 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Middle East Fertility Society Journal, Vol. 12, No. 1, 2007, pp. 27-30 The prevalence of circulating anti sperm antibody (ASA) in infertile population representing of all etiologies* Amjad Hossain, Ph.D.†Nazrul Islam, M.Sc‡Subhash Aryal, M.Sc§Amos Madanes, M.D. # University of Texas Medical Branch, Galveston, Texas; The Midwest Fertility Center, Downers Grove, Illinois; University of Illinois at Chicago, Chicago, Illinois and The Midwest Fertility Center, Downers Grove, Illinois, USA *Presented in part at the annual meeting of American Society of
Reproductive Medicine (ASRM), Montreal, Canada, October 15-19, 2005. Correspondence: Amjad Hossain, Ph.D., University of Texas Medical Branch at Galveston, Dept. of Ob/ Gyn, Div of Reproductive Endocrinology, 301 University Blvd., Galveston, TX 77555-0587, Tel: 409-772-8598, Fax: 409-747-5129, Email: amhossai@utmb.edu Received May 31, 2006; revised and accepted on June 18, 2006 Code Number: mf07004 ABSTRACT Objective: The clinical significance of anti-sperm antibody (ASA) in
the etiology of infertility is slowly emerging. Both males and females can
make antibodies that react with human sperm. The objective of this study is
to investigate the prevalence of serum ASA in male and female patients at various
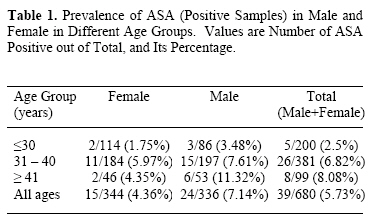
age groups. Key words: Age, ASA, Female, Male, Sera The concept that an adverse immune response to certain tissues in the reproductive system causes infertility is now more recognized than before (1-3). Consequently, the focuses are intensifying on the origin of immunological imbalances and their subsequent consequences in the reproductive function (1, 2, 4). The anti sperm antibody (ASA) is one of the many immunological markers that gets consideration in evaluating immunological infertility (5-8). It has been shown that both male and female can make antibodies that react with human sperm (9, 10) and it should, therefore, be considered as a potential fertility parameter (1, 2, 4). On the other hand, the conflicting information on the significance of ASA in the etiology of infertility is indicated (11-13). Therefore, probably, infertility practices across the world usually exclude ASA assay in screening infertility patient. This has created a scarcity of data on ASA in the current literature (1, 14). Without sufficient information on ASA, the true relevance of ASA in human fertility will remain undetermined. We have investigated ASA as an infertility parameter in a large cohort of patients, and found considerable data on this issue. MATERIALS AND METHODS Patients, irrespective of their etiologies, registered for infertility treatment in our clinic, were screened for ASA. This screening covered 680 individuals representing approximately equal proportion of males and females. The ASA was assayed on heat inactivated sera using a commercially available ASA kit (FertilPro N.V., Conception Technology Inc.) by a single technician. The analyzed sera were stored at -20o C for a second analysis when needed. The indirect test was applied following manufacturer’s suggested protocol along with a positive and negative control. Briefly, ASA negative donor sperm was incubated in test serum with anticipation that the motile sperm membrane will be coated with anti sperm immunoglobulin if present in the serum. The incubated sperm was then mixed with anti sera cocktail and latex bead mixtures, and observed under microscope. The binding of the latex beads on the sperm surface confirmed the presence of ASA in the patient’s serum in which the donor sperm was incubated. The semen analysis of ASA positive males were reviewed and compared with that of ASA negative group. The prevalence of ASA was estimated as percentage of ASA positive patients in different age and sex groups (Table 1). The strength of the relationship of positive samples with the age and sex of the patients were tested by statistical analysis (16). RESULTS Thirty nine out of 680 (5.7%) patients were ASA positive (Table 1). Irrespective of gender, the 2.5%, 6.8% and 8.1% patients were positive in the age group of ≤ 30, 31-40 and ≥ 41 yr, respectively (Table 1). The 4.4% female and 7.1% male were positive but the difference between the sexes was not significant (p = 0.12). In females, 1.8%, 6.0% and 4.4%, whereas in male 3.5%, 7.6% and 11.3% were ASA positive in ≤ 30, 31-40 and ≥ 41 yr age groups, respectively (Table 1). The statistics (likelihood ratio test) indicates that age is a significant predictor (p ≥ 0.03) of the number of ASA positive individuals in the infertile patient population (Figure 1). There was a significant difference (p ≤ 0.01) in the prevalence of ASA between age groups ≤ 30 and 31-40 yr, but the difference between the other two age groups, 31-40 and ≥ 41 yr, was not significant (p = 0.68) (Figure 1). The means of different semen parameters of ASA positive group were within the ranges of that of ASA negative group. DISCUSSION In this study we revealed the prevalence of circulating ASA in infertile population by indirect assay. The immunoglobulin found in the reproductive system and serum are diverse category (IgA, IgG, IgM etc) (4, 11). These immunoglobulin iso types may transudate from circulation into reproductive tissue and, from the reproductive tissue back to the circulatory system. However, the circulating ASA cannot predict the relative abundance, and titers of ASA isotypes in the reproductive tissues (4, 12). Direct evaluation of the secretory fluid of reproductive tissues may reveal more accurate information (8, 15). The duration of our study was 3 years (2000-2004), and at the end of the study all 39 ASA positive sera, and randomly chosen equal number of ASA negative sera were retested by the same assay system. The results of the two runs of the assay were identical. This finding is important because it shows that the ASA binding properties of sera were not compromised by prolonged storage. This study found that 6% of our infertile patient population were carrying circulating ASA. Because the sera instead of reproductive tissue secretions were screened and stringent criteria were used, detecting low levels of ASA prevalence (6%) is not unexpected. Measuring all ASA iso types (IgA, IgG, IgM) by directly analyzing reproductive tissue secretion would probably show higher prevalence rate (7, 16). We found that ASA, in both sexes, increased with age, this probably suggests that age may be a contributing factor in induction of ASA. This age related variations in the incidence of ASA may suggest that the vulnerability of different age group of patient to immunological imbalances is not the same. Finally, the semen analysis assay of ASA positive and negative samples did not identify any specific semen parameter or combination of parameters that can be indicator for ASA testing. In our observation, some apparently normal semen (by standard semen analysis criteria) were ASA positive, and on the contrary, many semen of poor quality passed the ASA test. We, thus, realized that only ASA screening but not semen analysis can confirm if a semen is ASA positive. Anti sperm antibody prevalence may not be correlated with semen parameters as seen in our study and documented by others (17); however, correlation of ASA titers with sperm motility is reported in the literature (17). From the present study, it may therefore, be concluded that : 1) less than 10% infertile patient of all etiologies is positive by circulating anti-sperm antibody, 2) no strong specific indicator of ASA testing exists in current semen analysis, 3) Cryo storage does not influence antibody titers, and 4) ASA prevalence probably increases with patient’s age. REFERENCES
Copyright © Middle East Fertility Society The following images related to this document are available:Photo images[mf07004t1.jpg] [mf07004f1.jpg] |
| |||||||||

{kind=link}
{kind=link}