 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Middle East Fertility Society Journal, Vol. 11, No. 3, 2006, pp. 152-168 REVIEW Biological and reproductive implications of stem cell research and therapeutics: prospects in the Middle East Noha A. Mousa, M.D. Mohamed A. Bedaiwy, M.D. Robert F. Casper, M.D. Reproductive Sciences Division, Department of Obstetrics and Gynecology, University of Toronto, Toronto, Canada Correspondence: Mohamed Bedaiwy, M.D., Toronto Centre For Advanced Reproductive Technologies (TCART), 150 Bloor St W, Suite 210, Toronto, Ontario, M5S 2X9, Canada and the Division of Reproductive Sciences, Fran and Lawrence Bloomberg Department of Obstetrics and Gynecology, University of Toronto, and Samuel Lunenfeld Research Institute, Mount Sinai Hospital, 600 University Avenue, Room 876, Toronto, Ontario M5G 1X5, Canada (FAX: 416-972-0036). Email addresses: bedaiwymmm@yahoo.com, RFcasper@aol.com Received on October12,2006; Code Number: mf06028 ABSTRACT
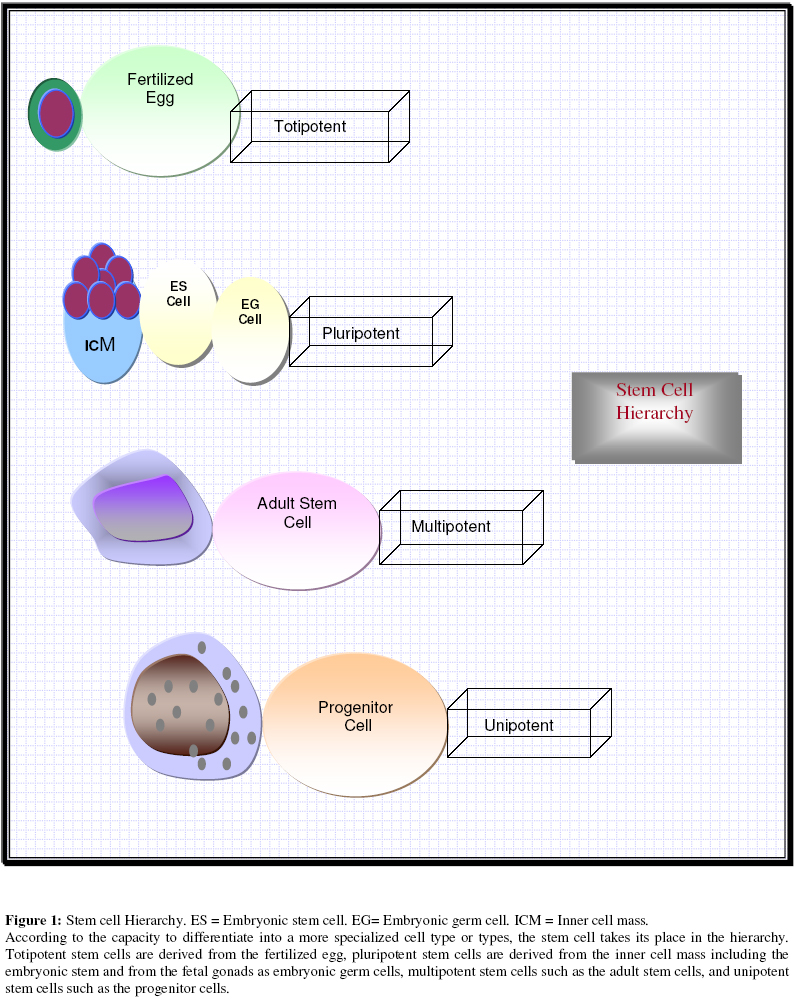
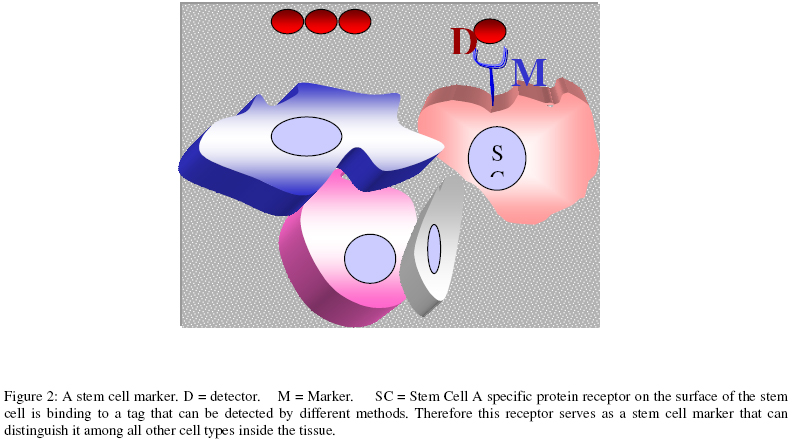
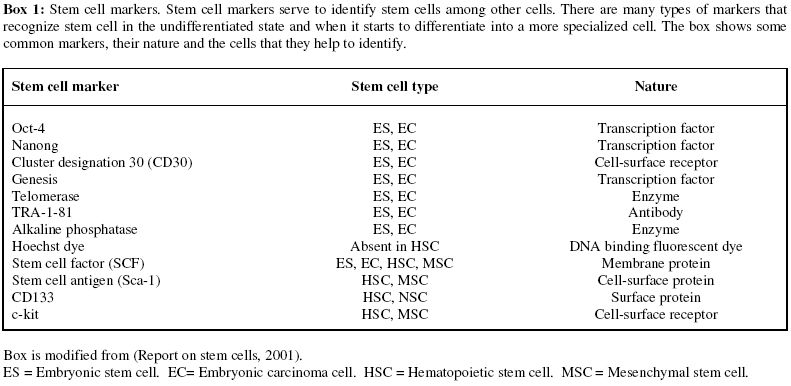
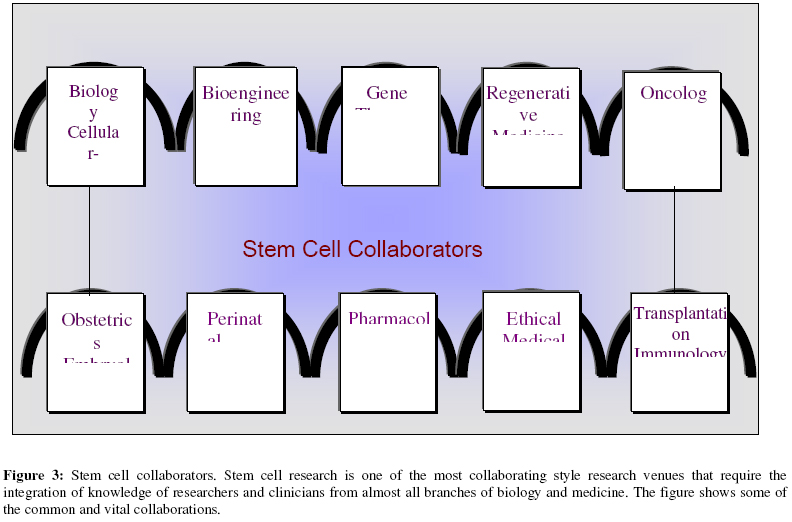
Objective: To explore the potential ways in which stem cell research is linked to research and clinical aspects of Obstetrics and Gynecology practice. Moreover, to explore the possible applications most tailored to the needs and resources of the Middle East. Key words: stem cell, stem cell markers, embryonic stem cells, umbilical cord stem cells, fetal stem cells, trophoblast stem cells, ovarian tumors, endometrial cancer, infertility, endometriosis, perinatal, epigenetic, progenitors. INTRODUCTION History Stem cells were first recognized experimentally in 1945 (1) and the properties of stem cells have been discussed for more than 40 years (2-3). In 1998, James Thomson and his group managed, for the first time, to isolate and culture human embryonic stem cells using blastocysts obtained in excess of in vitro fertilization (4). Over the last decade, stem cells have caught the imagination of both the lay and scientific community with their promise of opening a new frontier in medical therapy. In the following review, we will summarize the basic concepts behind stem cell research and recent developments that may intersect with basic gynecological or obstetrical knowledge or practice. Terminology Stem cells are classically described as undifferentiated cells that retain the capacity for self-renewal and differentiation into specialized cell types. Stem cells can be organized into a hierarchy based on their ability to differentiate (Fig.1). Totipotent stem cells can be obtained as embryonic blastomeres from the fertilized egg up to the 8-cell stage, and can give rise to a complete organism including the extraembryonic tissues. Pluripotent stem cells are those cells that can form the three embryonic tissue layers; the ectoderm, the endoderm and the mesoderm. They can be obtained from the inner cell mass (ICM) of the blastocyst e.g. embryonic stem (ES) cells or from primordial germ cells in the genital ridge, the embryonic germ (EG) cells. Multipotent stem cells can differentiate into more than one type of specialized cell in a certain tissue or organ. These cells can self renew over the life time of the individual or over many subsequent generations if transplanted e.g. hematopoietic stem cells At the bottom of this hierarchy are the precursor or progenitor cells which can only produce terminally differentiated or specialized cells performing closely related functions in a specific organ or tissue (5). Stem cell plasticity: Plasticity is a term referring to the property of being physically malleable. Stem cell plasticity is commonly used to describe the property of being able to switch the fate of the cell into a new phenotype and function (6). Stem cell engraftment: This term indicates the homing of the transfused or transplanted stem cells into a specific target organ and their ability to be functional as evidenced by proliferation, expression of differentiation markers, and formation of specialized proteins or structure. Clonogenicity: The ability of a single stem cell to proliferate and form colonies in vitro. Ex vivo expansion: The use of growth factorbased cultures to increase the number of stem cells or progenitor cells to a level suitable for transfusion or transplantation. Stem cell line: The stem cells that are produced through the division and proliferation of a single stem cell. Stem cell markers: Specific proteins or cellular receptors that allow detection of pluripotency, usually through the use of corresponding tagged antibodies or specific dyes (Fig.2). There are different types of stem cell markers and more markers are being discovered. Each marker or group of markers is specific for a certain type of stem cell. Box 1 shows some common stem cell markers. For example, Oct-4 and Nanog are transcription factors, which are thought to be critical for the self-renewal of pluripotent stem cells in the undifferentiated state. The action of those transcription factors is thought to be through inactivation of differentiation genes in the stem cell. These factors are expressed in human embryonic stem cells as well as in mice and monkey embryonic stem cells (7). Stem Cell Based Sciences There is an apparent or potential interaction of stem cell research with almost every field of biological and clinical research. Therefore, collaboration is a seemingly essential component of stem cell research. Broadly based networking is crucial to attain the best outcome (Fig.3). While, there are various and overlapping stem cell research fields, they can be broadly considered under one of the following subcategories:
Classification of stem cells One of the still developing stem cell sciences is stem cell classification, which is broadened as soon as more stem cell characters and behavior patterns are known, upon which new cells are added or excluded from the "stemness" tagged family. Besides, the discovery of new stem cell markers continually makes the final definition of stem cell under different circumstances unstable. However, by examination of the data so far we outlined different stem cell categories and the key points of comparison in (Table 1). Reyftmann and colleagues reviewed and compared the properties of different stem cell types, including: embryonic stem cells (ES), fetal or embryonic germ cells (EG), fetal somatic cells, umbilical cord stem cells (UCB) and other adult stem cells, regarding their origin, their differentiation potential, and their current therapeutic applications in humans. The authors tried to draw the attention of researchers in the field for the use of fetal stem cells and cord blood cells as a potential alternative to human embryonic stem cells, as they generally encounter less ethical and societal opposition, and they may have equal potential for clinical therapeutics (8). Fetal somatic stem cells can be derived from somatic tissues like the kidney or the liver of 12 weeks age fetus and they are believed to be less immunogenic, more multipotent cells than other adult stem cells. They may also have better engraftment features upon transplantation (9). The embryonic germ cells that can be obtained from the genital crest of the aborted fetus between 8 to 11 weeks age, showed remarkable proliferative potential and have proven to be pluripotent with a normal karyotype. They are more difficult to obtain in the form of undifferentiated cell lines than embryonic stem cells, as they tend to spontaneously differentiate, so more specific culture media should be designed to delay the spontaneous differentiation (10). The establishment of human embryonic germ cell lines can be useful in various fields and may also provide a novel model for the mutagenicity studies of different pharmacological agents (8). Up till now, there are 4 groups who were able to derive human embryonic germ cell lines from the primordial germ cells. Different culture media and growth factors have been used for their isolation and growth. The primordial germ cells may be of importance in the determination of menopause and it has been postulated that their number and hence the genes regulating their proliferation could account for premature ovarian failure. Also, comparative studies of human EG cells and embryonic carcinoma cells offer an informative model on the origin of gonadal tumors (11). A Rich Resource in Obstetrics and Gynecology Obstetricians and gynecologists are usually working in close contact with the main sources of promising stem cell types; embryonic stem cells (ES), umbilical cord blood stem cells (UCB) and fetal stem cells. A number of recent studies reviewed and outlined possible areas in which stem cell research can be applied in fields related to Gynecology and Obstetrics. One of them was the study done by Perillo A, et al., (12) which covered some important combinations:
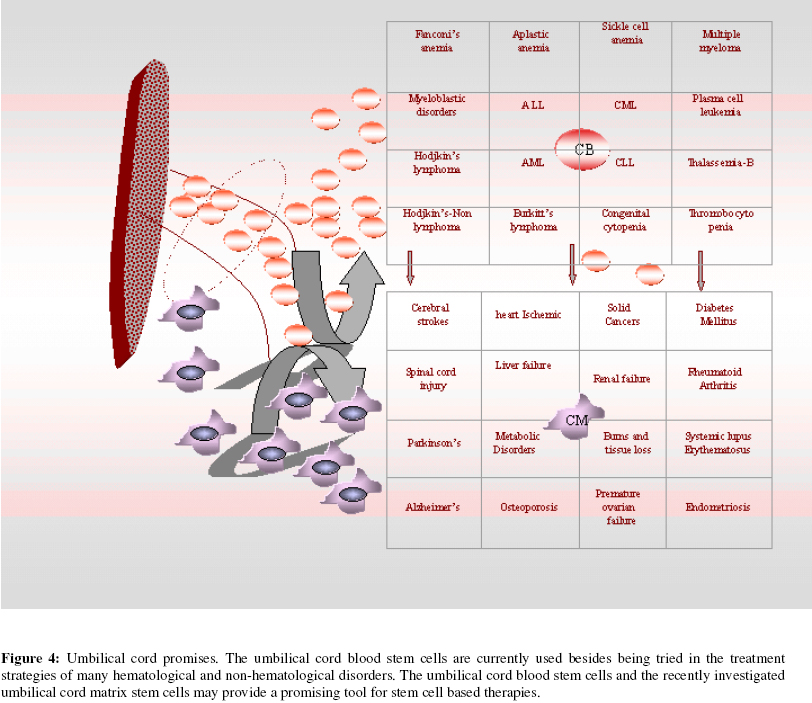
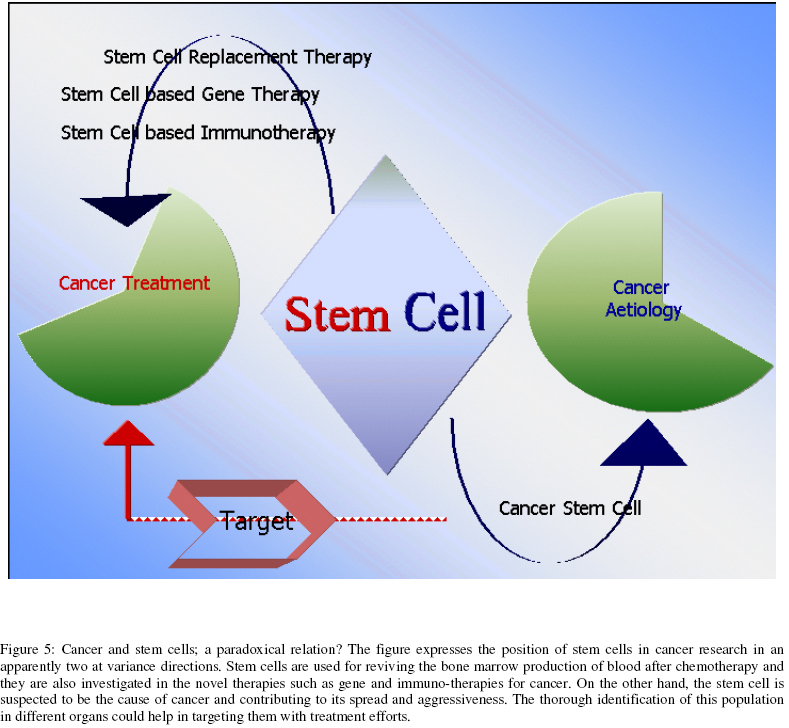
Perinatal medicine is another field, which may be expected to benefit remarkably from stem cell research. In a recent review Santner-Nanan B et al (13) discussed the inherent capacity of stem cells to respond to signals coming from damaged tissue, and their ability to migrate to these tissues and replace the injured cells or to deliver specific growth hormones and protective factors. The potential use of stem cell in gene repair has been investigated and umbilical cord blood stem cells transfected with a viral vector were used to deliver intact genes when transplanted during the perinatal period. The relatively small size of the fetus could enhance the chances of success compared to adults. The regenerative potential of the cord and placental derived stem cells also provide hope in the management of prematurity complications in the newborn such as lung and brain injuries. Stem cells were able to differentiate into bronchial epithelial cells and pneumocytes after in vivo transplantation (13). However, there is still much work to be done to achieve success clinically. Umbilical Cord (UC) stem cells The ethical and public conflicts that surround human embryonic stem cells, has led to research towards finding more non-controversial resources. The umbilical cord and umbilical cord blood, usually designated as waste material in most places of the world, has been proved to contain a clinically valuable source of stem cells. A global annual birth rate of 100 million indicates how large this potential resource can be as a source of stem cells (14). Umbilical cord blood was first transplanted in 1988 in a case of Fanconi’s anemia. Gluckman E et al, 1989(15) and has been used during the past decade increasingly in place of peripheral blood or bone marrow for transplantation. Cord blood can be collected, HLA typed, processed and stored in cord blood banks. Commonly, cord blood stem cells were used for transfusion in stem cell rescue therapy in leukemic children. More recently cord blood has been demonstrated to be a successful alternative to bone marrow in adult leukemia (1618). Some of the diseases, for which umbilical cord blood stem cells are being studied as a potential treatment, are shown in Fig.4. There is a controversy regarding the parameters of sample selection, especially in regard to minimal blood volume that could provide a useful sample for transplantation. Blood volume was found to have a significant impact on the cord blood cellular content after processing and cryopreservation and this was proposed as one method for evaluation of the cost effectiveness for cord blood banking (19). Another more recent study, showed no correlation between the cord blood volume and its content of the nucleated cells (NC) and that automatic processing is superior to manual processing of samples in regard to the number of NC (20). There is also research to show that expansion of cord blood hematopoietic stem cells can be successfully performed in vitro to overcome the hurdles in obtaining a clinically significant number of HSC for therapeutic use. These authors demonstrated the possibility of expanding the longtern SCID repopulating cells in UCB (those cells thought to be responsible for the success of bone marrow engraftment) by 6 to 10-fold. This work could open up the field of adult stem cell transplants using cord blood or increase the possibility of donation to more than one individual. In addition, increased stem cell numbers could make tissue therapeutics with these cells more likely (21). Umbilical cord blood (UCB) hematopoietic stem cells are multipotent and capable of differentiating into non-blood cell types suitable for transplantation (22-23). Di Campli C et al. (24) in a recent controlled experiment tried the direct intraperitoneal infusion of human cord blood stem cells in mice that had an induced hepatic injury using alcohol. By measuring different hepatic markers, they confirmed human cell engraftment and differentiation into hepatocytes, and the mortality rate was significantly reduced from 70% to 20% with evidence of rapid liver engraftment and regeneration (24). In another interesting study, human cord blood cells were transfused to fetal goats that were followed over 2 years. The human cord blood cells engrafted in multiple organs of the animal such as the bone marrow, the liver, the kidney, the spleen, the lung and the heart. Moreover, many human genes were expressed in the tissues of the goat. In the liver, there was evidence of differentiation into more specialized liver cells as the human cells produced tissue specific markers such as the human hepatocyte-specific antigen and other native liver antigens (25). Umbilical cord matrix stem (UCMS) cells; are stem cells derived from human umbilical cord Wharton's Jelly. Weiss ML et al recently managed to characterize UCMS cells and demonstrated their potential as a source of stem cells for therapeutic and transplantation uses. Among those properties, most valuable were their potential to be isolated in large number, their ability to grow efficiently, to form expanding colonies and to be frozen and thawed. They also can be induced to express exogenous proteins, growth factors and angiogenic factors so that they may be valuable in neurodegenerative disorders. In their study, human UCMS cells were transplanted into the brains of hemiparkinsonian non-immune suppressed mice. There was an improvement measured by reduced symptoms in the pilot test. There was no host immune rejection response and no tumors induced when the cells were grafted in normal mice (26). Stem Cells and Gynecologic Tumors Although stem cells have been primarily considered as a potential therapeutic tool for treating malignancy, degenerative diseases and genetic disorders as described above, the role of stem cells in the pathogenesis of malignancy has recently been recognized (Fig.5). Some authors consider this concept as an updated version of older ideas such as the "embryonal rest" theory of cancer, which arose in the 19th century when pathologists noticed the similarity between cancer tissue and embryonic tissue. Thus, it was postulated that cancer might arise from embryoniclike cells. The same concept was supported by pathological observations in tumors such as Wilms tumor, neuroblastoma and teratocarcinoma, which are now considered as examples of tumors arising from cancer stem cells (27). Other authors focused on the comparable morphology and differentiation characters between embryonic carcinoma cells and human embryonic stem cells (28). Furthermore, Andrews et al considered that embryonal carcinoma (EC) cells were the stem cells of teratocarcinoma, and the malignant counterparts of embryonic stem cells. They showed that human ES cells acquire karyotypic changes similar to those expressed by EC cells when cultured long-term in vitro. In addition, when those long-term cultured ES cells were injected into mice, they obtained a teratocarcinoma that histologically contained stem cells, and when the tumor-derived cells were recultured, the cells showed the features of ES cells. Therefore, ES cells may develop in culture similar to EC cells during tumor progression (28). It has been also demonstrated that cancer cell lines derived from various solid malignant tumors have stem cell populations that are capable of selfrenewal and differentiation. Directing treatment towards their differentiation may be of great value in cancer therapy (29). Cancer cells also express embryonic stem cell markers such as Oct-4 and this is considered to be consistent with the stem cell hypothesis of carcinogenesis (30). Consequently, many studies suggested that cancer could arise from a cancer stem cell, a tumor-initiating cell that has properties similar to those of stem cells such as the ability to be maintained indefinitely in culture. It is thought that these cancer stem cells are crucial for the malignant behavior (31). Moreover, some studies supported the principle of similar molecular mechanisms controlling both the metastasis of cancer stem cells and the trafficking of normal stem cells and discussed the common molecular mechanisms involved in these processes. As a result, strategies aimed at modifying those factors could have important clinical implications in oncology (32). Most recently, one of the interesting models that have been proposed for cancer etiology is the epigenetic progenitor model. This model postulates that tumorigenesis is primarily initiated by epigenetic changes in the normal stem cell population of a specific tissue or organ. Chronic injury following nutritional, inflammatory, and environmental factors of diverse sources might be the cause of this epigenetic change resulting in enhanced stemness and pluripotency. More specifically, the epigenetic changes would be possibly carcinogenic if they affected one or more of the tumor progenitor genes in the stem cell. This model relies on currently accepted evidence of epigenetic changes such as DNA hypomethylation, hypermethyaltion and chromatin changes, all of which are linked to the development of different cancers and could account for certain characteristics of cancer such as late onset development, heterogeneity, resistance to therapy and cancer progression. The development of new cancer prevention techniques and therapies might hinge on the prevention or reversal of the initial progenitor epigenetic changes (33). At the clinical level, cancer stem cells have now been identified in several malignancies, including those of blood, brain, breast, and skin. Kondo T et al showed the presence of a sub-population of multipotent stem cells in glioma that were able to differentiate and also to be tumorigenic in animal models (34). Another group isolated stem-like neural precursors from human glioblastoma (35). Ponti D et al reported the isolation of breast cancer–initiating cells from three breast cancer lesions and from an established breast carcinoma cell line. Those cultures contained undifferentiated cells capable of self-renewal and proliferation as non-adherent spherical clusters after cloning. In addition, they were able to differentiate into mammary epithelial lines such as ductal and myoepithelial cells. The stem cells were also identified by their expression of the specific stem cell tag, Oct-4, and gave rise to new tumors when they were grafted into mice (36). Fang D et al tested the presence of a tumorigenic stem cell–like population in melanomas and found a subpopulation of stem cells that when cultured in specific medium used for human embryonic stem cells, proliferated as non-adherent spheres. After cloning of these melanoma cells, they maintained stem cell characteristics and were able to self-renew and differentiate into melanogenic, adipogenic, chondrogenic, and osteogenic lineages. Also they found that this subpopulation was more tumorigenic than other cells when injected into mice (37). Ovarian cancer Bapat SA, et al (38) isolated 2 tumorigenic clones from the ascitic fluid of a patient with an advanced grade IV adenocarcinoma of the ovary. The clones were characterized as non-adherent spheroids capable of self-renewal in vitro, as well as being able of inducing tumors in mice similar to the original human tumor in histopathology. The cells maintained their ovarian cancer character upon serial grafting in an animal model. The clones expressed specific stem cell markers such as Nanog and Oct4. Therefore, the authors concluded that epithelial ovarian stem cell mutagenesis could be a cause of epithelial ovarian tumors and of the aggressiveness and recurrence of ovarian cancer (38). Endometrial Cancer Chan RW et al hypothesized that adult stem cells reside in the endometrium. They showed for the first time, that the human endometrium contains a small population of epithelial cells and stromal cells that exhibit stem cell behavior in vitro. They measured a functional stem-cell trait, clonogenicity, to identify the stem cells among other differentiated cells. This research study explored the role of stem cells in proliferative endometrial diseases including endometriosis, endometrial hyperplasia and endometrial cancer (39). Gynecologic tumors-stem cells; case reports Hashiguchi J described a rare case of uterine lipoleiomyomata with intravascular leiomyoma in a 48-year-old female, which developed in the uterine body. The lipoleiomyomata showed the proliferation of leiomyocytes mixed with adipocytes. Intravascular leiomyoma was separately present in the broad ligament. Immunohistochemical studies revealed that this intravascular leiomyoma was positive for S-100 alpha protein, Neuron-specific enolase (NSE), factor VIII-related antigen, and a monoclonal antibody to muscle cell actin isotypes termed (HHF35). As a result of these observations the authors hypothesized that this leiomyomatous tumor may have arisen from multipotent undifferentiated mesenchymal stem cells (40). Scurry J, et al reported a case of a Merkel cell tumor of the vulva with glandular and squamous differentiation which supported an origin from pluripotent stem cells. Though this was the ninth reported case of a vulvar Merkel cell tumor, it was the first where squamous and glandular differentiations were both seen (41). Mukonoweshuro and Oriowolo reported a case of a 66-year-old patient with stromal osseous metaplasia in a low-grade ovarian adenocarcinoma. The patient had a past history of stage 1c welldifferentiated endometrioid adenocarcinoma removed 21 years ago and was treated with radiotherapy. The recurrent tumor had a prominent stromal osseous metaplasia that had not been present in the initial tumor and likely involved multipotential stromal stem cells leading to bone formation (42). Ambani DS et al described the first reported case of a monophasic synovial sarcoma presenting as a vulvar mass in a 33-year-old-pateint. The sarcoma was thought to develop from pluripotent stem cells that capable of differentiating into mesenchymal and epithelial structures (43). To conclude, it is apparent that isolation and long-term cultures of ovarian, endometrial and cervical tumorigenic cells with progenitor cell properties represent a suitable in vitro model to explore the characters of cancer–initiating cells, to understand their possible role in recurrence after treatment and to develop therapies aimed at eradicating the tumorigenic subpopulation within those malignancies. Stem Cells in the Treatment of Gynecologic Tumors Hematopoietic stem cells (HSC) represent well-established rescue treatment for solid tumors including gynecological cancers. High-dose chemotherapy regimens followed by autologous HSC transplantation have been used for several years in the treatment of advanced ovarian cancer. Adjunctive treatment with different growth factors and enhancers has also been used for rapid restoration of immune system function (12). Another possibility for using stem cells in the treatment of gynecologic tumors is their potential as cellular vehicles for viral vectors and therapeutics (6). These cells could solve some of the problems of non specific delivery of vectors, since they had been shown to have highly specific engraftment properties in some tissues such as the brain. Moore and colleagues injected human umbilical cord progenitor endothelial cells into glioma model in mice. The cells specifically were attracted to the brain tumor tissue suggesting that HSC can be a promising carrier for gene therapies in brain tumors (44). Stem Cells and Reproductive Biology Stem cell research is currently thought to be capable of establishing solutions for many ovarian and testicular disorders and contributing to the treatment of infertility, based on the capacity of stem cells to provide model systems to help understanding the differentiation of, and functioning of, the gonads (45). Johnson J et al (46) presented the concept of an extra-gonadal source of germ cells from the bone marrow that could give rise to oocytes during adult life. Their conclusion were based on several observations including the capacity of adult mouse ovaries to generate a larger number of oocytes compared to the small pre-meiotic primordial germ cell pool they contain. In addition, they demonstrated the presence of germ cell markers in the bone marrow, and referred to some experimental findings such as the restoration of ovarian oocyte production in mice after post-chemotherapy bone marrow transplantation. Some of those oocytes were identified as donor-derived (46). The same effect occurred after bone marrow transplantation in ataxia telangiectasia-mutated gene-deficient mice, which acquired the ability to a produce oocytes that they were lacking before. The authors determined that the oocytes appeared to have normal morphology and expression of specific oocyte markers (46). However, more research on the fertilization capacity of these extragonadal-derived oocytes needs to be done and it is too early to determine if these findings will have clinical relevance to postponing or treating premature ovarian failure. The above study, has been criticized in a review by Bukovsky A, (47, 48) who suggested that ovarian surface epithelium germ cells have been shown to regularly shed primordial oocyte-like structures through the blood stream to distant sites in the body during the process of follicular renewal, and the bone marrow might be one of those sites. Earlier results from Johnson J et al also a demonstrated that evidence of germ cell formation in bone marrow completely disappeared in the absence of ovaries. In spite of this, Bukovsky still believes that the autologous transfusions can be helpful in cases such as cancer chemotherapy in young females who posses ovaries with a capacity for follicular renewal. A more promising approach worth further exploration is the in vitro production of new autologous oocytes from the ovarian surface epithelium and their in vitro fertilization, and intrauterine implantation of genetically related embryos (47, 48). In a search for a stem cell-related etiology for endometriosis, Starzinski-Powitz et al demonstrated the presence of undifferentiated endometrial cell populations, with multiple epithelial markers of differentiation, and with the capacity of self-renewal and plasticity. These endometrial stem cells have been isolated from retrograde menstrual blood, and they have also been isolated from peritoneal and colonic endometriotic lesions. These cells suggest that retrograde menstrual blood stem cells may be the etiological factor of both the primary disease and its progression to distant sites (49). The basal layer of the endometrium has been suggested as the origin of these stem cells (50). Trophoblast Stem Cells and Placental Development The trophoblast is an integral and crucial part of the developing embryo. Having a model for studying normal placental development and circulation (51) will certainly enhance the examination of abnormal placental development including such conditions as gestational trophoblastic diseases, intrauterine growth restriction and pre-eclampsia. The establishment of trophoblast stem cell lines is one tool to study trophoblast proliferation and differentiation. The isolation of trophoblast stem cell lines from blastocysts in the mouse has been successful in the presence of specific growth factors (52-53). However, the mouse trophoblast is significantly different from human trophoblast, and obtaining trophoblast cell lines from human embryonic stem cells has so far been unsuccessful. As a result, there is still no accurate model applicable to the human trophoblast and placenta (54). A recent report of successful derivation of human trophoblast stem cell lines from human embryonic stem cells, if confirmed, could generate a template for models of human implantation and normal and abnormal placental development (55). This model could also help in resolving some important molecular mechanisms that control the trophoblast invasion through the endometrium during implantation in contrast to the uncontrolled invasion of tumors (56). Defective trophoblast stem cell invasion of the endometrium and incomplete differentiation of those cells have also been linked to the pathogenesis of pre-eclampsia (57). These issues could be related to the levels and activity of endothelial or trophoblast progenitor cells (58). Possible Future Research Stem Cells and the Pathogenesis of Gynecologic Tumors
Stem Cells and Reproductive Biology
Umbilical Cord
Trophoblast Stem Cells and Placental Development
Prospects for stem cells in the Middle East As the ethical debate is the top priority both at the political and social levels, we should seriously consider our position towards this emerging research direction from a middle east cultural perspective. Indeed, there are a few recent, valuable literature references to the position of Islam on stem cell research. Aksoy S has outlined the bases of Islamic law derived form the Quran and “sunnah” on which rulings concerning stem cell research could be judged by most scholars (59). The majority of Islamic scholars see the use of the embryo for essential therapeutic or research purposes as being permissible if necessary on the strict condition that this process does not contradict any genuine Islamic moral rule. They emphasize that this research should always be limited to the time before ensoulment and should be restricted to the use of the extra embryos left behind by the IVF technique. It is not acceptable to deliberately produce embryos for the research purposes. In addition, seeking non-controversial sources of stem cells is most encouraged (60-61). In a recent review, Hug K. analyzed the broad spectrum of ethical arguments against embryonic stem cell research and the counter opinion for each position. The author also presented the point of view of the major world religions including the three monotheistic faiths Islam, Christianity and Judaism. The position of most orthodox and conservative Christian churches was to prohibit the use of embryos for stem cell research except for those embryonic stem cell lines that have been already established, based on their belief that human life starts at the time of conception. Unlike Christianity, Judaism permits embryonic stem cell research if the embryos are obtained within the first 40 days after conception, which is considered as not being full human status (62). Another factor in the Middle East regarding stem cell research is its cost-effectiveness. Do we have the resources to establish such a program? The basic structure of stem cell research should start with building multidisciplinary programs and establishing collaborations between stem cell research partners including basic sciences, clinical sciences and engineering. In addition, the group effort should seek to link major scientific institutes in the region and promote the concept among related industrial and pharmacological institutions that could contribute substantially to funding and to reducing the costs of therapeutics. A major part of the funding should be directed to building umbilical cord and placental tissues banks and for providing equipment and training programs for researchers, clinicians and technicians. Moreover, the most cost-effective techniques for cell collection, purification and expansion should be analyzed before starting the practical steps. A very encouraging issue is the huge resource of deliveries. For example the birth rate of 25.8 per 1000 population in 2004 in Egypt, and similar rates in most countries of the region, is almost double the rate in western countries (63). This illustrates how large a resource we have in the Middle East for promising sources of stem cells including umbilical cord blood and matrix, and trophoblast and fetal somatic stem cells. These are the stem cell sources that are probably the most applicable for research purposes in our societies. Some countries, such as Iran and Turkey (60, 64) have already started to pursue this research path. However; much more effort is needed by the scientific community in the Middle East to establish an economically viable research program in stem cell research. CONCLUSION A wide range of research efforts is currently underway to explore stem cell solutions for many different clinical problems. Clinicians and researchers in Obstetrics and Gynecology should be at the forefront of stem cell research because of our access to the most important raw materials in this area. Current IVF surplus embryos following infertility treatment are the major resource for embryonic stem cells within the proper ethical framework. Delivery products such as umbilical cord blood, mesenchymal stem cells derived from umbilical cord matrix or trophoblast stem cells from placental tissue are all sources of potential new treatments that avoid the ethical and religious problems associated with embryo use. At the top of the list of diseases needing new therapies are cancer, degenerative diseases, autoimmune diseases, congenital and acquired immuno-deficiencies and massive tissue loss from different sorts of pathological and physical injuries. Focal interest in the field of gynecology involves stem cells in relation to the pathogenesis of ovarian, endometrial and other cancers. Established stem cell replacement therapy is already being used in the process of blood regeneration after cancer chemotherapy. Infertility might also benefit from the research insights in the role of stem cells to develop autologous oocytes. Human implantation and placentation are areas that might benefit from trophoblast stem cell derivation and study. Perinatal brain and lung injuries, as well as congenital immuno-deficiencies and metabolic dystrophies, are also potential targets for successful stem cell therapies. Although stem cell research is still in its infancy in the Middle East, our potential wealth of clinical material and our willingness to address the proper ethical, religious and cultural issues related to stem cell research could result in a leadership role in the clinical use of stem cells. REFERENCES
Copyright © Middle East Fertility Society The following images related to this document are available:Photo images[mf06028f5.jpg] [mf06028b1.jpg] [mf06028f2.jpg] [mf06028t1.jpg] [mf06028f3.jpg] [mf06028f1.jpg] [mf06028f4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}