 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
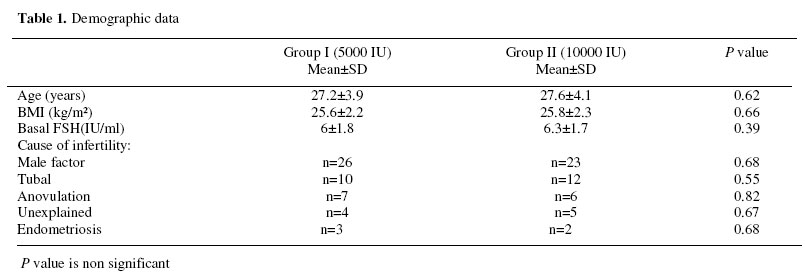
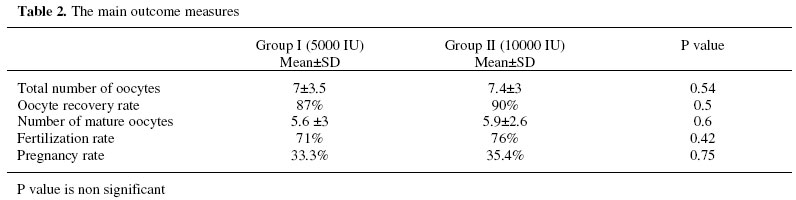
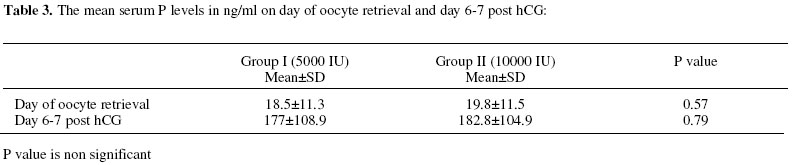
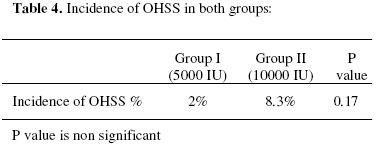
Middle East Fertility Society Journal Vol. 11, No. 2, 2006, pp. 99-103 Does triggering ovulation by 5000 IU of uhCG affect ICSI outcome?* Amany A.M. Shaltout, M.D., Mohamed S. Eid, M.D., Amal A. Shohayeb, M.D. Dr Samir Abbas Medical Center,Jedda ,KSA; and Department of Obsterics and Gynecology, Cairo University. *Presented in the ESHRE meeting in Prague: June 20, 2006. Correspondence: Amany Shaltout, Dr Samir Abbas Medical Center (IVF unit), Jeddah , P.O. box 12190, KSA.Tel.009662- 653 0000 Ext 270.E-mail:amanyshaltout@hotmail.com Received on May 28, 2006; Code number: mf06019 ABSTRACT Objective: To evaluate the effect of 5000 IU as compared to 10000 IU of uhCG on the outcome of ICSI cycles. Key words: ovulation induction, hCG, ICSI Human chorionic gonadotropin belongs to the same glycoprotein family as FSH ,LH and TSH. All members of this family share the same alfasubunit, but have different beta subunits. However, the molecular similarity between hCG and LH is such that the first 114 amino acids of each compound share 80% homology and hence both are capable of stimulating the same hormone receptor (1). In spontaneous and stimulated ovarian cycles , ovulation occurs 36-38 hours after the onset of the LH peak (2,3,4).Modern assisted reproduction treatment protocols commonly use gonadotropin – releasing hormone agonists for pituitary down regulation, which suppress endogenous gonadotropin production, improving folliculogenesis and inhibiting the endogenous midcycle LH surge. This has resulted in fewer cancelled cycles, higher number of oocytes and more pregnancies (5-7). Due to its structural similarity to LH uhCG has been used for over 40 years to induce final follicular maturation and subsequent ovulation in infertility treatment as a surrogate LH surge (8). In ovarian stimulation cycles, I.M. administration of 10,000 IU u hCG has long been accepted as the standard dose for triggering of ovulation. The aim of the present study was to evaluate the effect of 5000 IU as compared to 10000 IU of uhCG used to induce final follicular maturation and subsequent ovulation, on the outcome of ICSI cycles. As a secondary outcome measure the incidence and severity of OHSS between both groups was also assessed. MATERIALS AND METHODS This prospective randomized double blind clinical trial was conducted from the period June 2004 to December 2004 in Dr Samir Abbas Medical Center, Jeddah, KSA. One hundred patients scheduled for ICSI were recruited for the study. Inclusion criteria included: age<35 years, BMI<30 kg/m2 and basal FSH<10 IU/l. Patients were excluded from the study if they had: PCOS, history of severe OHSS, or history of previous cancellation due to poor response. Long down-regulation using gonadotropin releasing hormone agonist(GnRHa), (Decapeptyl, Ferring) was started in the mid-luteal phase of the preceding cycle and was confirmed on the first day of the treatment cycle by serum LH levels <2 IU/l and serum estradiol (E2) <50 pg/ml with ultrasound scan showing no ovarian cysts. Ovarian stimulation with 2-3 ampoules of 75 IU human menopausal gonadotropin (Menogon, Ferring) was then started and the dose was adjusted according to response and continued until one follicle was ≥18 mm and at least 2 other follicles ≥ 16 mm with serum E2 level of ± 150 pg/ml per follicle. Two patients were withdrawn from the study before randomization, 1 had OHSS while the other had poor response. A total of 98 patients were then randomly divided ( using sealed envelope) into 2 groups: group I (n=50) received 5000 IU and group II (n=48) received 10000 IU uhCG (Profasi, Serono) via intramuscular route. Transvaginal oocyte retrieval was done 36 hours later. The retrieved oocytes were assessed for maturity and ICSI was performed for all cases. Up to 3 embryos were transferred to the uterine cavity 2-3 days later. Luteal phase support using progesterone vaginal suppositories (Cyclogest 400 mg ) was started on day of oocyte retrieval and serum pregnancy test was performed 16 days post oocyte retrieval. The main outcome measures were: the total number of oocytes retrieved, oocyte recovery rate (total number of oocytes retrieved divided by the number of follicles of at least 14mm diameter on day of hCG), number of mature oocytes, fertilization and pregnancy rates. The secondary outcome measures were the serum progesterone (P) on day of oocyte retrieval and 6-7 days post hCG and the incidence and severity of OHSS. Statistical Analysis Data was presented as percentages, means and standard deviations. Student t-test was used for comparison of means while the chi squared (x2) was used for comparison of proportion, P value of <0.05 was considered significant. All statistical calculations were done using Microsoft Excel Version 7 (Microsoft Cooperation, NY, USA). RESULTS A total of 98 patients were enrolled for the study and were randomly divided into 2 groups: group I (n-50) and group II (n-48). There was no statistically significant difference (mean± standard deviation) between patients in group I and II regarding age (27.6± 4.1 versus 27.2±3.9), BMI (25.8±2.3 versus 25.6 ±2.2 kg/m2) and basal FSH (6.3±1.7 versus 6±1.8 IU/l) respectively (Table 1). Two patients in group I were cancelled after hCG administration. No oocytes were retrieved in one patient, while the second patient had no fertilization of her oocytes. A total of 48 patients in group I completed the study. There was no statistically significant difference between both groups regarding oocyte recovery rate (87% versus 90%) ,total number of oocytes retrieved (7±3.5 versus 7.4±3), number of mature oocytes (5.6 ±3 versus 5.9±2.6) fertilization rate (71% versus 76%) and pregnancy rate (33.3% versus 35.4%), respectively as shown in Table (2). Regarding serum P on day of oocyte retrieval it was (18.5±11.3 versus 19.8±11.5) while on day 67 post hCG it was (182.8±versus 177 ±108.9), there was no statistically significant difference between both groups (Table 3). Four patients in group II (8.33%) developed OHSS as compared to only 1 patient (2%) in group I (Table 4). All cases were in the form of mild OHSS (9) with mild GIT symptoms, abdominal distention and enlarged ovaries. Although the risk of OHSS was 4 times greater in group I as compared to group II, yet this difference was not statistically significant. DISCUSSION Human chorionic gonadotrophin induces a number of critical physiologic changes in anticipation of ovulation and subsequent fertilization. These actions can be broadly categorized as induction of follicular rupture, luteinization, and resumption of meiosis (10,11).In ICSI cycles successful oocyte retrieval is the most direct measure of hCG efficacy as it integrates a cascade of intrafollicular events necessary for ovum release from the follicle. In addition, an elevated serum progesterone level in the post ovulatory period is an established biochemical indicator of the effect of hCG. Although hCG has been commercially available for more than 40 years, yet only very few studies have been performed to assess the optimum dose in female patients. In our study 5000 IU was as efficacious as 10000 IU of uhCG as indicated by the oocyte recovery rate, the total number of oocytes retrieved, the number of mature oocytes and the fertilization and pregnancy rates, which were of no statically significant difference between both groups. In addition ,there was no significant difference between both groups regarding the serum P levels on day of oocyte retrieval and 6-7 days post hCG. This agrees with the findings of Abdalla et al. (12) , who performed a prospective randomized study to evaluate the minimal effective dose of u hCG in IVF. hCG was administered at doses of 2000, 5000, and 10000 IU in 88, 110, and 104 cases, respectively. There was a significant difference in successful oocyte recovery in the 2000 IU as compared with the other 2 groups. The rate was, however, similar in the 5000 IU (95.5%)and 10000 IU (98.1%) groups. Our study also agrees with Wikland et al (13), who performed a prospective randomized trial to compare the SC and IM route of 5000 IU versus 10000 IU of uhCG in an IVF program. There were no significant differences in the oocyte maturity rate in 8 (5000 IU group) and 10 (10000 IU group) SUZI cycles between either the 2 different doses or the routes of administration. There were 79% (SC) and 85% (IM) mature oocytes in the 5000 IU group and 78% (SC) and 86% (IM) in the 10000 IU group. There was no significant difference in the fertilization rate 53% (SC) and 52% (IM) in the 5000IU group versus 53% (SC) and 52% (IM) in the 10000 IU group, while the pregnancy rate was 36% (SC) and 39% (IM) in the 5000IU group as compared to 48% (SC) and 37% (IM) in the 10000IU group, which again was of no significant difference. Another study was done to evaluate the influence of BMI as well as having the patient administer 5000 IU of uhCG to herself in comparison to a healthcare professional on IVF outcome (14).Results showed that there was a statistically significant difference between patients with BMI ≥ 26kg/m2 (n=50) as compared to those with BMI 18-25 kg/ m2 (n=50) regarding serum hCG level on the day of retrieval (63.9±7.3U/L versus 99.6±U/L). This was associated with a significant difference in all other parameters; number of oocytes retrieved (11.8±versus 16.1±3.9), oocyte: follicle ratio (33.9 versus 41.7), number of oocytes fertilized (5.8± 0.7 versus 8.1± 1.1), fertilization rate (46.2% versus 61.3%) and clinical pregnancy rate (26.6% versus 37.1%).The administration of uhCG by the patient herself or a healthcare professional had no effect on the outcome of any of the parameters. The authors concluded that in obese patients a higher dose of hCG (10000 IU) should be used for final follicular maturation. The secondary outcome measure in our study was the incidence and severity of OHSS. Four patients in 10000 IU group (8.33%) developed OHSS in comparison to only 1 (2%) in the 5000 IU group and all were mild cases. Although the risk for developing OHSS in group II was 4 times that in group I yet this difference was not significant, most probably due to the small sample size. This is contrary to a study done on high responders in which 5000IU uhCG was given IM to 47 patients with E2 levels ≥2500 pg/ml but <4000 pg/ml in comparison to 3300 IU given to 47 patients with peak E2 levels ≥4000 pg/ml but <5500 in order to decrease the incidence of OHSS(15). Four patients in the 5000IU group developed mild OHSS in comparison to 3 in the 3300 IU group, while the 5000IU group had only one case of moderate OHSS and no cases of severe OHSS. However the 3300IU group had 5 cases of moderate and 2 cases of severe OHSS. Despite decreasing the dose of hCG yet the risk of OHSS was not eliminated. The authors explained this by the fact that there was no consistency between the patient characteristics in both groups where the 3300 IU group were younger, had higher peak E2 levels in response to stimulation, had a great mean number of oocytes retrieved and a greater mean number of mature oocytes. The authors recommended that a further study might compare patients with similar demographics and ovarian responses randomized to one of two lowered doses of hCG to determine whether the dose of 3300 IU hCG is equally efficacious to 5000IU in similar patient populations. CONCLUSIONS 5000 IU of uhCG is as effective as 10000 IU for triggering of ovulation, with the added advantage of lesser incidence of OHSS which is the most serious complication of ovulation induction. We therefore recommend optimizing the triggering dose of uhCG at 5000 IU, especially in young lean patients undergoing ovulation induction for infertility treatment. REFERENCES
© Copyright 2006 - Middle East Fertility Society The following images related to this document are available:Photo images[mf06019t1.jpg] [mf06019t2.jpg] [mf06019t4.jpg] [mf06019t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}