 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Middle East Fertility Society Journal, Vol. 11, No. 3, 2006, pp. 202-209 Insulin resistance and upper-body obesity in polycystic ovary syndrome Ansam A. Al-Bayatti, M.B.Ch.B., M.Sc., Ph.D. Department of Biochemistry, College of Medicine, University of Baghdad, Iraq Correspondence: Assist. Prof. Dr. Ansam Al-Bayatti Ph.D., College of medicine, University of Baghdad, Bab Al-Muatham Baghdad, Iraq, P.O. Box: 61032, Phone: +96417722065, Mobile: +9647901331923, E-Mail: ansimalaad@yahoo.com Received on March 6, 2006; revised and accepted on May 31, 2006 Code Number: mf06034 ABSTRACT
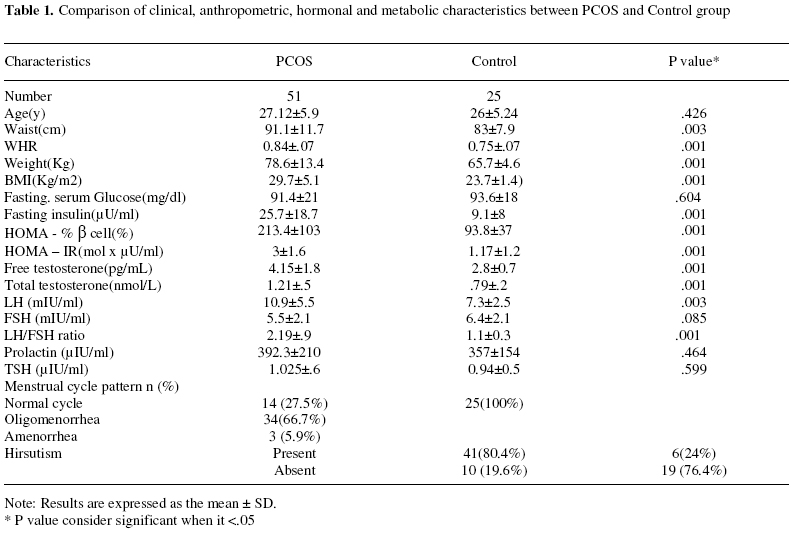
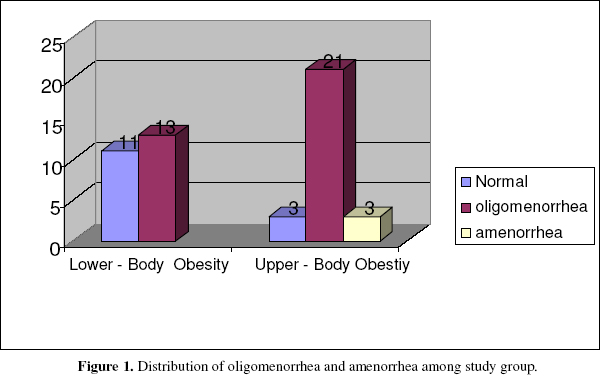
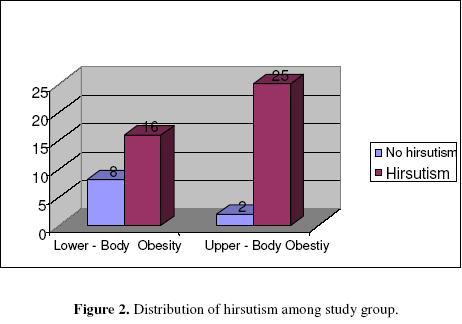
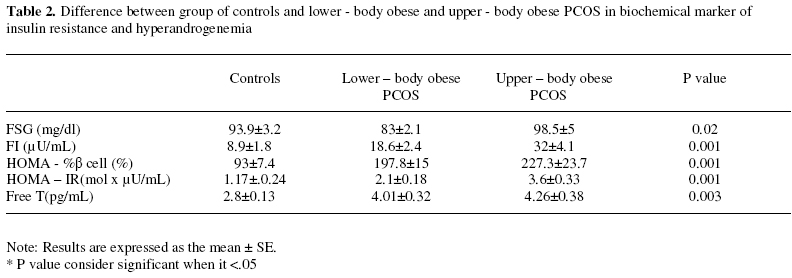
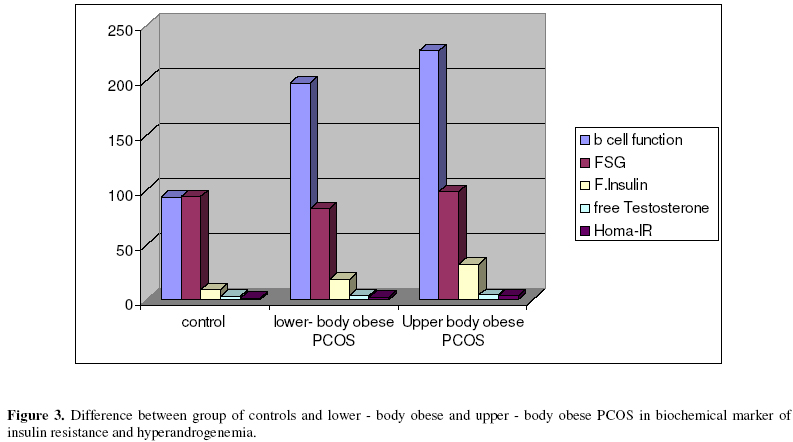
Background: Polycystic ovary syndrome (PCOS) is the most common endocrinopathy affecting 5-10% of premenopausal women. 50-90% characterized by insulin resistance. Obesity is common among patient with PCOS. Key words: polycystic ovary syndrome, insulin resistance, upper -body obesity. Polycystic ovary syndrome (PCOS) is the most common form of anovulatory infertility found in women of reproductive age. PCOS is estimated to occur in 5 – 10 % of reproductive age women (1). The disorder is characterized by hyperandrogenemia, chronic anovulation, and reduced fertility (2). PCOS patients are also at increased risk for obesity, insulin resistance, type2 diabetes, and premature arteriosclerosis. Consequently, PCOS has significant implications for the health and quality of life of these patients. This true even later in life when reproductive disturbances become less pronounced (3, 4). Insulin resistance, defined as subnormal insulin action on glucose, representing a unifying pathogenic link in a cluster of abnormalities grouped under the term of insulin resistance syndrome (5). More recently, investigators recognized insulin resistance, which characterizes 50 -90 % of PCOS women, as central components of PCOS, possibly playing an underlying pathogenic role. Women with PCOS also show an increase prevalence of abnormal β-cells function (6, 7). Insulin resistance is found in most overweight women with PCOS to greater extent than can be expected from obesity. The gold standard method for quantifying insulin sensitivity had been the hyperinsulinemic euglycemic clamp technique. However, this technique is expensive, labor intensive, uncomfortable for patient and time consuming (3). Many investigators have studied simple surrogate indices of insulin resistance in comparison with the index assessed by euglycemic hyperinsulinemic clamp. One of these is Homeostasis model assessment (HOMA) of insulin resistance (HOMA – IR) which provide a mathematical mean for estimating insulin resistance. The rationale for using this calculation is that the relationship between glucose and insulin reflecting insulin sensitivity are hyperbolic rather than linear and it shows a very good correlation with clamp method (8). Obesity is an excessive accumulation of fat in the body. The prevalence of obesity is steady increasing across the world particularly in the developed countries. Obesity is one of feature of original description of syndrome by Stein and Leventhal, is seen in 35 – 60% of women with PCOS (2). Upper – body obesity (android obesity) is common adverse health factor. There is overwhelming evidence that Upper – body obesity is major risk factor for cardiovascular disease and type 2 Diabetes Mellitus, whereas lower body obesity is not. Upper – body obesity diagnosed by measurement of waist – hip ratio (WHR), waist circumference, CT scan and MRI imaging (9). The aim of this study is investigate the relationship between insulin resistance and β cell function in upper – body obese women with PCOS. Compared it with those of lower – body obesity and controls. MATERIALS AND METHODS Patients Fifty one Iraqi women with PCOS in their reproductive age (20 – 40) old, were recruited between March 2005 and August 2005 from Infertility Clinic population of Al-Elwiyha maternity teaching hospital. None had used medication including oral contraceptive pills or metformin for at least 3 months preceding the study. Patients were excluded if they were diabetics. After undergoing a history and physical examination including measurement of height, weight, waist and hip circumference, BMI (weight [kg] divided by height square [m2]) were calculated. Blood sampling were performed at 8:00 – 10:00 am, during 3rd – 6th day of menstrual cycle (only follicular phase) for those with normal cycle. For patient with oligomenorrhea (< 8 cycle / year) blood samples were collected regardless the duration of the cycle. Blood samples were collected into plain tube and centrifuged within 30 min of collection. Serum was removed. serum glucose was measured using enzymatic colorimetric method, the rest of the serum stored at -18ºC until time of assay for determination of total testosterone, free testosterone, insulin, LH, FSH, Prolactin, TSH. The presence of PCOS was defined by revised 2003 criteria arising from European Society of Human Reproduction and Embryology (ESHRE) and American Society for Reproductive Medicine (ASRM) symposium held at 1 may 2003 Rotterdam, Netherlands in which PCOS is diagnosed if there are any two of the following: 1) menstrual dysfunction 2) clinical or biochemical hyperandrogenism 3) presence of polycystic ovaries on ultrasound examination. With the exclusion of other etiologies of hyperandrogenism (late onset congenital adrenal hyperplasia, androgen – secreting tumor, Cushing syndrome, hyperprolactinemia and hypothyroidism) (10). Controls Twenty five apparently healthy fertile women who where attending our hospital as companions had served as controls who were matched for age and with regular menstrual cycle and normal ultrasound and no hyperandrogenism features. Assays The serum glucose assay was performed with enzymatic colorimetric method (GOD – POD) supplies by Giesse Diagnostic Snc. Italy. Serum insulin, free testosterone and total testosterone were measured by ELISA (Diagnostic Automation Inc. Canada). Serum LH, FSH, Prolactin, TSH measured by IRMA Institute of Isotope Ltd. Budapest. Hungary. Statistical analyses Homeostasis model assessment (HOMA) was used to calculate indices of insulin resistance and insulin secretion for each of patient and control (11). HOMA–IR = [(glucose in mg/dl x 0.05) x insulin µU/ml]/22.5, HOMA -% β cell= [20 x insulin µU/ml]/[(glucose in mg/dl x 0.05)–35]. In ideal normal – weight individual age <35 year had HOMA – IR of 1 mol x µU/ L2 and HOMA -% β cell function of 100%. The computer based HOMA2 calculator (available at www.dtu.ox.ac.uk/homa) uses fasting glucose and insulin to generate the index of insulin resistance, HOMA – IR, and the index of β cell function (HOMA - %B). Student t-test was used to compare means between PCOS and control. Analysis of variance (ANOVA) was used for the evaluation of the difference between controls, lower – body obese PCOS, upper – body obese PCOS patients. The association of variables was established with Pearson coefficient of Correlation. A P value of < 0.05 was considered statistically significant. All data were analyzed with SPSS software (statistical Package for the Social Sciences, version 11.0 for windows XP; SPSS, Inc, Chicago, I11). RESULTS The clinical, anthropometric, hormonal, and metabolic variable in the 51 patients with PCOS and 25 control groups were shown in table (1). There is no significant difference with regard to age, fasting serum glucose, FSH, Prolactin, TSH (p value>0.05). Waist circumference, WHR, BMI, the mean serum level of LH, free testosterone, total testosterone were significantly elevated in PCOS patient compare with control group. (p value < 0.05). Mathematical models for assessment of insulin resistance (HOMA – IR) and percent of β cells function where also significantly high in patients with PCOS compared with control. Form the total 51 patients with PCOS enrolled in the study 34 patients (66.7%) had oligomenorrhea of which 21 patients (61.8%) had got upper - body obesity. Also 41 patients (80.4%) had hirsutism from which 25 (49%) had upper -body obesity (Figure 1, 2). With regard to WHR, PCOS patients had divided into two group using value of WHR of 0.85 as cutoff: into upper – body obesity (WHR>0.85) and lower body obesity (WHR ≤ 0.85). We found among obese PCOS (BMI >25) 26 patients (60%) had upper – body obesity in compare to only 2 (28%) of obese control. Using the analysis of variance (ANOVA) comparing two groups of patients with PCOS (upper – body obesity, lower – body obesity) with those controls. It had been found that. (Table 2, Figure 3). Patient with upper–body obesity are significantly more insulin resistance and have high percentage of β cells function than those with lower body obesity which in turn more insulin resistance than control. There is also significant positive correlation between upper body obesity and insulin resistance (HOMA –IR) with (r=0.371, p=0.002), β cell function (HOMA -% β cell) with (r=0.383, p=0.001) and serum free testosterone (r=0.254, p=0.027) fasting insulin (r=0.387, p=0.001). The highest blood glucose level was found significantly in patient with PCOS with upper – body obesity in compare to those with lower body obesity or control. We use the upper 95th percentile to establish a normal limit for HOMA–IR. It is found that 95th percentile for control where 1.9 mol x μU/L2 using this cutoff value for determination of insulin resistance. We found that around 74.5% of our patients have insulin resistance. DISCUSSION As mentioned above, polycystic ovary syndrome is heterogeneous clinical disorder. Hyperinsulinemia and insulin resistance and hyperandrogenemia are often described in women with PCOS. Obesity, particularly upper – body obesity, may play a pathogenic role in development of the syndrome in susceptible individuals (11, 12). As shown in the result 34% of POCS had oligomenorrhea from which 21 patients (61.8%) had upper -body obesity. These data were in consistence with Kaye et al. (1990) who found that high WHR were associated with more menstrual abnormality and high prevalence of infertility (13). Hollmann et al. (1997) showed that high WHR was associated with greater disturbance in reproductive hormones in PCOS (14). The most common symptom in young women with PCOS is excessive facial hair (hirsutism). In our study, we found high percentage of hirsutism among patients with PCOS (80.4%) in compared to only (24%) of the control, and this in agreement with the other study which found to be 83% in PCOS (15). From PCOS with hirsutism was found that 25 (61%) had upper – body obesity and this confirmed by Evans et al. (1988) who found that high WHR significantly greater in hirsute subject (16). We used HOMA-IR to quantify insulin resistance because this tool has been shown to be reliable reflection of insulin resistance with a good correlation (r= 0.6 – 0.88) with euglycemic hyperinsulinemic glucose clamp study. A recent report showed HOMA – IR to have a better correlation with clamp results than even indices derived from oral glucose tolerance tests (17). By using the upper 95th percentile as cutoff value for insulin resistance (1.9 mol x µU/l2). This study found 76.5 % of our population with PCOS had insulin resistance. These data accords with that found by Kauffman et al. (2002) who found that 73.1% of Mexican – American women with PCOS (18). Also Carmina and Rogerio (2004) found the prevalence of insulin resistance using HOMA – IR to be 77% of PCOS patients (19). While Catherine et al. (2005) found insulin resistance with HOMA to be 64% (20). This difference can be attribute to ethnic difference in the group that been studied and also due to the lack of well accepted criteria for diagnosis of POCS. WHR had strong independent associated with the cumulative insulin response. WHR is strongly related to intra abdominal fat mass, which in turn more closely correlated with glucose and insulin levels than subcutaneous fat mass (21). There have been few studies examining the compartmentalization of fat in PCOS. In this study, a significant trend toward upper – body obesity in PCOS patients was noticed as it affected by higher mean value of waist, waist – to – hip ratio than their control (91.1±11.7 vs. 83±7.9, 0.84±0.07 vs. 0.75 ±0.07). These finding were in agreement with L.C. Marin – Papunen et al. which found increased upper body obesity in patient with PCOS (22). This study shows that 60% of obese PCOS had upper–body obesity in compare to only 14% of obese control. This data accord with Jan Holte's opinion who found that PCOS tend to deposit more subcutaneous fat on trunco–abdominal site and relate this finding to relatively reduce estrogen progesterone influence during anovulation which promote fat accumulation at trunco–abdominal site at expense of gluto–femoral fat (23). Our study also found that 12% of patient with lean PCOS had upper–body obesity compared to zero percentage in control. This finding is in consistence with Kirchangest and Huber. 2001 who found that majority of PCOS patients have upper body obesity (android obesity) even in lean subject (24). In this study, we make comparison among those with upper–body obesity (WHR > 0.85), lower– body obesity (WHR ≤ 0.85) and control. PCOS patients with upper–body obesity where more insulin resistance and associated with more pronounced hyperandrogenism than those with lower – body obesity which in turn more resistance than control. These data accord with other studies which demonstrated that androgen profile and insulin basal level as well as insulin response to glucose load are significantly higher in upper – body obese PCOS than lower – body obesity regardless of body mass index (25). Holte et al. (1995) found significant association between abdominal fat mass and insulin resistance evaluated by the euglycemic hyperinsulinemic clamp. He found that a highly significant correlation between fee fatty acids (FFA) concentration and insulin resistance which support the concept that an increase of FFA flux from the highly lipolytic abdominal fat to the liver and muscle may represent an important link between upper–obesity and insulin resistance (26). Upper–body obesity which has high lipolytic activity releasing FFA into blood circulation. FFA compete with glucose uptake in muscle and fat cells, resulting in increased FFA oxidation and impaired insulin mediated glucose utilization (glucose oxidation and glycogen deposition) in skeletal muscle and in acceleration of gluconeogenesis in liver (27). Upper–body obesity is thought to induce insulin resistance by expressing and secreting several peptide hormone and cytokines e.g. Tumor Necrosis Factor α (TNF α) which interestingly reported in high in obese PCOS (28). Abdominal obesity is associated with profound alteration of both production and metabolic clearance rates of major androgens and reduced sex – hormones binding globulins (SHBG) blood levels (25). Upper – body obese PCOS women androgens could, in turn, play role in regulating tissue metabolism. In fact at level of visceral depot, Testosterone stimulates lipolysis and therefore increases FFA efflux. In addition at the level of the muscle, testosterone modifies the histological structure by increasing type II, less insulin sensitive fiber. Thus upper – body obesity per se may play key role in determining both altered androgen metabolism and insulin resistance in vicious circle manner. In this study, there is a significant trend toward high percentage of β cell function ( βF), as evaluated by HOMA -%B cell, in those patient with upper–body obesity than those with lower– body obesity which in turn have high β cell function compared with control. This accords well with other authors who found that a central fat depot could (via increased level of free fatty acid) modulate the βF and increase FFA has been described as elevating the insulin secretion rate (29). The high percentage of β cells function found could be explained as compensation for degree of insulin resistance and this accord with study of Catherine et al. 2005 (20). This hyperinsulinemia also may be due to decline in hepatic insulin extraction in upper – body obesity and mediated in part by increased androgen activity (30). In conclusion, patient with high PCOS have 76.5% prevalence of insulin resistance, upper body obesity aggravates insulin resistance and hyperandrogenism of patient with PCOS and modulate β–cell function. REFERENCES
Copyright © Middle East Fertility Society The following images related to this document are available:Photo images[mf06034f2.jpg] [mf06034t1.jpg] [mf06034f1.jpg] [mf06034t2.jpg] [mf06034f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}