 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Middle East Fertility Society Journal, Vol. 11, No. 3, 2006, pp. 191-195 The effect of zona thinning size on implantation and pregnancy rates of ICSI-ET patients with advanced woman age Erdal Aktan, M.D. * Dilek Ozer, M.D. * Aygul Demirol, M.D.† Timur Gurgan, M.D.‡ Kaan Bozkurt, M.D. * Ozel Ege Tup Bebek Merkezi, IVF Center, Izmir; Clinic Women Health, Infertility and IVF Center, Ankara, and Hacettepe University, Faculty of Medicine, Dept of Ob&Gyn, Reproductive Endocrinology and IVF Unit, Ankara, Turkey *Ozel Ege Tup Bebek Merkezi, IVF Center, Izmir, Turkey Received on January 20, 2006; Code Number: mf06032 ABSTRACT
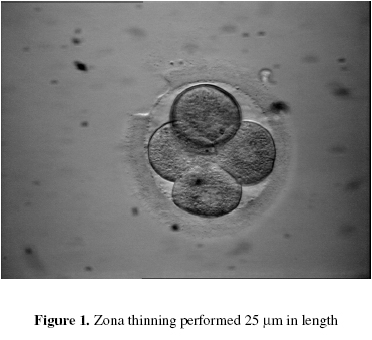
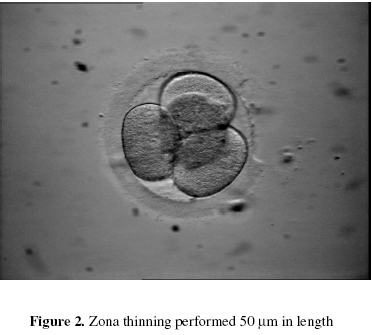
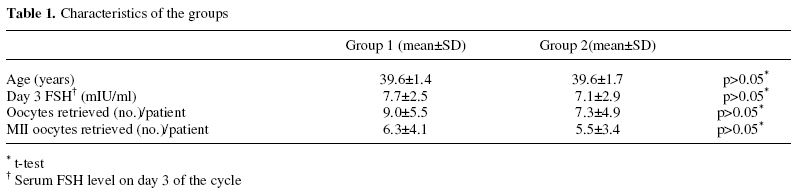
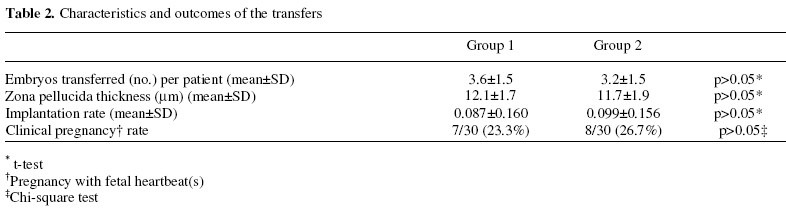
Objective: To find if the zona thinning size (in length) of the embryos transferred had any effects on the implantation and clinical pregnancy rates. Key words: Clinical pregnancy rate, implantation rate, hatching, zona thinning size, ICSI. Implantation rate is the limiting factor for the success of IVF-ET. Both the embryonic capabilities and the degree of uterine receptivity affect implantation, and the hatching of the embryo is the key event (1). Increased zona thickness (2) and reduction of enzymatic lysins produced by the embryo itself (3- 5) were proposed as the possible causes of unsuccessful hatching and reduced implantation rates. Furthermore, the phenomenon of zona hardening and failure of hatching may be worse in patients of advanced age, which may contribute to lower pregnancy rates(3,6,7). Assisted hatching procedures using mechanical methods (1,8), chemical methods (9,10), piezo-micromanipulator (11) or laser systems (12-14) to overcome these difficulties and improve the hatching potential of blastocysts have been proposed. Improvements in laser technology led the novel Zona Laser Treatment Systems achieve a great accuracy and safety which put mechanical and chemical hatching methods into the shade. It has been reported that assisted hatching improved implantation and pregnancy rates in patients with poor prognosis of pregnancy and repeated IVF failures (13,14). Laser technology was used for zona thinning of embryos by ablating 50% of the thickness of zona in a length of approximately 20 µm, and it was also reported that this new approach improved the implantation and pregnancy rates (14). Considering the data regarding the effects of assisted hatching on the outcome of IVF patients, we decided to investigate if increasing the hatching size (in length) of the embryos transferred would improve the implantation and pregnancy rates in women with advanced age. MATERIALS AND METHODS Patients Sixty women undergoing ICSI-ET treatment, who were ≥38 years old and accepted to take part in this prospective-randomized study, were enrolled. Women were assigned as one to the 25 µm (Group 1) and the following to the 50 µm (Group 2) zona thinning size groups consecutively, according to the order of the transfers. Thirty patients were assigned to each of the groups. Stimulation protocol Gonadotrophin-releasing hormone agonist (GnRH-a) (leuprolide acetate 0.5 mg/day s.c) injections in long or short protocol were started in all patients and continued until the day of human chorionic gonadotrophin (HCG) injection. Routine ovarian stimulation with human menopausal gonadotrophins (HMG)/ rec-FSH was started on the 3rd day of the cycle and ovarian response was monitored using vaginal ultrasound scan and serial estradiol concentrations. HCG (10 000 IU i.m.) was administered 36 h before the oocyte retrieval. Luteal phase was supported with progesterone 600 mg/ day, vaginally. Oocyte handling, ICSI procedure The oocytes were denuded of their surrounding cumulus cells 2 h after retrieval using hyaluronidase 80 mIU/ml for 10-15 s. Then, the oocytes were transferred into Gamete medium and repeated aspiration in a finely pulled pipette was performed for the complete removal of the corona cells. The oocytes were rinsed and incubated in IVF medium under mineral oil until the time of injection. ICSI was performed in all metaphase-II (MII) oocytes using micromanipulators (Eppendorf TransferMan NK/CellTram air-CellTram oil, Hamburg, Germany) mounted on an inverted microscope (Olympus IX 70, Tokyo, Japan) with a Hoffmann Modulation Contrast System (Modulation Optics, Greenvale, NY, USA). Zona thinning procedure and embryo transfer Embryos were graded according to the following criteria: Grade 1: Embryos with evenly sized blastomeres and no fragmentation, Grade 2: Embryos with uneven or irregularly shaped blastomeres, no more than 10% fragmentation, Grade 3: Embryos with between 10 and 50% fragmentation, Grade 4: Embryos with fragmentation greater than 50%. At least one Grade 1-3 embryo, with 4 or 7/8 blastomeres on the 2nd or 3rd day respectively, was transferred for each patient. Laser-assisted hatching procedure was carried out on all of the embryos selected for transfers using Hamilton Thorne Zona Laser Treatment System (ZLTS, Beverly, MA, USA). Zona pellucida thickness of an embryo was determined by calculating the mean of four measurements of zona pellucida thickness performed on that embryo. A trench breaching nearly the whole thickness but not perforating the zona was made on each of the embryos selected for transfers 30 minutes before the embryo transfer, in the length of 25 (Figure 1) or 50 µm (Figure 2) according to the groups the patients were assigned. The cleaved embryo was positioned and held firmly using an ICSI holding pipette such that the point at which laser was applied had the largest available perivitelline space of the embryo. A single opening was drilled using laser pulse length of 25 ms. If the zona was resistant to laser pulses of 25 ms and no perforation occurs, a laser pulse of larger length such as 125 ms was used. If the zona was still resistant to perforation with laser pulses of 125 ms, then lasers of 750 ms pulse length was applied. Embryo transfers were performed under the guidance of ultrasound scanning. In our clinic, our policy is to perform laser zona thinning procedure on the embryos selected for transfer in “all” of the women ≥ 38 years old and undergoing IVF/ICSI treatment. This study was approved by the institutional ethics committee. Statistical analysis The results of the groups were compared using t-test and chi-square test. RESULTS The characteristics of the groups are summarized in Table 1. The groups are similar regarding the age of the patients, Day 3 FSH levels, and the number of the oocytes retrieved. The characteristics of the transfers are shown in Table 2. The groups revealed similar implantation and clinical pregnancy rates with the similar number of embryos transferred. DISCUSSION Assisting the hatching of embryos before transfer can be expected to improve implantation and pregnancy rates (15). It has been hypothesized that assisted hatching may enhance embryo implantation, not only by mechanically facilitating the hatching process, but by also permitting early embryo endometrium contact (16). Different techniques were proposed for assisted hatching. Balaban et al (17) reported that selective assisted hatching using four different methods (partial zona dissection, acid Tyrode, diode laser, and pronase thinning of zona) yielded similar implantation and pregnancy rates. Hsieh et al (18) also compared the chemical and laser assisted hatching methods and found that laser assisted hatching of embryos was better than the chemical method for enhancing the pregnancy rate in women with advanced age. Routine laser assisted hatching of embryos also enhances the pregnancy rate in women with young age (19). In contrast, it was reported that laser assisted hatching did not improve the implantation rate of frozen-thawed embryo transfer (20, 21). A novel approach as only thinning the zona of embryos but not perforating it has some advantages over the traditional assisted hatching procedure, which encompasses the whole thickness of the zona. The holes on the zona of embryo created by drilling release the pressure exerted by the growing embryo, and the natural expansion of the blastocyst and the thinning of the zona do not occur, and the zona remains relatively thick. This may be the cause of higher failure of pregnancy following drilling (22). Also, the loss of blastomeres or whole embryo may be encountered during the contractions of reproductive tract (23). Considering these drawbacks Gordon and Dapunt (24, 25) applied the zona thinning procedure in mouse embryos and found a large increase in implantation rates comparing with the untreated embryos. In 1992 Khalifa et al (9) also reported that complete hatching was not the rule after zona drilling while thinning of zona promoted early and complete hatching of the embryos. Antinori et al (14) concluded that the significant increase in the implantation rates obtained in their laser treated embryo group could be explained by including the inner layer of zona pellucida in the thinning procedure. They stated that 50% reduction in zona thickness makes it very likely that the inner layer of zona pellucida is involved in the thinning procedure of the bilayered zona of human embryo. Improvements in the laser technology made it possible to precisely control the amount of zona thinning procedure by offering accurate targeting and shooting capabilities. Mantoudis et al (16) evaluated the efficacy of laser assisted hatching of embryos on implantation and pregnancy rates of a selected group of infertility patients. They compared the pregnancy rates in total, partial, and quarter laser assisted hatching groups and found that pregnancy and clinical pregnancy rates arising from quarter laser assisted hatching were higher in comparison with partial and total laser assisted hatching. In another study, it was reported that quarter laser assisted hatching was an effective strategy for improving the implantation of embryos in patients with repeated implantation failures (26). In this study, we compared the “25 and 50 µm” zona thinning size groups in women with advanced age and found no statistically significant difference between the groups regarding the implantation and clinical pregnancy rates. In conclusion, the results of this study indicated that increasing the zona thinning length up to twice the commonly used size did not have any significant effects on the implantation and clinical pregnancy rates in women with advanced age who underwent ICSI-ET treatment. REFERENCES
Copyright © Middle East Fertility Society The following images related to this document are available:Photo images[mf06032f1.jpg] [mf06032t2.jpg] [mf06032t1.jpg] [mf06032f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}