 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Middle East Fertility Society Journal, Vol. 12, No. 1, 2007, pp. 31-34 Synchronization of antral follicles: a step further towards a friendly IVF Program Sherif Khattab, M.D.,Iman Abdel Mohsen, M.D.,Ismail Aboul Foutouh, M.D.,Ashraf Ramadan, M.D.,Mohamed Moaz, M.D. Egyptian International Fertility center, Misr International Hospital, Cairo, Egypt Correspondence: Prof. Dr. Sherif Khattab, The Egyptian International Fertility center, Misr International Hospital, 40, Abdel Rehim Sabry st; Dokki, Cairo, Egypt Received on June 8, 2006; revised and accepted on October 9, 2006 Code Number: mf07005 ABSTRACT Objective: To evaluate the value of synchronization of follicles using
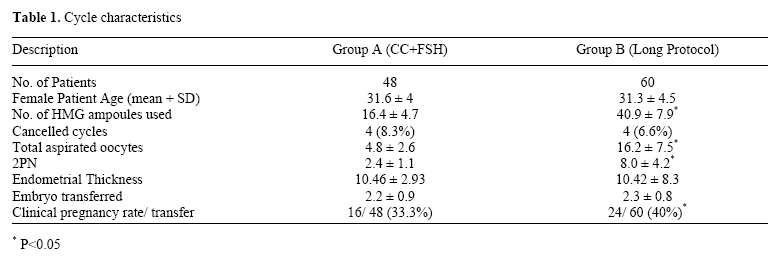
luteal phase estradiol for a friendly IVF program. Key words: friendly IVF, clomiphene citrate, ICSI, male infertility As part of the complex physiological patterns of the menstrual cycle in humans, it has been demonstrated that during the first days of the follicular phase of the cycle, early antral follicles exhibit dissimilar sizes, ranging from 2 to 8 mm in diameter (1). This can partly be explained by the inconsistent sensitivity to follicle stimulation hormone (FSH) by the developing oocytes during follicular development (2, 3). This natural phenomenon involves the exposure of early antral follicles to gradient FSH levels during the late luteal phase. During the last days of the menstrual cycle (i.e. late luteal–follicular phase transition) paralleling the corpus luteum demise, FSH levels increase progressively to preserve antral follicles from atresia, and ensure their subsequent growth (4). According to their inherent sensitivity to FSH, it is possible that some early antral follicles are able to respond to lower amounts of FSH than others and, therefore, to start their developments during the late luteal phase (5). The premature, gradual exposure of follicles to FSH may accelerate the development of more sensitive follicles and accentuate size discrepancies observed during the first days of the subsequent cycle, and eventually the formation of a dominant follicle. Moreover, these noticeable size heterogeneities may be amplified during controlled ovarian hyperstimulation (COH). In contrast to natural cycles, during COH most of the early antral follicles are required to grow coordinately in response to exogenous gonadotropins to accomplish simultaneously functional and morphologic maturation. Marked follicular size discrepancies at the end of COH may be counterproductive because they imply that a substantial fraction of FSH-sensitive follicles fail to undergo satisfactory maturation (6-7). According to their intrinsic sensitivity to FSH, some follicles are able to respond to lower FSH levels than others and, therefore, to start their development earlier, during the late luteal phase (8). Since larger follicles are more FSH responsive than are smaller follicles, exogenous gonadotrophin administration is likely to intensify further size discrepancies of growing follicles during COH. For the aforementioned reasons, the GnRH agonist long protocol has been accepted as the standard protocol for COH since it suppresses the endogenous release of FSH, allowing for follicle cohort synchronization. Recently, it has demonstrated that luteal FSH suppression achieved by the administration of E2 during the luteal phase coordinates antral follicle growth as corroborated by the reduction in their mean diameter and mutual size discrepancies both before and during COH in GnRH antagonist cycles (9-10). This has resulted in an increased cohort of mature follicles, and with less size discrepancies, during GnRH antagonist administration that mimics the effects of the standard long agonist protocols (11). In the present investigation, supported by the previous results, we wished to test the theory that luteal E2 administration could promote the coordination of follicular growth during in a low cost IVF program. It consists of administering oral estrogen (Progynova) 2 tablets /day during the luteal phase preceding COH, followed by ovarian stimulation using a combination of Clomiphene citrate (CC) and human menopausal gonadotropin (hMG). MATERIALS AND METHODS This was a prospective, controlled, pragmatic study to determine the efficiency of combining luteal phase E2 administration in order to synchronize the follicular cohort in patients undergoing COH using a CC/ hMG protocol. All patients were carefully informed of the benefits and disadvantages of using the new protocol, and informed consent was given. A total of 108 infertile couples were included in the study and divided into two groups according to couple preference. Group I (n = 48) received 4 mg E2 (Progynova, Schering, Germany) daily for 10 days in the luteal phase of the cycle preceding ICSI cycle. At day 1 of menses, transvaginal ultrasound was done to exclude the presence of basal ovarian cysts and to count the number of antral follicles. Clomiphene citrate 100mg was started on the 2nd day of the cycle for five days, and hMG (2ampoules) was administered on day 6 for 5 days. Group II (n = 60) received the standard long protocol. The dose of hMG was then adjusted according to the ovarian response as determined by serial ultrasound measurements. Human chorionic gonadotrophin (hCG) (Choriomon, IBSA, Switzerland) was given when at least when two follicles reached 17 mm, in addition to monitoring by serum E2 on day of hCG. If only one oocyte reaches 17 mm, the cycle was cancelled. Otherwise, ovum pick up was scheduled 36 hours later ICSI procedure As soon as the oocytes were identified using a stereomicroscope (Nikon, SMZ-2T, Japan), the cumulus complex was rinsed and cultured (Medicult, Denmark), then transferred to the carbon dioxide incubator 6% and 37oC temperature (Forma Scientific, USA). Standard ICSI procedure was done using an inverted microscope (Nikon,SMZ-2T,Japan) equipped with micromanipulators and microinjectors (Eppendorff, Germany). At Magnification of 400X, injected oocytes were incubated in G1 medium (Vitrolife, Sweden) at 37°c in an atmosphere of 6% CO2 (Forma Scientific Incubator, USA). Embryo transfer was carried out on day 2 -3 using a Labotect catheter. Only good quality embryos were transferred. The patient remained resting with a slight head-down tilt to her bed for 2 hours before being allowed to go home. Luteal phase support was carried out by vaginal suppositories (Cyclogest 400mg, Alpharma, England) for 14 days. Pregnancy was confirmed by determination of maternal serum B-hCG two-week post-transfer and subsequent ultrasound detection of fetal pole and cardiac pulsations. RESULTS There was no significant difference between both groups regarding age, duration of infertility and BMI. Group I showed a statistically significant reduction in duration of stimulation, dose of hMG (16.4±4.7 vs. 40.9±7.9), and number of MII oocytes retrieved (4.8±2.6 vs. 16.2±7.5). However, it also showed a significantly increase number of cycle cancellation (8.3%). Endometrial thickness was also similar between both groups (10.5±2.9 vs. 10.4±8.3). Number of embryos transferred was significantly lower in Group I (2.2±0.9 vs. 2.3±0.8) (P<0.5). There was also a lower clinical pregnancy rate in Group I (33.3% vs. 40%). As for the multiple pregnancy rates, there was only one case of twins in Group I, while in Group II 12 women had twin pregnancies (Table 1). DISCUSSION Over the years, the field of assisted reproduction has seen many compounds being developed and marketed for ovulation induction. One product has relatively held its ground as a first-line drug, clomiphene citrate (CC). The fact that CC is an orally administered and is a relatively cheap preparation has proved an enormous advantage over its injected and more expensive competitors. Clomiphene citrate (CC), a synthetic, non-steroidal estrogen receptor agonist and antagonist has been used to induce ovulation. CC therapy induces ovulation by increasing pituitary gonadotrophin output via a blockage of the normal negative feedback exerted by estrogens on hypothalamic GnRH release (12). The resulting increase in circulating FSH and LH levels triggered by CC administration initiates follicular maturation and ultimately leads to ovulation. Treatment with CC at a dosage of 50 or 100 mg/day for 5 days succeeds in inducing ovulation (13). In IVF, co-treatment with CC and gonadotrophins has been employed as an attempt to decrease costs of medications. However, in today’s modern IVF protocols, the use of CC is decreasing due to its anti-estrogenic side-effects, its limited stimulation capacity compared to the injected competitors, and the size discrepancies in antral follicle sizes (13). In the present study, couples with severe male factor of infertility were recruited as women are usually of young age and normo-ovulatory, thus expecting to respond well to treatment with CC and gonadotrophins. The results of this study demonstrate that E2 helped in reducing the discrepancies between growing follicles , and as a result synchronized the growth of antral follicles resulting in a good number of oocytes retrieved that could not be achieved with CC alone Thus, administration of E2 during the late luteal phase of the menstrual cycle helps to synchronize the antral follicle cohort by suppressing the inherent gonadotropin release by the pituitary. The low cost protocol a significantly less number of hMG ampoules, but also resulted in a fewer number of follicles retrieved than with the standard long protocol. Moreover, there is was higher rate of cycle cancellation with the CC protocol. However, in patients that reached the stage of embryo transfer, the pregnancy rates were significantly lower in the CC group but still can be considered reasonable. This should also been viewed in terms of very low multiple pregnancy rate with the CC protocol. In conclusion, this new approach is simple and effective protocol for COH in a low cost program. If its efficiency can be supported by well powered, truly randomized controlled trials, it could prove to be an attractive alternative to GnRH agonist long protocol especially in couples with male infertility. REFERENCES
Copyright © Middle East Fertility Society The following images related to this document are available:Photo images[mf07005t1.jpg] |
| |||||||||

{kind=link}