 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Middle East Fertility Society Journal Vol. 11, No. 2, 2006, pp. 104-108 Detection of Ureaplasma urealyticum and Mycoplasma hominis in endocervical specimens from infertile women by polymerase chain reaction Shahin Najar Peerayeh, Ph.D. , Mortaza Sattari, Ph.D. Department of Microbiology, School of Medical Sciences, Tarbiat Modares University, Tehran, Iran Correspondence: Najar Peerayeh, Dpt. of Microbiology, Schoolof Medical Sciences, Tarbiat Modares University, Tehran, Iran. Fax:+98-21-88013030.E-mail:najarp_s@modares.ac.ir Received on April 9, 2006; Code number: mf06020 ABSTRACT Objective: Ureaplasma urealyticum and Mycoplasma hominis are commonly found in the genitourinary tract as the causative agents of several sexually transmitted diseases, reproductive failure, and neonatal morbidity and mortality. We have used a polymerase chain reaction (PCR) for the detection of these mycoplasmas in endocervical samples from infertile women. Key words: Ureaplasma urealyticum, Mycoplasma hominis, infertility, PCR Ureaplasma urealyticum and Mycoplasma hominis are most prevalent in the genital tract of sexually active women. U. urealyticum can be found in the cervix or vagina of 40-80% of asymptomatic women and M. hominis in 20- 50%(1,2). The presence of genital mycoplasmas in a large proportion of healthy women complicates the assessment of the pathogenic roles of these organisms, but several studies have indicated that genital colonization of the genital mycoplasmas can be associated with an increased risk of developing certain pathogenic conditions and pregnancy abnormalities, e.g., pelvic inflammatory disease, pyelonephritis, premature rupture of membranes, chorioamnionitis, and preterm labor and birth. In addition, they may be acquired by neonates either in utero or by vertical transmission at birth and can cause pneumonia, pulmonary hypertension, chronic lung disease, and meningitis of the newborn (3-6). In addition, infection with genital mycoplasmas has been linked with infertility (7-10). Diagnosis of mycoplasma is usually made by serological determination or in vitro isolation of the organism. However, serological procedures are often hampered by interspecies cross-reaction, while cultivation is time-consuming and hard to do for some fastidious mycoplasmas. Use of mycoplasma species-specific DNA probes made it possible to discriminate between different species, this method proved to be rapid and specific (11). This study used a polymerase chain reaction (PCR) to determine the colonization rate of U. urealyticum and M. hominis in genital tract of infertile women. Table 1. Nucleotide sequences of the primers used
Clinical specimens; Between February 2003 and August 2003, endocervical swab samples were taken from a total of three hundred and seventy seven infertile women, ranging in age from 17 to 45 years, in infertility clinics of Tehran city. From patients a detailed history was obtained, and all complaints concerning the genital tract, such as vaginal discharge and cervicitis were recorded. DNA extraction from specimens: DNA was extracted from standard strains (U.urealyticum serotype VIII and M. hominis PG 21 were kindly provided by Statns Serum Institute of Copenhagen, Denmark) and clinical samples as described previously by Cadieux et al (12). Briefly, 1ml of the sample was centrifuged at 12000 ×g for 10 min. The pellet washed in PBS and resuspended in 50µl of distilled water. After boiling for 10 min, an aliquot of 7µl was used directly in PCR experiments. PCR assay: PCR reactions were performed with an automated thermalcycler (Eppendorf, USA). Specific oligonucleotide primers were used for U.urealyticum and M. hominis(Table 1). These were chosen in published nucleotide sequences: in the urease gene for U.urealyticum (13) and in the 16S rRNA gene for M. hominis(14). Amplification was performed in 50µl of reaction mixture containing 10µl of 10× PCR buffer, 2.5 mM Mgcl2, 200µM dNTP, 1.25 units of Taq polymerase, 20pmol of each primer and 7µl of sample DNA. The reaction mixtures were placed in thermalcycler. The thermal profile involved an initial denaturation step at 94C for 3min followed by 30 cycles of denaturation at 94C for 1min, primer annealing at (52C for U.urealyticum and 62C for M. hominis) for 1min, and primer elongation at 72C for 1min. The cycling was followed by a final extension step at 72C for 10min. Aliquots of amplified samples (10µl) were analyzed by electrophoresis on a 1.5% agarose gel stained with ethidium bromide. Statistical analysis Chi-square (X2) test was used for the generation of P<0.05 values. Table 2. Detection of Mycoplasmas from infertile women by PCR
*25 of patients were PCR positive for both of microorganisms Table 3. Distribution of the genital mycoplasmas in accordance to patient’s ag
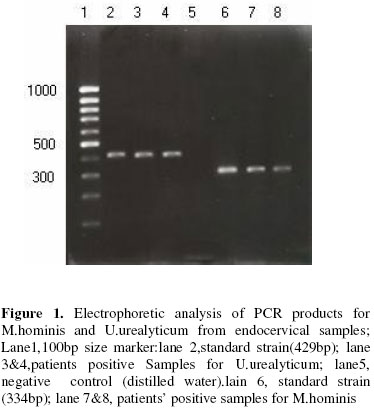
*25 of patients were PCR positive for both of microorganisms RESULTS Of the 377 patients studied, 116(30.7%) were positive for U.urealyticum, M. hominis or both genital mycoplasmas (Table 2). Of these 116 patients, 60 (51.7%) were PCR positive only for U. urealyticum, 31(26.7%) were PCR positive only for M. hominis and 25(21.5%) presented both organisms. A photograph of electrophoresis based on bromidestained agarose gel for PCR-amplified products from the Mycoplasmas strains is presented in fig 1. DNA from the 16S rRNA sequences that is amplified by the PCR primers used in this study shows at 334bp (M. hominis). A 429bp fragment of the urease gene was amplified for identification of U. urealyticum. In this population, 29% of the women presented with signs or symptoms, such as vaginal discharge (29%), cervicitis (19%) and abortion (17%). When relating mycoplasmas with those clinical features, these microorganisms were detected in 27% of the patients with vaginal discharge (M. hominis in 5% of women, U. urealyticumin 12% and both microorganisms in 10%). In women with abortion, genital mycoplasmas were identified in 28% (M. hominis in 7%, U. urealyticumin 15% and both microorganisms in 6%). Mycoplasmas also were detected in 32% of patients with cervicitis (M. hominis in 15%, U. urealyticumin 11% and both microorganisms in 6%). There was an association of the presence of M. hominis and cervicitis in patients (P<0.1). The age of the patients from who were PCR positive varied from 17-45 with a mean age of 31 years. Distribution of the genital mycoplasmas in accordance to patient’s age is presented in table 3. NO significant difference was found between the age of patients whose sample was PCR positive (positive group) and that of the other patients (negative group). There was also no difference regarding the duration of infertility, vaginal discharge, and abortion, between the positive and the negative group. DISCUSSION In this study, 30.7% of 377 infertile women were colonized with genital mycoplasmas as detected by PCR. U. urealyticum(22.5%) has been shown to be more frequently detected in women than M. hominis(14.8%). Other studies using PCR for detecting genital mycoplasmas in endocervical specimens have reported prevalence rate as high as 40 to 80% for U. urealyticum and 20-50% for M. hominis(1,2,6,15). Since genital mycoplasmas have been found significantly associated with low socioeconomic background, such as poverty, number of sexual partners, and use of contraceptive drug (15-19), it is not surprising that the rate of genital mycoplasmas was lower in our study. Although differences were not statistically significant, but the isolation rate of genital mycoplasmas were higher in women under 30 years of age that is consistent with that previously described by others (15, 16, 18, 20). At present, the main method of detecting genital mycoplasmas is by culture, but the cultivation of mycoplasmas is laborious, time consuming, and requires specific expertise. PCR is revolutionizing the diagnosis of many infectious diseases, particularly those caused by organisms that are difficult to cultivate. PCR is a more sensitive and reliable means of detecting genital mycoplasmas in the endocervical specimens; its results can be available within a day, compared with 2-5 days for culture. Although the precise role of genital mycoplasmas in human infertility has not been firmly established, there is strong support in the literature for causal role in the cases of women and men infertility (21-30). In addition, genital mycoplasmas have been implicated in several maternal complications of pregnancy and in neonatal morbidity and mortality. They may play roles in endometritis, chorioamnionitis, premature rupture of membranes, prematurity, low-birthweight infants, postpartum fever, and they may be important causes of pneumonia and meningitis in very low-birth-weight infants. Therefore the specificity, the exquisite sensitivity, and the rapidity of PCR make this technique most valuable in the diagnosis of genital mycoplasmas infections. REFERENCES
Copyright © Middle East Fertility Society The following images related to this document are available:Photo images[mf06020t2.jpg] [mf06020t3.jpg] [mf06020t1.jpg] [mf06020f1.jpg] | |||||||||||||||||||||||||||||||||||||||||||||||
| |||||||||

{kind=link}