 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Middle East Fertility Society Journal, Vol. 12, No. 1, 2007, pp. 41-46 Three-dimensional ultrasonography in the evaluation of the uterine cavity Mohamed M. Momtaz, M.D.Alaa N. Ebrashy, M.D.Ayman A. Marzouk, M.D. Department of Obstetrics and Gynecology, Kasr El Aini Medical School, Cairo University Correspondence: Mohamed Momtaz, 209, 26th July Street, Mohandessin, Cairo, 12411 –Egypt. Tel.: 002-02-3478837, Fax: 002-02-3440922, Email: mmomtaz@link.net Code Number: mf07007 ABSTRACT Objective: To evaluate the use of three-dimensional transvaginal ultrasound
(3D TVS) in the assessment of uterine cavity pathology and uterine congenital
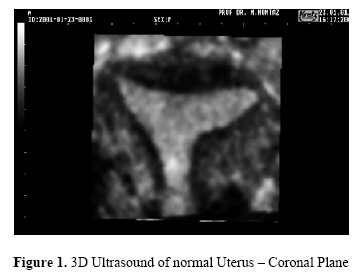
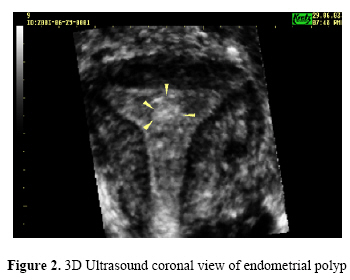
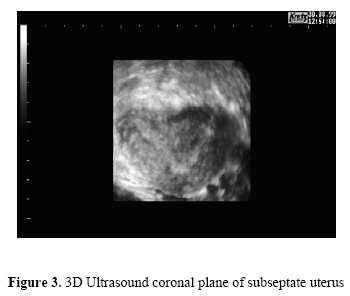
anomalies. Keywords: Uterus, uterine cavity, evaluation, ultrasound, three-dimensional, 3D, sonography The objective of an ultrasound (US) examination is to get a spatial impression of the examined organ. With the conventional technique the examination has to imagine a three-dimensional (3D) idea of the shape, size, and position of the organ examined. With the use of two dimensional (2D) transvaginal sonography (TVS), the examination of uterine lesions is limited to the transverse and sagittal planes (1), which sometimes give an inadequate view of the uterus and uterine pathology (2). Three-dimensional TVS represents a new technique of imaging. It has the ability to register all three imaging planes simultaneously as well as to visualize surfaces three dimensionally. Three-dimensional TVS enables visualization of the uterus in the coronal plane (3), which is rarely seen on conventional scans (4). It thus provides a unique diagnostic tool for non-invasive studies of the uterine morphology and diagnosis of congenital uterine anomalies (5). The coronal plane of the uterus is used to visualize both horns of the endometrium and the cervix at the same time. The normal uterus usually shows a convex shape of the endometrium (Figure 1) and myometrium in the fundus (6). La Torre et al (7) showed that studying the coronal plan of the uterus acquired froma3Dvolumeimprovesthe visualizationofpossibleinteractionsbetween structuressuchasuterine fibroidsandpolyps(Figure 2). The frontal plan of the uterus also offers marked improvements for studying uterine malformations (Figure 3) (8, 9), especially in cases of infertility (10). 3D TVS is helpful in delineation of intracavitary adhesions and determination of their location that assists in surgical planning. It is beneficial for differentiation between polyps and submucous myomas (Figure 4) (11). Our objective was to determine the potential advantage of 3D TVS over other conventional methods including 2D TVS and hysterosalpingography (HSG) alone or in combination for the assessment of uterine cavity lesions. MATERIALS AND METHODS A prospective study was conducted at the Obstetrics and Gynecology Department of Kasr El Aini Hospital, Cairo University in the period between January 2003 and December 2005. The study included 132 patients in the age group between 21-72 years with a mean of 35.9 + 11.9 (SD) years. Various clinical presentations were encountered in the study group (Table 1). Criteria of inclusion were all patients who were suspected to have a uterine cavity lesion or abnormality on 2D TVS or HSG. After taking consent, all patients were subjected to history taking and clinical examination, ultrasonographic evaluation using Voluson 530D (GE Medical Systems); including 2D TVS and 3D TVS evaluation, HSG, and Hysteroscopy / Laparoscopy. Results were analyzed using sensitivity (SE); specificity (SP), positive predictive value (PPV); negative predictive value (NPV) and positive and negative likelihood ratios (PLR, NLR). All statistical calculations were done using Microsoft Excel® and SPSS® (Statistical Package for the Social Science). RESULTS We examined 123 cases by transvaginal 2D, HSG, 3D TVS and hysteroscopy / laparoscopy. Twenty-one cases had normal uterine cavity and no uterine pathology where 102 patients had a uterine cavity abnormality or pathology on the final diagnosis. Thirty-eight cases had a Mullerian anomaly (Group I) whereas there were myomas either single or multiple in 32 cases and endometrial polyps in 20 (Total = 52) (Group II). Twelve cases had intrauterine adhesions (Group III) (Table 2). In Group I (Table 3), SE, SP, PPV and NPV were highest for 3D TVS (0.97, 0.96, 0.92 and 0.99 respectively) but comparable to 2D TVS + HSG (0.95, 0.94, 0.90 and 0.95 respectively). These were higher than 2D TVS or HSG alone. The positive likelihood ratio (PLR) and negative likelihood ratio (NLR) values were strong for 3D TVS (27.6 and 0.03) and 2D TVS + HSG (14.7 and 0.08). However, for 2D TVS, only PLR was strong (11.7) and for HSG, only NLR was strong (0.07). In Group II (Table 4), 3D TVS showed highest SE and NPV where SP and PPV were comparable to 2D TVS, HSG or to both techniques combined. The PLR was similarly strong in 2D TVS, 2D TVS + HSG and 3D TVS; it was borderline for HSG alone. However, the NLR was only strong for 3D TVS. Table 1. Clinical presentation of patients in the study group
Table 2.Patients’ final diagnosis on Hysteroscopy / Laparoscopy
In Group III (Table 5), all methodologies showed high SP and NPV with low SE and PPV. The PLR was strong for HSG, alone or in combination with 2D TVS, and for 3D TVS but not for 2D TVS. However, the NLR was weak to moderate for all methods. DISCUSSION The acceptance of 2D TVS as a screening tool for the presence of uterine pathology is beyond any doubt, however recently with the introduction of 3D TVS; this is obviously being challenged specially concerning the uterine cavity anomalies and the uterine cavity lesions. Being an easy and non-invasive office procedure, it definitely surpasses the HSG in evaluating the uterine cavity. Furthermore, it visualizes the frontal (coronal) plane of the uterus that is not seen by HSG (12). Congenital uterine anomalies are associated with an increased risk of repeated first and second trimester miscarriage and preterm delivery (13). Accurate and reliable diagnosis is important therefore as it allows the identification of patients at risk of these complications and timely surgical intervention. This is undoubtedly the area where three-dimensional sonography has contributed the most and has become the investigation of choice in units where available. This reflects its ability to demonstrate both the endometrial cavity and the myometrium simultaneously in the coronal plane (2). Raga et al. (10) and Wu et al. (14) both reported favorable results suggesting three-dimensional sonography offered 100% specificity for the exclusion of uterine anomalies and was able to differentiate between the different anomalies. In our study, 3D TVS showed high SE (97%) and SP (96%) for the detection of uterine cavity anomalies. It also showed excellent NPV(99%) and Table 3. 2D TVS. HSG and 3D TVS in cases of Group I (Mullerian anomalies)
PPV (92%). The PLR was 27.6 and NLR was 0.03, which provide strong evidence to the value of 3D TVS in both diagnosis and ruling out of uterine anomalies. The combination 2D TVS + HSG showed similar but less strong ratios (PLR=14.7, NLR=0.08). However, 3D TVS would definitely be less invasive and less expensive than doing both of these tests. La Torre et al. (7) compared 3D TVS with conventional imaging with and without saline contrast in their study of 23 patients in whom subsequent hysteroscopy revealed the presence of 16 endometrial polyps. Standard 2D TVS demonstrated a relatively poor SP of only 69.5% suggesting the presence of polyps in 23 patients. This was improved to 94.1% when 2D TVS was used in conjunction with saline infusion as only 17 patients were then thought to have polyps. 3D TVS performed almost as well diagnosing the presence of polyps in 18 patients with a SP of 88.8% and subsequently correctly identified all 16 polyps when used in conjunction with saline infusion. In Group II of this study, 52 patients had submucous myomas and endometrial polyps diagnosed on hysteroscopy. All diagnostic modalities (2D TVS, HSG and 3D TVS) had reasonable SP (96%, 91%, and 97% respectively) but they, except for 3D TVS, had low SE (79%, 65% and 96% respectively). The difference between this study and the results of Le Torre et al. (7) probably comes from the fact that we included both submucous myomas and polyps in one group whereas they studied only polyps. In comparing the likelihood ratios for different methodologies' ability to diagnose submucous myomas and polyps; 2D TVS, 2D TVS + HSG and 3D TVS showed strong PLR (19.7, 20.0 and 34.1) whereas HSG alone had a moderate PLR (7.7). On the other hand, only 3D TVS had a strong NLR (0.04) suggesting its ability to rule out uterine myomas and polyps with greater precision than any other technique singularly or combined. A similar improvement in specificity with 3D TVS has been shown by Sylvestre et al. (15) in their study of 209 subfertile patients thought to have an intrauterine lesion on transvaginal two-dimensional sonography or hysterosalpingography. In our study, we could show that 3D TVS coronal plane examination of the uterine cavity without saline infusion is as sensitive and specific as the results of saline infusion sonography whether 2D or 3D (9, 15). Table 4. 2D TVS. HSG and 3D TVS in cases of Group II (Myomas and Polyps)
Table 5. 2D TVS. HSG and 3D TVS in cases of Group III (Intrauterine adhesions)
3D TVS offers a reliable and standardized tool to diagnose, differentiate and quantify uterine anomalies. It has significantly added to our understanding of uterine anomalies qualifying their effect on reproductive outcome and thereby helping the clinician counsel patients accordingly and confidently. Concerning the lesions within the substance of the uterus not involving the cavity it was shown that 3D TVS did not offer better opportunity than 2D TVS concerning diagnosis except in more diagnostic perception of the size and site of the lesion (16). However, the spatial and the reconstructed image produced by the 3D frontal view of the uterus is more informative especially when it comes for the decision of management either, myomectomy through open surgery, or hysteroscopic myomectomy (17). We recommend the use 3D TVS in cases with suspected uterine Mullerian anomalies involving the uterine cavity. It has several advantages over HSG, 2D TVS and Hysteroscopy, mainly its ability to visualize the uterus in coronal plane visualizing both the endometrial cavity and the surrounding myometrium. Also, 3D TVS is highly beneficial in cases with suspected submucous myoma and endometrial polyps. It is most valuable in delineating their location and position in relation to the cavity, which is essential in planning to surgical management and the choice of surgical method whether hysteroscopic or laparotomy. In cases of suspected intrauterine adhesions, 3D Sonohysterography may be more valuable in delineating their presence and extent especially in mild cases that may be missed by 3D TVS alone (18,19). REFERENCES
Copyright © Middle East Fertility Society The following images related to this document are available:Photo images[mf07007f2.jpg] [mf07007f1.jpg] [mf07007f3.jpg] [mf07007f4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}