 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
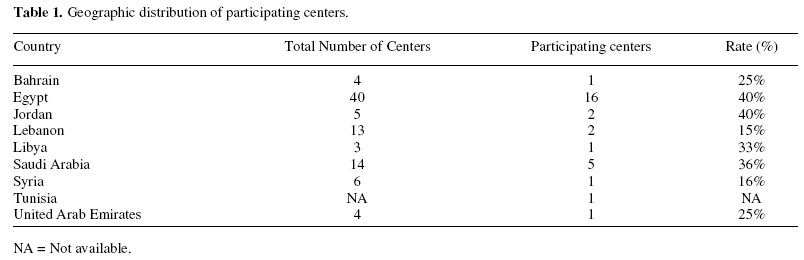
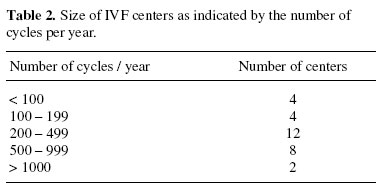
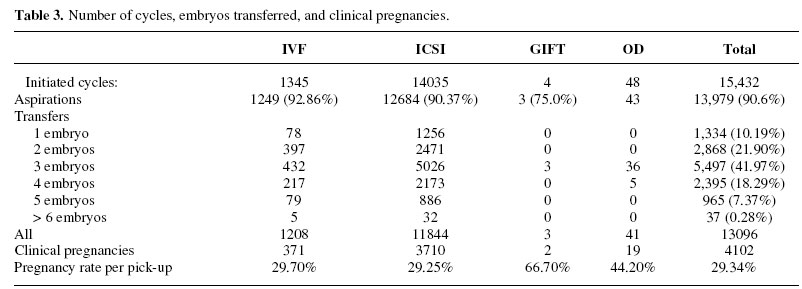
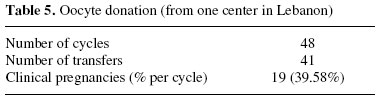
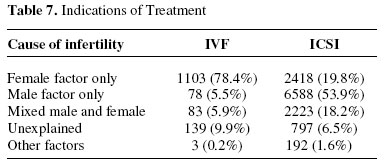
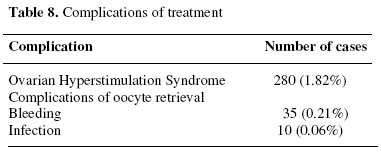
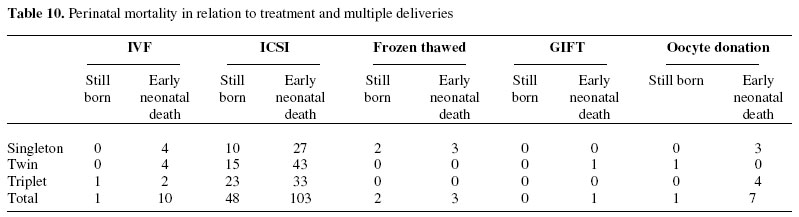
Middle East Fertility Society Journal, Vol. 11, No. 3, 2006, pp. 145-151 EDITORIAL Results of Assisted Reproductive Technology in 2001 generated from the Middle East IVF registryRagaa T. Mansour, M.D., Ph. D. Ahmed M. Abou-Setta, M.D. The Egyptian IVF-ET Center, Maadi, Cairo, Egypt Correspondence: Ragaa T. Mansour, M.D., Ph. D., The Egyptian IVF-ET Center, 3, Street 161, Hadayek El Maadi, Cairo, 11431, Egypt, Telephone: (+202) 5254944, Fax: (+202) 5253532, E-mail: ivf@link.net; ragaaivf@hotmail.com Received on September 9,2006; revised and accepted on October5,2006 Code Number: mf06027 ABSTRACT Objective: To summarize the results of ART procedures cycles initiated in the Middle East during the year 2001. Key words: Middle East, IVF, ICSI, Registry data, ART results INTRODUCTION Ever since the introduction of the first center to accommodate in-vitro fertilization (IVF) in the Middle East almost twenty years ago, the IVF technique has become much more acceptable as a means of procreation among the medical community, patients, and society. Currently, for example, in Egypt alone there are 52 known operating IVF centers. This number is only a fraction of the centers functioning in the Middle East area as a whole. Due to the widespread IVF practice in the Middle East, a regional registry to represent Middle East IVF centers became a necessity. Even though, until today there are no official governmental or governmentally affiliated bodies responsible for developing or maintaining an IVF registry in any individual Middle Eastern country. In addition, there are no specific requirements, or guidelines, for the reporting of data to any national IVF registry. However, like any other new modality of treatment, reporting of data is very important for evaluation of the efficiency of the treatment and estimation of the relative risk, which leads to continuous modifications in an attempt to improve the risk/ benefit ratio. This report for the year 2001 is the second consecutive Middle East IVF Registry publication for the Middle East data on assisted reproduction technology (ART). In 2004 the first report of the Middle East IVF Registry was published for cycles performed during the year 2000 (1). In addition the data from the previous registry has been incorporated in the World IVF Registry 2000 (2). MATERIALS AND METHODS In an effort to collect data for the year 2001, all IVF centers in the Middle East were contacted through E-mails, faxes, phone calls, and personal contacts. The ‘World Report on ART’ forms, prepared by the International Committee for Monitoring Assisted Reproductive Technologies (ICMART), were distributed to all the centers, with a covering letter setting a deadline to collect the completed anonymous forms. Completed forms were collected from the respective centers via E-mail and/ or through regular mail. Each center was given a unique serial number and country code, and the original information pertaining to the sender was concealed. Data was then extracted, compiled, and analyzed on a pre-made MS Excel spreadsheet. Data entry was confirmed by double entry and comparison to the original forms received. The present report summarizes data from assisted reproductive treatments started during 2001. The data includes treatments from standard in vitro fertilization (IVF), intracytoplasmic sperm injection (ICSI), and frozen embryo replacement (FER) following standard IVF and ICSI, gamete intra-fallopian transfer (GIFT), and oocyte donations (OD) performed during the period of January 1, 2001 till December 31, 2001. Follow-up data on pregnancies and deliveries are cohort data; being collected collectively after the outcome of all pregnancies was determined. RESULTS Response Rate Data were received from thirty centers for the year 2001 and none were excluded. The geographic distribution and response rate of centers is shown in Table 1. Size of ClinicsThe size of the centers, as indicated by the number of cycles per year, is shown in (Table 2). As in previous years, center sizes in the Middle East show a parametric distribution. In addition, most of the centers still remain the category from 200 – 499 cycles per year. Number of Treatment CyclesThe total number of cycles performed was 16,293. Table 3 shows the number of initiated and pick-up cycles, the number of embryos transferred and the number of clinical pregnancies (CPR). ICSI constituted 86.14%, IVF constituted 8.26%, while the frozen-thawed embryo replacement cycles represented only 5.28% of the total number of ART cycles. As for standard IVF, the clinical pregnancy rate per aspiration and per transfer was 29.70 and 30.71%, respectively. The corresponding rates for ICSI were 29.25 and 31.32%, respectively. The results of frozen-thawed cycles are shown in Table 4. Only a few centers provided data for cryopreservation of embryos. The frozen-thawed cycles represented only 5.28% from the total number of ART cycles. Oocyte donation was only reported by one center in Lebanon (Table 5). Age DistributionThe women's age at the time of retrieval is shown in Table 6. It is obvious from the results that women’s age groups ‘< 29 years old’ and ‘30 – 34 years old’ constituted the largest age groups undergoing ART, with a combined total of over 64% of cycles. Even though, there is also a trend for IVF/ ICSI in older women, with a large number of women aged 35 – 39 (25.75%) also attempting IVF. Moreover, women aged forty years and older represented 10.35% of all cycles. Indications for ARTThe indications for ART are shown in Table 7. The male factor of infertility alone, or in association with other factors, still remains the largest indication for undergoing assisted reproduction. This represented 65.85% of all indications for IVF/ ICSI in 2001. Risks of TreatmentThe complications, such as ovarian hyperstimulation syndrome, bleeding and infection, are shown in Table 8. Ovarian hyperstimulation syndrome still remains high, with OHSS occurring in 1.82% of initiated cycles. In addition, there was a reported occurrence of bleeding in 0.21% and infection in 0.06% of all aspiration cycles. Pregnancies and Deliveries after TreatmentThe numbers of deliveries are shown in Table 9. Perinatal mortality is shown in (Table 10). Data on deliveries and malformations are incomplete due to inadequate follow-up. Only a few centers reported on the incidence of chromosomal aberrations, and/or malformations, in IVF babies. These chromosomal aberrations and congenital malformations are presented in Table 11. DISCUSSION The present report for the year 2001 is the second consecutive report to cover ART data of treatment cycles in the Middle East. Thirty centers voluntarily provided data on 16,293 cycles performed between January 1, 2001 and December 31, 2001, which is similar compared to the year 2000. Furthermore more centers are expected to participate in the future registries since they did not have data, or did not yet operate, in 2001. In 2001, the Egyptian IVF Registry was formed in order to help gather information on the benefits, risks, and success rates of assisted reproduction in Egypt as a whole (3). It was created as a nongovernmental group independent of any current organization or society. Its primary role was to create and maintain the Egyptian IVF Registry and disseminate information pertaining to the benefits and risks involved with assisted reproduction in the Egypt. In October 2003, a workshop was conducted in Cairo, Egypt in collaboration with ICMART and WHO in order to disseminate tools for data collection and train people to develop national and regional IVF registries. All IVF centers in the Middle East were invited to join and participate. The program was designed to provide an overview on the already existing national (e.g. Egyptian IVF Registry) and regional registry models (e.g. ESHRE registry in Europe and the SART/ CDC registries in the USA) and also to formulate a plan of action to establish the Middle East IVF registry. One hundred and thirty nine infertility specialists representing 97 IVF centers from 14 countries in the Middle East participated in the workshop. At the end of the meeting, the Middle East IVF Registry was agreed to be formed in order to help gather information on the benefits, risks and success rates of assisted reproduction in the Middle East. It was agreed to be an autonomous independent of any current organization or society, as its Egyptian counterpart. Its primary role was to create and maintain the Middle East IVF Registry and disseminate information pertaining to the benefits and risks involved with assisted reproduction in the Middle East. This current report is the result of the second round of data collection and analysis. It represents the data for the year 2001. The women's age at the time of oocyte retrieval demonstrated that women aged < 29 and 30 -34 years old still remained the largest two groups undergoing ART in 2001 (Table 5). Even though, there is also a trend for IVF in older women. Women aged 35 -39 constituted around one fourth of all women undergoing ART. The group of women above 40 years constituted 10.3% of all groups, which is a relatively high rate. As for the numbers of cycles performed, the year 2001 showed a slight decrease as compared to the year 2000. This is mainly contributed to the new distribution of centers that have sent in their data. Even though the number of contributing centers is similar between the years 2000 and 2001, several centers that reported in 2000 did not contribute in 2001. The gap was filled by new centers that began their contribution in 2001. This is an example of some of the problems faced by voluntary registries. Unfortunately, as noted by the numbers of transferred embryos, there is still a problem with transferring a large (>3) number of embryos per transfer cycle, with 25.9% of all women undergoing transfer receiving at least four embryos. Furthermore it is generally apparent that the optimum targeted number of embryos was three, with 42.0% of all women receiving this number. Lastly, only 32.1% of women received only single, or two embryos, per transfer. It is not clear if these were intentional low-number transfers, or if it was due to a lack of available embryos for transfer. It is also notable that ICSI represented about 86.14% of ART cycles for the year 2001. This represents a significant predominance of ICSI as compared to standard IVF practice in the Middle East. If we compare these figures with the indications of ART cycles we may find an explanation. The female factor only as a cause of infertility represented only 25.8% of cases attempting ART cycles. On the other hand, male factor alone, or in combination with other factors, represented 65.85% of the cases. In addition, the patients pay for the treatment cycle totally on their own. There is no insurance coverage or governmental aid for IVF. Therefore, most centers would prefer ICSI to avoid total fertilization failure unexpectedly in some cases. The multiple delivery rates were still high in both IVF and ICSI. Twin deliveries represented 20.6% in IVF and 25.5% in ICSI. In addition, triplet and high-order deliveries represented 4.1% of all IVF and ICSI cycles in 2001. This is a reflection of the relatively high number of embryos transferred per cycle in all age groups. In the year 2001, 41.97% of the transfer cycles received 3 embryos, 18.29% received 4 embryos, and 7.7% received 5 or more embryos. It is clear that the rates of multiple pregnancies are high due to the transfer of >3 embryos per cycle in The Middle East, coupled with the limited availability of cryopreservation. This limited availability may play a strong role in favor of transferring these large numbers. Furthermore, the financial constraints and lack of medical insurance coverage makes it difficult for most of the patients to afford repeating the cycle. The reported frozen-thawed embryo replacement cycles represented only 5.28% of the total number of ART cycles. This reflects the very limited practice of cryopreservation as indicated by the fact that only a few centers provide this service. Until recently, cryopreservation was not even mentioned as an allowed procedure by the local organizing authorities in different countries in the Middle East. The complications reported were mainly ovarian hyperstimulation syndrome, which occurred at a rate of 1.82%. This is a relatively high incidence compared to the reported incidence of 1.0% of all stimulated cycles in 25 countries in Europe, as indicated by the ESHRE registry (4). Ovarian hyperstimulation syndrome is a preventable disease and more strict precautions have to be taken for prevention. Bleeding occurred in 0.21% of aspiration cycles. In addition, infection was also rare, occurring in only 0.06% of all aspiration cycles. The data on malformation is very deficient. Only a few centers provided information on the number of babies born with congenital malformation, or abnormal karyotyping for the babies. This is both a result of the poor follow-up of babies born after IVF and due to the financial constraint of routine karyotyping of the offspring. In summary, this is the second in an annual series of publications reporting the cumulative results of the work of the Middle East IVF Registry for the year 2001. Thirty centers participated in the registry reporting 15,432 fresh cycles, with an overall clinical pregnancy rate of 29.34%; and 861 frozen cycles with an overall clinical pregnancy rate of 17.2%. The multiple pregnancy and delivery rates were high, with 28.35% of deliveries being twins, triplets or high-order. The problem of multiple pregnancies needs to be resolved by reducing the number of embryos per transfer and improving the practice of cryopreservation. Rigorous efforts for the prevention of OHSS are also required. Finally, better recording systems and follow-up of pregnancies and deliveries will improve the quality and accuracy of the registry. REFERENCES
Appendix 1. Middle East IVF registry (2001) participating centers
Copyright © Middle East Fertility Society The following images related to this document are available:Photo images[mf06027t8.jpg] [mf06027t6.jpg] [mf06027t10.jpg] [mf06027t4.jpg] [mf06027t1.jpg] [mf06027t11.jpg] [mf06027t5.jpg] [mf06027t2.jpg] [mf06027t3.jpg] [mf06027t9.jpg] [mf06027t7.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}