 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Middle East Fertility Society Journal, Vol. 11, No. 3, 2006, pp. 210-215 Use of low-dose human chorionic gonadotropin (hCG) for final follicular maturation in ovulatory women treated by intrauterine insemination Razeih Dehghani-Firouzabady, M.D. Naeimeh Tayebi, M.D. Maryam Asgharnia, M.D. Seyyed Mehdi Kalantar, Ph.D. Research and Clinical Center for Infertility, Yazd Medical Sciences University, Iran Address for correspondence: Razeih Dehghani-Firouzabady, M.D., Research and Clinical Center for Infertility, Yazd Medical Sciences University, Iran, Email: dr_firouzabadi@yahoo.com Received on June 10, 2006; revised and accepted on September 13, 2006 Code Number: mf06035 ABSTRACT
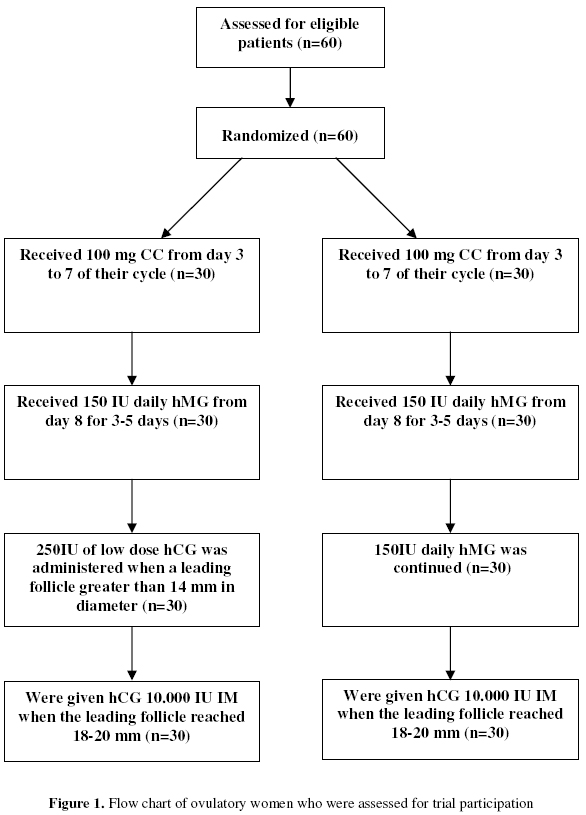
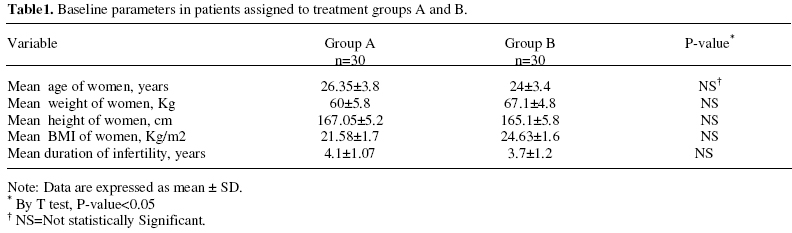
Objective: To evaluate follicle growth and maturation supported by daily late follicular phase low-dose human chorionic gonadotropins (hCG) administration following pre-stimulation with clomiphene citrate(CC) and human menopausal gonadotropin (hMG) in comparison with a sequential CC and hMG regime only. Key words: Ovarian stimulation, low-dose human chorionic gonadotropin (hCG), intrauterine insemination (IUI) Serum hormone levels in the normal menstrual cycle are characterized by an early increase of FSH during the luteal-follicular transition (1) followed by declining concentrations in the late follicular phase; conversely, LH levels across the follicular phase are initially low and then increase in the very late follicular phase as the midcycle LH surge becomes imminent (2). Hormone dynamics during gonadotropin stimulated ovulation induction and controlled ovarian hyperstimulation (COH) follow a very different course with high levels of FSH activity across the entire follicular phase, even when LH/hCG–containing preparations, such as HMG, are used (3,4). Early follicular phase concentrations of FSH are crucial to follicle recruitment, whereas later LH increments become critical for dominant follicle selection and maturation at a time of declining FSH levels (5). Some studies have demonstrated that combined FSH and LH administration significantly reduced the number of small preovulatory follicles (<10mm in diameter) (6). Recently, Filicori et al showed that in the final stages of ovarian stimulation, folliculogenesis can be supported by the administration of low-dose hCG (200 IU daily for 7 days) and that this promotes the development of numerous large preovulatory follicles (7). Also, they reported with this regimen can obtain several good quality oocytes were retrieved and fertilized by intracytoplasmic sperm injection (ICSI) can result in pregnancy (8). More recently, studies in ovulatory women have focused on the use of low-dose hCG alone in the later part of the follicular phase, following a week of more traditional FSH/HMG stimulation (9). This study was designed to evaluate the clinical outcome of a regimen using low dose hCG to complete folliculogenesis over final days of stimulation in a group of IUI patients in the expectation that this might lead to potentially more efficient regimens of ovarian stimulation for IUI. MATERIAL AND METHODS A prospective randomized clinical trial was the study design in this study. The study was performed between February and December 2005 (Figure 1). Sixty patients who met all of the inclusion criteria were randomized by using a computer generated random table, into two treatment groups. For inclusion into the study, patients had to meet all of the following criteria: age less than 40 years; normal body mass index (BMI) of 20-25 kg/m2; regular menstrual cycles; documented normal uterine cavity and patent tubes by either hysterosalpingogram or laparoscopy and no signs of polycystic ovary syndrome (PCOS) or endometriosis; with normal fasting glucose, normal serum prolactin, thyroid stimulating hormone before beginning treatment, and normal FSH on day 3 of the cycle. Finally the etiology of infertility had to be either mild male infertility (according to WHO criteria; count: 15-20X106, motility: 40%-50%, and morphology: 30%-40%) or unexplained infertility. The institutional review board gave approval for the study. All patients gave informed written consent. Patients in both groups were treated with 100 mg CC from day 3 to 7 of their cycle. From day 8, patients received 150 IU hMG (Menogon, Ferring), Then Thirty patients were randomly assigned to each group. Patients in group A, from cycle day 8 serial transvaginal ultrasound examinations were performed for them. When a leading follicle greater than 14 mm in diameter was detected, hMG therapy was replaced by the daily administration of 250 IU HCG (Pregnyl®500; Organon). A daily dose of 250 IU of HCG was administered daily by diluting an ampoule of 500 IU of HCG with 1.0 ml of normal saline and then administering SC 0.5ml of this solution. Low dose HCG was continued until the leading follicle attained a mean diameter of 18-20 mm. Patients in group B continued two ampoules of hMG (150 IU daily) and ultrasound scans was performed daily from day 8. The drug regimen was continued until the diameter of the leading follicle reached 18-20mm. Serum E2 (pg/ml) and LH (IU/L) levels were measured on day of HCG administration using an Elisa technique. Endometrial thickness (mm) was measured on the day of administration of the final ovulatory dose of hCG. Measurements were taken at the point of greatest uterine diameter perpendicular to the midsagittal plane in the fundal region and included both layers of the endometrial cavity. In both groups a final ovulatory dose of human chorionic gonadotropin (10,000 IU IM) (Gonasi HP 5000) was given when the leading follicle reached 18-20 mm. Intra uterine insemination (I.U.I) was performed 34-36 hours later. Serum B-hCG was measured two weeks after IUI. Biochemical pregnancy rate was defined as a serum B-hCG greater than 25mIU/ml and clinical pregnancy determined by detection of fetal heart beat by abdominal sonography 8 weeks after IUI. The appropriate statistical tests including Student's t test, chi-square and Fisher exact test were used to compare the results, which are expressed as means and standard deviation, using SSPS for windows. Differences were considered to be statistically significant if the p-value was <0.05. RESULTS The baseline patient characteristics of the two treatment groups are shown in Table 1. No significant difference between groups existed in any of these parameters, including age, body mass index (BMI), duration of infertility. All the patients who entered the study completed treatment. Infertility factors present in group A were mild male factor (40%), unexplained factor (60%); whereas in group B the corresponding Infertility diagnoses were not significantly different at 36% and 64%. Cycle outcomes in terms of follicle number and endometrial thickness are shown in Table 2. Group A had significantly more follicles greater than 14 mm (p = 0.035) and fewer follicles smaller than 14 mm compared with group B (p = 0.045) by the end of stimulation. Associated with the larger follicle size was a significantly higher serum E2 (pg/ml) on the day of hCG administration (368.5 ± 40 group A vs. 194.2 ± 10 group B, p = 0.015). Mean serum LH (IU/L) on the day of hCG administration was similar in both groups (p = 0.4) and no difference in the endometrial thickness between the two groups was observed (Table 2). Table 3 shows the biochemical and clinical pregnancy outcomes. The patients treated with low dose hCG (group A) achieved significantly more pregnancies than group B (26% in group A vs. 10% in group B) (T test, p =0.02). None of the pregnancies miscarried and two-twin pregnancies occurred in the group A and one in group B. Two of the patients developed moderate forms of the OHSS in group B and none in group A. The mean duration of low dose hCG administration (only given to group A patients) was 3.4 ± 0.2 days. DISCUSSION Low-dose hCG can be used to complete folliculogenesis in patients being stimulated for assisted reproduction. This small study showed that low-dose hCG was significantly better at achieving pregnancies than a conventional regimen. This approach to ovarian stimulation represents an effective and economic alternative (10). Although recombinant LH could have been a candidate drug for this study we chose to use lowdose hCG because it can function as a surrogate for LH and occupies LH receptors for more than 24 hours allowing prolonged stimulation (11, 12). The longer half-life and greater affinity of hCG for the LH /hCG receptor accounts for the potency ratio estimate of hCG-to-LH of around 1:6 (13, 14). In the group that received low-dose hGG, mean serum E2 levels on day of HCG administration were significantly higher than for the conventional regimen (group B), although LH concentrations were identical. The literature suggests that the rate of ovulation is much better (90%) in cycles where the leading follicle reached 14 mm before day 12 than when the lead follicle is slower and is only 12 mm (47% cycles ovulated) (10). In our study, low-dose hCG injections were started when the leading follicle attained a diameter of 14mm. The stimulatory action of low-dose hCG on follicular maturation is probably due to its interaction with LH receptors expressed by the granulosa cells of larger follicles and the enhanced activation of the granulose cell aromatase enzyme system (5, 9). Large follicles (>14mm) were more numerous in the group that received low-dose hCG than in the group treated with CC and HMG. Similarly, the number of small follicles was significantly lower in group A compared with group B. Filicori et al (2002) confirmed that LH administration in the form of low-dose hCG (7) or human derived menotropin (15, 16) is capable of inhibiting the development of small preovulatory follicles (<10mm) (15). In addition, granulosa cells of small follicles are incapable of responding to LH stimulation due to a lack of specific receptors (8), whereas larger ones expressing granulosa cell LH receptors continue to thrive in response to lowdose hCG administration (8). Thus, this regimen may help to limit the occurrence of OHSS, while maintaining maximum efficacy of ovarian stimulation (6). In this study and in the Filicori et al (2005) large ovarian follicles (>14mm) continued to increase in number during low-dose hCG administration (17) as was observed in this study. This pattern suggests that LH administration is capable of differentially modulating the development of ovarian follicles by stimulating the growth of larger antral follicles and restraining the number of small preovulatory follicles (6, 18, 19). No cases of ovarian hyperstimulation syndrome or miscarriage were observed in the current study in group A, but two cases of moderate OHSS occurred in group B. In a preliminary study, Kyono et al (2004) observed that late follicular phase administration of 200 IU daily of hCG was associated with a lower incidence of OHSS (20). In the present study, there was a significant difference in clinical pregnancy rates between the groups. The results of a study by Lee and colleagues (2005) showed improved growth and maturation of larger follicles could increase pregnancy success rates (21). In summary, this study demonstrates that administration of 250 IU/day of hCG can be used to replace HMG in the last 3-4 days of ovarian stimulation for patients undergoing IUI. Pregnancy rates more than doubled and no adverse consequences were detected in the patients receiving low-dose hCG treatment. REFERENCES
Copyright © Middle East Fertility Society The following images related to this document are available:Photo images[mf06035t2.jpg] [mf06035t1.jpg] [mf06035t3.jpg] [mf06035f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}