 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Middle East Fertility Society Journal, Vol. 11, No. 3, 2006, pp. 216-221 Expression of estrogen and progesterone receptors in the human endocervix Ayman Al-Hendy, M.D., Ph.D. * Hui Qun Wang, M.D., M.S.† John A. Copland, Ph.D.‡ Departments of Obstetrics & Gynecology and Internal Medicine, and Sealy Center for Environmental Health & Medicine, University of Texas Medical Branch, Galveston, Texas, USA. *Dept of Ob. Gyn., University of Texas. Medical Branch Financial support: This research has been supported by theUniversity of Texas Medical Branch, Galveston, Texas. Received on March 26, 2006; revised and accepted on June 13, 2006 Code Number: mf06036 ABSTRACT
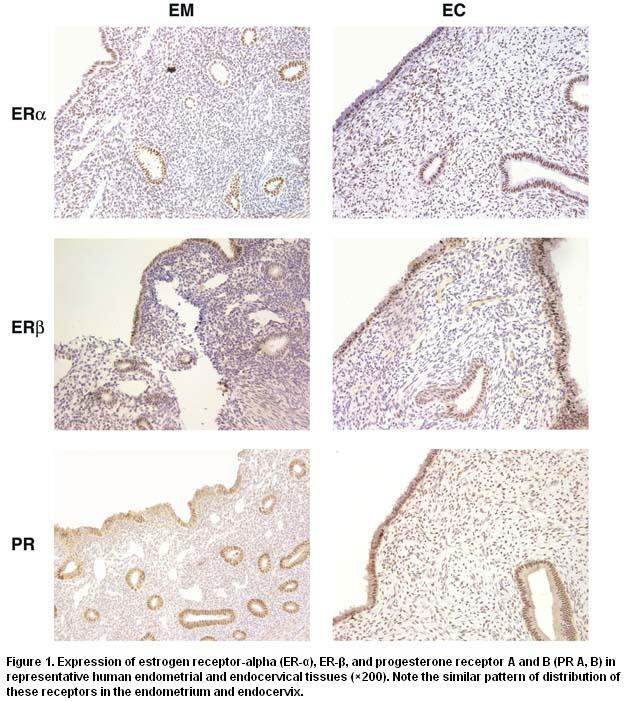
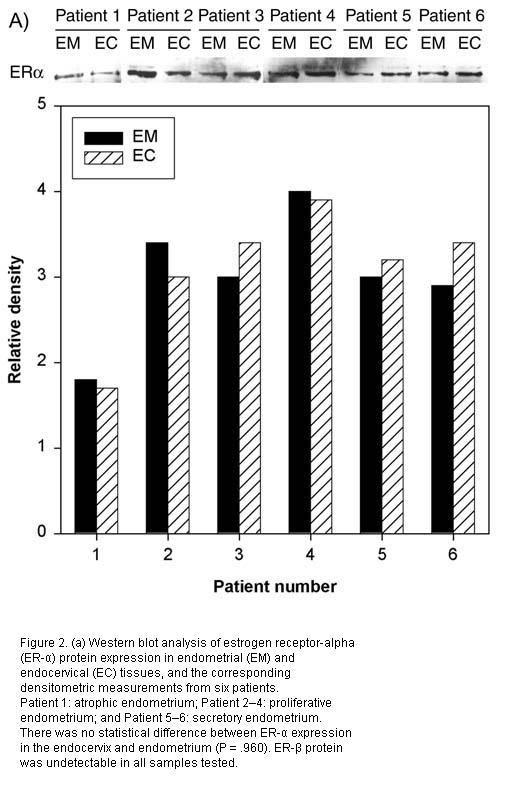
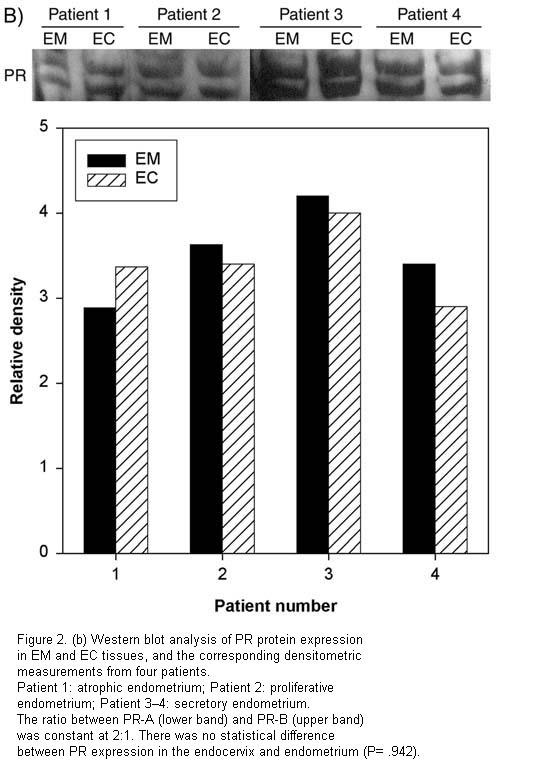
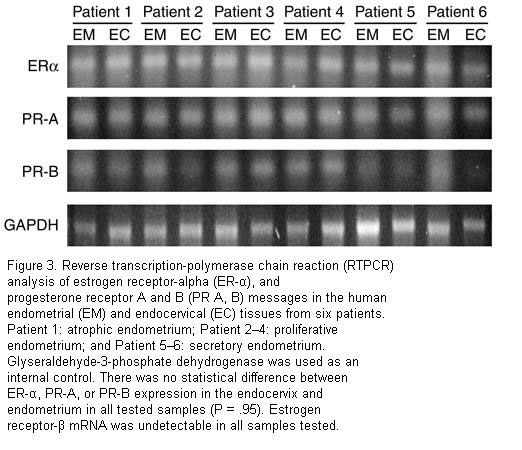
Objective: To determine the messenger RNA and protein expression, as well as distribution of estrogen receptors (ER) and progesterone receptors (PR) in the endocervix compared with the endometrium. Keywords: Endocervix, estrogen receptors, progesterone receptors. The use of unopposed estrogen alleviates menopausal symptoms, such as hot flashes, and reduces the risk of osteoporosis. However, it also significantly increases the risk of endometrial cancer (1-3). The addition of progesterone, either on a cyclic or continuous basis, greatly attenuates the increased cancer risk associated with unopposed estrogen (2,4,5). Standard medical practice dictates using combined (estrogen plus progesterone) hormone replacement therapy when indicated in women who have a uterus. Unopposed single estrogen therapy is allowed only in women who have completed a total hysterectomy (6). There are, however, no guidelines for hormone replacement therapy after a subtotal hysterectomy, a procedure involving the removal of the body of the uterus while conserving the cervix. Subtotal hysterectomies virtually disappeared from clinical practice in the 1980s but are making a comeback, with their popularity increasing among both patients and gynecologic surgeons (7). For example, the rate of this procedure has increased by 458% in Denmark from 1988 to 1998 (8). Similar trends have been witnessed in the United States (9). Little research exists on the potential effects of unopposed estrogen on the endocervix, which remains essentially intact in the case of subtotal hysterectomy. A few remote reports have demonstrated the expression of estrogen receptor in the human endocervix (10,11). Such studies are essentially using morphological methods, however, with no concurrent comparison with the endometrium. In the present study, we have studied the concurrent expression of estrogen receptors (ER) and progesterone receptors (PR) in the endocervices and endometria from the same individuals in different phases of their menstrual cycles as well as postmenopausally. This information will provide the initial step to help further our understanding of the response of the human endocervix to steroid hormones and can eventually lead to the development of appropriate guidelines for hormone replacement therapy after subtotal hysterectomy. MATERIALS AND METHODS Subjects We recruited 12 women undergoing total hysterectomy for benign indications at University of Texas Medical Branch (UTMB) Hospitals. The mean age of the recruited patients was 43 (standard deviation = 13, range = 28–67). The mean weight was 89 (standard deviation = 23, range = 66–129). The parity was 3 (median), and the range was 2 to 7. Of those patients with premenopausal endometrium, 4 were proliferative and 4 were secretory. Of those patients with postmenopausal endometrium, 4 were atrophic. Indications for hysterectomy included dysmenorrhea only (2 patients), chronic pelvic pain (5 patients), uterine prolapse (4 patients), and benign ovarian cyst (1 patient). Subjects did not use any hormonal therapy during the 6-month period immediately prior to the surgery. The study protocol was reviewed and approved by the UTMB Institutional Review Board. Uterine biopsies, processing of samples, and immunohistochemical analysis All biopsies of the endometrium and endocervix were collected by a gynecological pathologist from apparently healthy representative areas, with every attempt made to limit samples to the desired target tissue. Samples were immediately stored in liquid nitrogen and transferred to a laboratory. Immunohistochemical analysis was performed on formalin-fixed, paraffin-embedded sections as described previously (12). The mouse monoclonal antibody ER-α F-10 was used at a dilution of 1:1000 and the polyclonal antibody PR-C19 was used at a dilution of 1:800 (Santa Cruz Biotechnology, Santa Cruz, Calif). The mouse monoclonal antibody ER-β MCA1974 (Serotec Ltd, Oxford, United Kingdom) was used at a dilution of 1:2. Images were recorded by an RT Slide Digital Camera (Diagnostic Instruments Inc, Sterling Heights, Mich). Western blot analysis of ER-α and PR(A,B) Tissues were homogenized in Trizol (Sigma, St. Louis, Mo) and protein isolated as described previously (12). Equal amounts of protein (100 µg) were resolved by Tris-HCl on 8% to 16% gel and transferred to polyvinylidene fluoride paper. The membranes were blocked with 3% nonfat milk in Tris-buffered saline-Tween for 1.5 hours and then incubated overnight at 4ºC with the same antibodies described above. Bands were detected with X-Omat film (Eastman Kodak Co, Rochester, NY). Reverse transcription-polymerase chain reaction Total RNA was isolated using Trizol reagent according to manufacturer’s instructions (Sigma), and RT-PCR was performed using the Perkin-Elmer GeneAmp RNA PCR kit and RNA PCR Corekit(Perkin-Elmer;Norwalk,Conn). One microgram of total RNA was used for first strand cDNA synthesis. Primers used for RT-PCR of estrogen and progesterone receptors were kindly provided by Drs. Gregory Shipley and Peter Davies (University of Texas Health Science Center, Houston, Tex). The sequence of the sense (+) and antisense (-) primers are: hER-α (1394+) TACTGACCAACCTGGCAGACAG (1490-) TGGACCTGATCATGGAGGGT hER-β (758+) AGTTGGCCGACAAGGAGTTG (845-) CGCACTTGGTCGAACAGG hPR-A (2689+) GAGCACTGGATGCTGTTGCT (2754-) GGCTTAGGGCTTGGCTTTC hPR-B (845+)TGGGATCTGAGATCTTCGGAG (910-)GAAGGGTCGGACTTCTGCTG The sequences of the sense (S) and antisense (A)primers for GAPDH are: (S)-5'- CCA TGT TCG TCA TGG GTG TG-3' (A)-5'-TGC CCA CAG CCT TGG CAG CG-3' corresponding to bases 461–480 (sense) and 711– 730 (antisense) of the GAPDH gene (GenBank Accession No. NM002046). Each primer set was designed to cross at least one intron to rule out priming from genomic DNA. Any contribution from genomic DNA was further eliminated by observing the lack of the appropriate PCR product in the absence of reverse transcription. To ensure that the results were semiquantitative, the number of cycles used for amplification of PCR products was in the exponential range. Statistical Methods Endometrial and endocervical protein and mRNA expression measurements were compared using paired Student’s t test. A P value less than 0.05 was considered statistically significant. RESULTS Immunohistochemical analysis of ER and PR receptors The pattern of ER-α and PR staining was essentially similar in both the endometrium and endocervix. Homogeneous nuclear staining was evident throughout the entire thickness of epithelium with some reinforcement at the luminal surface (Fig. 1). Stromal cells were mostly negative, with the exception of weak scattered nuclear staining identified in both ER-α and PR. Even though this study did not attempt to quantify ER and PR staining, it was evident that postmenopausal samples demonstrated less intensity of staining, which suggests lower receptor expression (data not shown). Expression of ER-β expression was evident at a very low dilution of the corresponding antibody (1:2), which suggests minimal expression of this receptor in our samples. This was also consistent with our Western blot and RT-PCR tests, which failed to detect ER-β mRNA or protein. Throughout the different samples (proliferative, secretory, or postmenopausal), ER and PR expression followed identical patterns in both the endometrium and endocervix from the same individual. ER (α and β) and PR (A and B) expression in the human endocervix and endometrium As shown in Figures 2a, b and 3, similar patterns of ER-α and PR (A and B) expression were consistently demonstrated between the endocervix and endometrium within the same uterus. There was no detectable ER-β mRNA or protein in our samples, suggesting minimal expression of this receptor in the human endometrium and endocervix. There was always higher expression of PR-A than PR-B, both in the endocervix and endometrium, with a consistent ratio around 2:1. There was some individual variation within the ER and PR expression, probably related to menstrual phase or menopausal status; however, the limited number of samples studied would not allow a reliable investigation of these patterns. Nevertheless, the expression of ER and PR was identical between the endocervix and endometrium within the same individual. DISCUSSION Our study demonstrates comparable expression of both ER and PR in endocervix and endometrium collected from same individuals. We found that mRNA for ER-α, PR-A, and PR-B, as well as their corresponding proteins, are present in similar amounts in both the endometrium and endocervix. Using immunohistochemistry, we localized these positive signals to primarily the epithelial layers of these tissues, and, to a lesser degree, the stromal cells. Though our data is in agreement with an earlier report (10), we believe this is the first study of the expression of steroid receptors in the endocervix compared with the endometrium within the same individuals. Levels of PR-A were higher than those of PR-B, which is consistent with earlier work and may be related to differential responses to different ligands (13). Additionally, minimal staining for ER-β was detected in immunohistochemistry. This is consistent with recent reports describing higher levels of ER-α than ER-β in the endometrium (14), which suggests a differential function of these two receptors in endometrial and endocervical physiology. Both ER-α and ER-β followed similar expression patterns in both the endometrium and endocervix. The response of a given tissue to steroid hormones is a complicated process involving the steroid receptors, an array of cofactors, and other cellular elements (15). Further research is needed to elucidate the endocervical response to steroid hormones. Such information is urgently needed to assist in the development of appropriate guidelines for hormone replacement therapy after subtotal hysterectomy. This issue is particularly relevant since a considerable difference has been observed in the outcome and the side-effect profile between solitary estrogen replacement therapy and combined estrogen and progesterone replacement therapy (16, 17). ACKNOWLEDGMENTS We would like to acknowledge Dr. J.L. Simpson for review of the manuscript. We would like to acknowledge the excellent technical help of Ms. Ye Wang. REFERENCES
Copyright © Middle East Fertility Society The following images related to this document are available:Photo images[mf06036f2b.jpg] [mf06036f2a.jpg] [mf06036f1.jpg] [mf06036f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}