryos were transferred. Patients were given the choice of which luteal support route they prefer, oral, vaginal or injectable. If they were considered at high risk of OHSS (e.g. previous history of OHSS, >12 oocytes collected, E2 on day of HCG administration >8,000pmol/l) they were not offered HCG. Women who preferred oral progesterone were those who did not like to have the vaginal soiling of Cyclogest and considered IM injections painful, while others were afraid to forget some oral Duphaston tablets and chose to use one of the other two medications. Luteal phase support included oral Duphaston (40 mg/day), vaginal Cyclogest (400mg pessaries twice/ day) or IM hCG (Profasi in a dose of 1500-2500 IU every second or third day for 3-5 doses). All were used after oocyte retrieval and continued until either a urinary pregnancy test (by a sensitive kit) performed 17 days after oocyte retrieval was performed or a period started. Only clinical pregnancies including sonographic demonstration of a gestational sac were counted. Data were gathered on age, type of infertility (primary or secondary), cause of infertility, number of prior assisted reproduction cycles (at Tawam clinic or other clinics), duration and type of gonadotropin stimulation, serum E2 level on the day of hCG administration, number of oocytes retrieved, number of oocytes normally fertilized (two pronuclei), number of embryos transferred and clinical pregnancy rate. E2 serum concentration was measured by microparticle enzyme immunoassay (MEIA), performed using the AX SYM system (Dainabol Co., Tokyo, Japan), an automated immunoassay analyzer specifically designed to accommodate MEIA (6). Blood samples were obtained on day 0, +7, +11, +15. The statistical evaluation was performed using student t test as appropriate. Difference was considered significant at p <0.05. Results are expressed as mean ± SD. RESULTS Three hundred and five consecutive IVF-ET cycles were included in the study from January- May 2000. 201 women (66%) used IM Profasi, 44 women (14.4%) used oral Duphaston and 60 women (19.6%) used vaginal Cyclogest for luteal phase support. There were no cycle cancellations in the study group. Patient specific characteristics were similar between the three groups (Table 1). Those who failed to reach ET stage either due to fertilization failure or significant risk or OHSS, were excluded from the study group. Cycle specific parameters including duration of stimulation, number of gonadotropin ampoules used, serum E2 at day of hCG administration, number of oocytes retrieved and those fertilized and number of embryos transferred, were all similar between the three groups of patients (Table 2). Clinical pregnancy rate was found to be similar in the three groups (24.9%, 28.3%.25% for Profasi, Cyclogest and Duphaston respectively), (P=1.000 and P=0.359). DISCUSSION Luteal phase supplementation with a variety of steroid hormones is necessary after ovarian stimulation cycles, which are preceded by GnRH-a down regulation (3,10, 11,12,13,14). Pregnancy rate was found to be significantly higher with progesterone use as luteal phase support compared to unsupported IVF-ET cycles (15). Different types of luteal phase support medications have been used including natural oral and vaginal progesterone supplementation, intramuscular progesterone and IM hCG. Results were variable regarding the best type of luteal phase support to use with a better clinical pregnancy rate. Damario et al reported that implantation efficiency is reduced when Crinone 8% vaginal progesterone gel rather than IM progesterone-in-oil is used for luteal phase support after IVF-ET cycles (4). Abate et al reported that the ongoing pregnancy and the live birth rates per transfer were significantly higher in patients supplemented with IM progesterone than those treated with vaginal progesterone gel and he concluded that IM natural progesterone appears to be the most suitable route of administration for luteal phase support in IVF-ET cycles (16). Others reported that vaginally administered progesterone results in adequate secretary endometrial transformation despite lower serum progesterone values than IM progesterone which is indicative of the first uterine pass effect and a better bio-availability in the uterus with minimal systemic undesirable effects and similar clinical pregnancy rate and that support beyond the serum pregnancy test may not be needed (17,18). Anserini et al also reported that vaginal progesterone gel is a good alternative to parental progesterone for luteal phase support in assisted reproduction cycles (ART) with similar clinical pregnancy rate (19). Friedler et al compared vaginal and oral progesterone used for luteal phase support and he concluded that clinical pregnancy rate was similar between the two groups with significantly higher implantation rate in the vaginal progesterone group. He recommended that low dose of micronized progesterone administered vaginally is simple, easy and well tolerated, so it can be the method of choice for luteal support especially for high responder patients at risk of OHSS. (5). It was reported that there is no significant difference in the outcome of IVF-ET cycles when different types of vaginal progesterone were used for luteal support including gel, pessaries and capsules (3,20,21). Human chorionic gonadotrophin was compared with vaginal progesterone for luteal support and it was found that pregnancy rate was similar between the two groups with equal effectiveness (6). Although earlier, Buvat et al reported that pregnancy rate was significantly higher in the hCG group compared to oral progesterone group used for luteal support but similar to the vaginal progesterone group (22). Daya et al concluded that there is no difference between hCG and progesterone use for luteal support in IVF-ET cycles (3). The optimal effective dosage for luteal support has not been established yet. In women lacking ovarian function and receiving estradiol, even a dose of progesterone as low as 45mg/48hours as given by sustained release vaginal gel, causes complete secretary changes in endometrial glands (day 20) and stroma (day 24) as indicated by endometrial biopsies. This was despite low (1-5 ng/ml) plasma progesterone concentrations (22). Some authors suggested the use of 200 mg×4/day of oral Utrogestan (Utrogestan, Basins Iscovesco (CTS), Paris, France) (5); others suggested 400mg/day of oral or vaginal micronized progesterone for luteal support (23). Pouly et al reported the use of 90mg of progesterone gel administered vaginally compared to 300mg/day micronized progesterone taken orally in a clinical phase III clinical trial involved seven European fertility clinics and found no difference in clinical pregnancy rate per ET (24). The present study evaluated the clinical efficacy of two types of progesterone used separately for luteal phase support in IVF-ET cycles which are oral Duphaston and vaginal Cyclogest, and compared the associated clinical pregnancy rate with that obtained by the use of IM Profasi. Examination of cycle- specific characteristics revealed no statistically significant difference in the parameters studied in the three groups. The ultimate outcomes of stimulation in the treatment groups in the study were similar including the mean E2 level at time of hCG administration, the mean number of oocytes retrieved and those fertilized. The mean number of embryos transferred was also similar in the three groups. We used 400mg twice daily of vaginal Cyclogest pessaries for luteal support in one group of patients and 40mg/day of oral Duphaston in the second group or HCG in the third group in a way similar to Buvat et al (22). The clinical pregnancy rate was found to be similar in the three groups which indicate that all the three medications used for luteal support are equally effective. This is supported by the findings of Norman et al , who reported that orally and vaginally administered progesterone have similar bioavailability (25). Buvat et al reported that when serum peak estradiol concentration was >2700 pg/ml, implantation rate was 5-6 times higher with vaginal administration compared to oral treatment (26 versus 5%), with similar clinical pregnancy rate which is the most important thing (22). The tendency to lower late luteal phase estradiol concentrations following oral administration could reflect a different pattern/rate of steroid metabolism as conception has occurred over a wide range of luteal phase estradiol/ progesterone ratio. This parameter may not have a clear predictive value regarding establishment of conception. This finding concurs with previous reports showing that endometrial morphology is not altered by extreme shifts in luteal phase estradiol concentration and estradiol/ progesterone ratios (5,26,27). Some authors suggested a combination of two medications for luteal support like hCG and progesterone. They claimed that this would increase clinical pregnancy rate in women with low mid luteal estradiol levels undergoing IVF-ET cycles (28). Others had suggested adding E2 to the progestin support regimen to improve pregnancy and implantation rates in cases when hCG is contraindicated (29, 30). A recent meta -analysis of randomized trials favored the use of hCG above progesterone for luteal phase support with respect to pregnancy rate in IVF cycles and suggested further prospective randomized trials to determine a definite consensus with respect to the duration of luteal phase support in IVF cycles (31). We concluded that as clinical pregnancy rate was found to be similar in the three groups of women using different medication for luteal support, it remains the woman's choice to choose the type and route of administration of luteal support medication. Progesterone whether used orally or vaginally, is the method of choice for luteal support in case of high responder patients at risk of OHSS. These results are affected by the number of the cycles studied being small and by the study design being retrospective. Our results suggest the need for a prospective randomized controlled trial comparing vaginal Cyclogest, oral Duphaston and IM hCG for luteal support in IVF-ET cycles. REFERENCES
Copyright © Middle East Fertility Society |

{kind=link}
{kind=link}