 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Middle East Fertility Society Journal Vol. 11, No. 2, 2006, pp. 1119-126 Cytomegalovirus and the expression of immunological markers in reproductive failure Wafaa M. Aboul Enien, M.D * Nashwa A. Abou Khedr, M.D.†,Amal Z. Azzam, M.D * Nagwa G. Rizk, M.D. †,Tarek A. Karkour, M.D. * Department of Obstetrics and Gynaecology, and Medical Microbiology and Immunology, Faculty of Medicine, Alexandria University, Alexandria, Egypt * Department of Obstetrics and Gynecology, Faculty of Medicine,
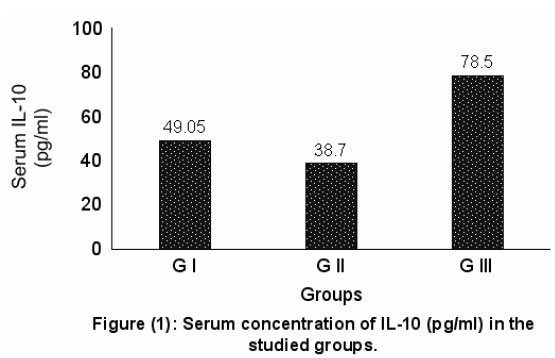
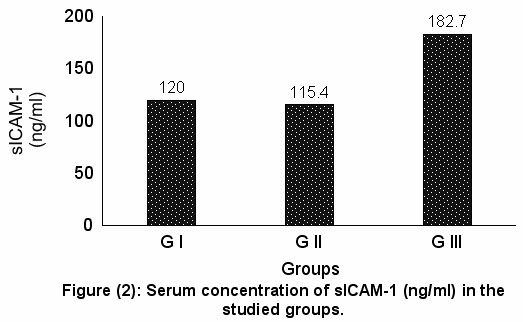
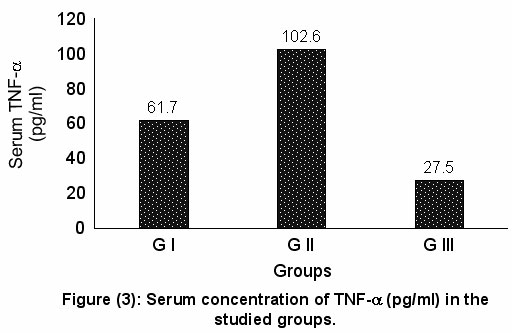
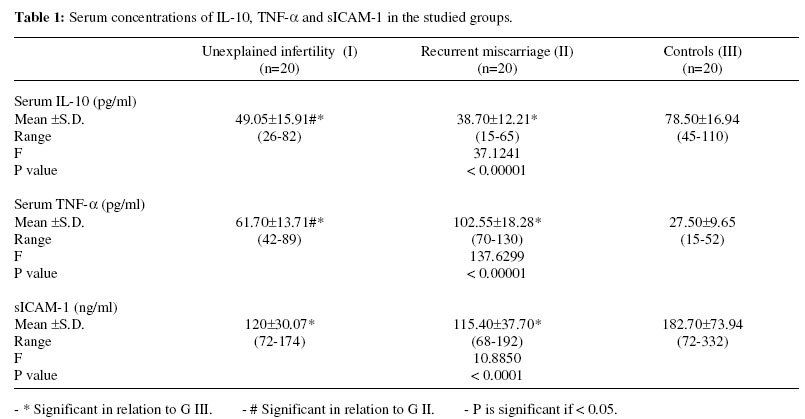
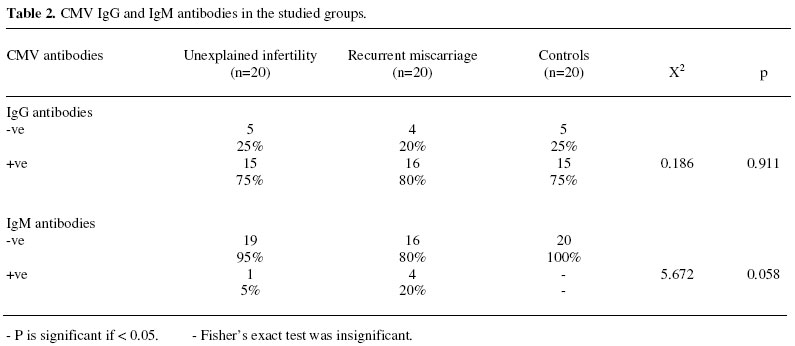
Alexandria University. Received on January 16, 2006; Code number: mf06023 ABSTRACT Objective: To assess the relation of cytomegalovirus (CMV) infection and serum interleukin 10 (IL-10), tumor necrosis factor-α (TNF-α) and soluble intercellular adhesion molecule 1 (sICAM-1) with reproductive failure. Keywords: Cytomegalovirus, interleukin-10, tumor necrosis factor-α, intercellular adhesion molecule-1, reproductive failure. Immunological factors operate at almost every step in reproduction. Immune infertility may result from destruction of gametes by antisperm or antiovarian antibodies, inhibition of sperm-zona pellucida binding, prevention of embryo cleavage or by alterations in implantation mediated by cellular and humoral responses (1). Moreover, the majority of evidence strongly suggest that a breakdown in immunological maternal-fetal interactions may lead to recurrent or occasional fetal loss (2). The immune system has two effector arms: humoral (antibody-mediated) immunity and cellular (T cell-mediated) immunity. This dichotomous nature of the immune system is determined by CD4+ Thelper/ inducer lymphocytes. Following activation by antigen, CD4+ T cells produce one of two cytokine profiles, leading to their classification as T-helper 1(TH1) and T-helper 2(TH2) cells (3). TH1 cells induce several cell-mediated cytotoxic and inflammatory reactions via interleukin 2 (IL-2), interferon-gamma (IFN-γ) and tumor necrosis factor-α (TNF-α). TH2 cells are involved in humoral immunity via TH2-type cytokines, IL-4, IL-5, IL-6, IL-9, IL-10 and IL-13 (4). TH2-type immunity is proposed to be the normal profile contributing to successful pregnancy and a shift towards TH1- dominance may play a role in reproductive failure (5). The mechanisms by which the mother accepts the implanting fetus as an allograft remain unexplained. Mononuclear cytotrophoblasts, the specialized cells of the placenta that invade the uterus, play an important role (6). Cytotrophoblasts secrete IL-10, the immunosuppressive cytokine that modulates immune responses, helping to protect the fetal hemiallograft from rejection. IL-10 is involved in the maintenance of normal pregnancy, perhaps by suppressing IFN-γ and TNF-α production by TH1 cells (7). Moreover, IL-10 may influence the histocompatibility leucocytic antigen (HLA) class I expression pattern at the feto-maternal barrier, contributing to the maternal tolerance of the allogenic fetus (8). Human cytomegalovirus (CMV) is often detected at the uterine-placental interface, impairing cytotrophoblast differentiation and invasion. Infected cytotrophoblasts express CMV IL-10 which upregulates human IL-10 and decreases matrix metalloproteinase-9 activity, an enzyme which degrades the extracellular matrix and increases the depth of invasion (9). The diminished degradation of extracellular matrix could contribute to the shallow invasion of the uterus and restriction of fetal growth in pregnancies affected by CMV (10). Although the mechanisms causing reproductive failure remain speculative, recent evidence suggests that a specific uterine immune-endocrine network play a pivotal role in the continuation of pregnancy. Soluble intercellular adhesion molecule-1 (sICAM-1), a cytokine inducible molecule is released by the endometrium in a hormonedependent manner and is able to interfere with several immunological responses. Its reduced levels in some patients with unexplained recurrent miscarriage may reflect the presence of an altered immunological environment during early gestation (11). The aim of the present study was to assess the relation of CMV infection and serum IL-10, TNF-α and sICAM-1 with reproductive failure. MATERIALS AND METHODS Blood was collected by venipuncture from the following groups of patients recruited from the Department of Obstetrics and Gynaecology, El-Shatby University Hospital, Alexandria: Group I: Women with unexplained infertility (n = 20, mean age 31 years, range 20-35 years, mean duration of infertility 5 years, range 2-9 years). Infertility work-up included semen analysis, luteal progesterone evaluation, hysterosalpingo-graphy and/or laparoscopy. Group II: Women with a history of at least three consecutive spontaneous miscarriages before 20 weeks gestation (n = 20, mean age 32 years, range 20-35 years), mean number of previous pregnancy losses was 3 times (range 3-6 times). None of the women were pregnant at the time of sampling. All women were evaluated according to a standard protocol that included thorough history and physical examination, karyotype on both partners to exclude parental chromosomal errors, hysterosalpingography followed by laparoscopy/ hysteroscopy if indicated to exclude anatomic abnormalities, serum assays for TSH, prolactin, midluteal progesterone and finally antiphospholipid antibodies. No presumed etiology was detected. Group III: Included twenty healthy fertile women (controls) who had no history of reproductive problems (mean age 30 yrs, range 20-35 years). All had at least one living child and their pregnancies proceeded uneventfully. -All women in the study were in good health, had no history of allergy and were not taking any medications at the time of blood sampling. -Sera were separated from all samples by centrifugation and stored at -20 °C until time of assay. All serum samples were frozen and thawed once. -Concentrations of IL-10, TNF-α and sICAM-1 were measured using enzyme-linked immunosorbent assays (ELISA). All kits except the sICAM-1 detection kit were obtained from Immunotech (Marseilles, France). Soluble ICAM1 kits were obtainedfromR &Dsystems (Minneapolis, MN, USA). The manufacturer’s protocols were followed, and recombinant reference cytokine samples served as positive controls for calibration. Each serum sample was monitored in duplicate. The sensitivity of each of the assays was 10 pg/ml for TNF-α, 5pg/ml for IL-10 and 0.35 ng/ml for sICAM-1. The presence of serum anti-CMV IgM and IgG antibodies were also determined by ELISA. Statistical analysis Data were coded and fed to SPSS/Win (Version 6.4). Data were presented as number, percentage, mean and standard deviation ( Correlation coefficient Chi-square test was used to test the association between variables (IgG, IgM antibodies), and if not valid, Fisher’s exact test was done. 5% level of significance was chosen. RESULTS Sixty patients were recruited for this study; twenty with unexplained infertility, twenty with a history of recurrent miscarriage and twenty fertile controls. The patients’ age did not differ significantly between groups (p = 0.113). Serum samples from all patients were examined for IL-10, TNF-α and sICAM-1. The three biochemical parameters were detectable in all patients of the studied groups. Levels of serum IL-10 were significantly lower (p < 0.00001) in unexplained infertility (mean = 49.05, SD = ±15.91, range = 2682 pg/ml) and recurrent miscarriage patients (mean = 38.70, SD = ±12.21, range = 15-65 pg/ml) compared to controls (mean = 78.50, SD = ± 16.94, range = 45-110 pg/ml), Fig (1). Soluble ICAM-1 production was also significantly decreased (p < 0.0001) in unexplained infertility (mean = 120, SD = ±30.07, range = 72174 ng/ml) and recurrent miscarriage patients (mean = 115.40, SD = ±37.70, range = 68-192 ng/ml) compared to controls (mean = 182.70, SD = ±73.94, range = 72-332 ng/ml), Fig (2). However, levels of TNF-α were significantly higher (p < 0.00001) in unexplained infertility (mean = 61.70, SD = ±13.71, range = 42-89 pg/ml) and recurrent miscarriage patients (mean = 102.55, SD = ±18.28, range = 70-130 pg/ml) compared to controls (mean = 27.50, SD = ±9.65, range = 15-52 pg/ml), Fig (3). Data is presented in Table I. There were no significant correlations between IL-10, TNF-α and sICAM-1 in each of the three studied groups. Table II demonstrates the incidence of CMV antibodies in the three studied groups. CMV IgG antibodies were detected in 15 patients with unexplained infertility (75%), 16 recurrent miscarriage patients (80%) and 15 fertile controls (75%). There was no significant difference in the incidence of CMV IgG antibodies between groups (p = 0.911). CMV IgM antibodies were detected in only one patient with unexplained infertility and in 4 recurrent miscarriage patients. No CMV IgM antibodies were detected in controls. Although there was an apparent increase in the incidence of CMV IgM antibodies in the recurrent miscarriage group compared to the other studied groups, this did not reach statistical significance (p = 0.058). DISCUSSION Recurrent spontaneous miscarriage (RSM) is a common complication of pregnancy that affects 2% of women in the reproductive age. Although genetic, anatomic and hormonal causes have been implicated in its etiology, more than 60% of cases remain unexplained (12). Immunological rejection of the fetus due to recognition of paternal antigens by the maternal immune system, resulting in abnormal immune cells and cytokine production, is postulated to be one cause of unexplained pregnancy loss (4). Various immuno-logical abnormalities have also been reported in infertile women who had implantation failures after multiple in vitro fertilization (IVF) cycles (13). Cytokines are important mediators in the interaction between the maternal immune system and reproductive system. Cytokines do not act in isolation but form a complex regulatory network in which modulatory interactions maintain homeostasis between the fetal unit and maternal immune system. This complex interplay between maternal and fetal immune mechanisms changes temporally as pregnancy progresses. If this delicate balance is adversely affected, immunoregulatory mechanisms may be insufficient to restore homeostasis and thus lead to reproductive failure (14). In the current study, serum levels of IL-10 were significantly lower in the patient groups compared to controls. This is in agreement with previous reports (5,7,15). Decreased production of IL-10 by decidual T cells of women with RSM compared with those of normal pregnancy has also been reported (16). Moreover, IL-10 was found to be produced at higher concentrations by peripheral blood mononuclear cells of women with normal pregnancy compared to those with a history of RSM (17). Furthermore, IL-10 was reported to play a positive role in the prevention of spontaneous pregnancy failure in a mouse model. The injection of IL-10 into abortion prone mice resulted in the prevention of fetal wastage (18). Thus IL-10 has emerged as an important TH2 type anti-inflammatory cytokine in the maintenance of normal pregnancy. It is known to selectively suppress the detrimental TH1 mediated cellular immunity by inhibiting the production of inflammatory cytokines as IFN-γ, TNF-α and IL-1 while maintaining humoral immunity vital for maternal defense against pathogens (7). Progesterone production could be responsible at least in part for the increased production of TH2 type cytokines implicated in the maintenance of successful pregnancy (18). Concerning the TH1 cytokine TNF-α, its level in serum was significantly elevated in the patient groups compared to controls. This is in accordance with previous studies (15,17,19) suggesting that TNF-α might be locally produced by activated endometrial lymphocytes and macrophages in response to trophoblast or sperm antigens then diffuses into the systemic circulation. Moreover, previous reports (5) investigating the expression of intracellular TH1 and TH2 cytokines demonstrated that the ratio of TNF-α to IL-10 expressing peripheral blood lymphocytes was persistently elevated in women with RSM and infertility due to implantation failures after IVF compared to fertile controls. However, this contradicts a recent study by Shimada et al (20) who reported a significantly lower TH1/TH2 ratio in peripheral blood of recurrent aborters provoking a new controversy on TH1/TH2 balance in the etiology of RSM. TNF-α is an important immunoregulatory cytokine with detrimental effects on implantation, embryo development and fetal survival. It suppresses trophoblast proliferation possibly by inducing apoptotic changes in these cells (21). In mice, TNF-α has been shown to have potent deleterious effects on pregnancy (22). It is suggested that TH1 cytokines trigger thrombotic and inflammatory processes at the maternal uteroplacental blood vessels by activation of vascular endothelial cell procoagulant (23). By contrast, TH2 cytokines inhibit TH1 induced tissue factor production by monocytes (24). Concerning sICAM-1, its level in serum was significantly lower in RSM and unexplained infertility patients compared to controls. This is in accordance with a study by Gaffuri et al. (11) stating that the expression of sICAM-1 by cultured endometrial stromal cells in the luteal phase of the cycle was significantly lower in abortion prone patients compared to controls. ICAM-1, one of the major adhesion molecules in the immune system, is strongly expressed at both protein and mRNA levels in endometrial stromal cells and is able to mediate their interaction with lymphoid cells. A number of inflammatory cytokines as IL-1, TNF-α and IFN-γ are capable of inducing cell activation and up-regulating the expression of ICAM-1 on the surface of various host cells including those of the human endometrial vasculature (25) Soluble ICAM-1, a shedding form of ICAM-1 disturbs the adhesion between immune cells and their targets thereby preventing an immunological reaction(26). It could play different roles in pathological mechanisms of human endometrium observed in endometriosis, spontaneous miscarriage and infertility (27). Our results of serum IL-10, TNF-α and sICAM1 contradicted a study by Schust et al. (28) reporting that serum levels of selected TH1 type, TH2 type cytokines and sICAM-1 were not associated with pregnancy outcome in women with RSM. One potential reason for the apparent discrepancy between our results and this study was that in our study, sera were collected from women with a history of RSM, whereas in the latter study, sera were collected from pregnant women after documentation of fetal cardiac activity for later comparison of pregnancy outcome. Since serum cytokines are metabolized rapidly, it is not surprising that local cytokine-mediated events at the maternal-fetal interface were not reflected in peripheral sera. Furthermore a recent study by Shimada et al. (29) reported that TH1/TH2 cell balance in RSM women did not differ from controls and that immunodystrophism was detected as diminution of the TH cell population rather than TH1 predominance. In the current study, the presence of serum anti CMV antibodies was studied in patient groups and controls. Most of the studied women manifested the presence of serum IgG anti CMV antibodies with no significant difference between groups. Moreover, serum IgM anti CMV antibodies were only present in the patient groups with no significant difference between RSM and unexplained infertility women. This agrees with previous reports (30,31) that did not support human CMV as a major abortion-related factor. Despite the established implication of human CMV in congenital infection, there are still conflicting reports regarding its association with spontaneous miscarriage. A study by Radcliffe et al(32) reported a significantly lower prevalence of serum anti CMV antibodies in RSM patients compared to fertile controls. In contrast, other studies (33,34) revealed a high prevalence of IgG anti CMV antibodies in women following spontaneous abortions. This suggests that abortion might result from fetal infection due to reactivation of chronic CMV infection during the course of pregnancy. Hence, peripheral serum levels of selected TH1type (TNF-α) and TH2-type (IL-10) cytokines and sICAM-1 might play an essential role in the pathophysiology of RSM and unexplained infertility. If this hypothesis is true, attempts at immuno-modulation may be of clinical importance. Indeed both immunomodulation and hormonal support (progesterone or hCG supplements) have been used to improve the live birth rate in recurrently aborting women and in those with implantation failures. Each may modulate the balance between various cytokines. However, neither hormonal support nor immunopotentiation has been proven to be beneficial. It is believed that molecular and cellular defects specific approaches should be used, tailored for the specific pathway whose disruption cause the clinical symptom (35). REFERENCES
Copyright © Middle East Fertility Society The following images related to this document are available:Photo images[mf06023f2.jpg] [mf06023t1.jpg] [mf06023f3.jpg] [mf06023t2.jpg] [mf06023f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}