 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
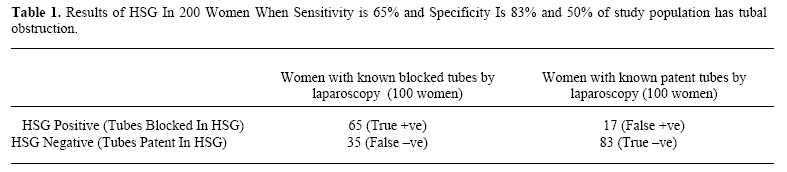
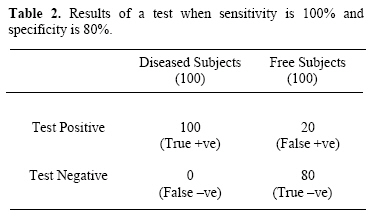
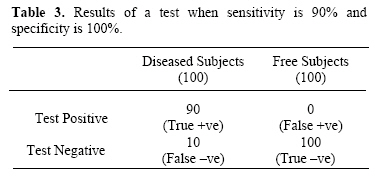
Middle East Fertility Society Journal, Vol. 12, No. 1, 2007, pp. 69-72 EVIDENCE-BASED MEDICINE CORNER Evidence-based diagnosis: II. Sensitivity and specificity Abdelhamid Attia, M.D. Prof. of Obstetrics & Gynecology - Cairo University; President of the Arab Federation of Evidence-Based Medicine Code Number: mf07013 Practicing EBM requires certain steps which are: 1) to assess the patient, 2) to phrase a question, 3) to search the literature for evidence, 4) to appraise the evidence, and 5) to apply the evidence to patient care. Clinical Scenario You are working at your clinic when 2 patients who complain of infertility (Mrs. A and Mrs. B) came to you with their hysterosalpingography (HSG) results. Looking into their hysterosalpingograms you find that Mrs. A has a “negative result” (tubes patent) and Mrs. B has a “positive result” (tubes obstructed). Knowing that the results of semen analysis of both partners and midluteal serum progesterone of both women are normal; you decide to start treatment for Mrs. A and plan for laparoscopy for Mrs. B. But you were stopped by a question from Mrs. A saying “Doctor! What is the probability that this test result is wrong and that I am going to start treatment that will not work for me?” and from Mrs. B saying: “What is the probability that this result is wrong and that laparoscopy would be unnecessary?” The problem You know correctly that any test result is never certain. This means that a positive test result does not necessarily mean that the patient is having the disease and vice versa. Thus, you need to know exactly the probabilities of having or not having the disease or disorder in question and to answer the questions of your patients properly. As you now know, from the first part of this article, you have to calculate a pre test probability of having the disease then calculate the posttest probability of having (or not having) it. This needs a search for articles that evaluated the accuracy of HSG in diagnosing or excluding tubal obstruction. The search Unlike therapy in which randomized controlled trials give the highest evidence, for diagnosis research the cross sectional double blind comparison with a gold standard is the best study design to answer questions about diagnosis. When searching for evidence we first search for a systematic review that addressed the problem at hand and in absence of systematic reviews we search for original primary studies. The gold standard for the diagnosis of tubal disease in comparison with HSG is laparoscopy. So you would like to have a systematic review or a meta-analysis for articles that studied the accuracy of HSG compared with laparoscopy for the diagnosis of tubal disease. Searching the PubMed using hysterosalpingo-graphy as a key word and limiting the search to meta-analysis retrieved 5 articles only (Fig 1). You read the abstracts and find that only one of them addresses your query (1). This meta-analysis has analyzed 20 studies with 4197 patients for whom both HSG and laparoscopy had been performed for comparison. In this meta-analysis the sensitivity of HSG was found to be 65% and the specificity 83%. Now given these data about HSG; howare you going to answer your patients? Sensitivity and Specificity? Sensitivity is “the probability of a positive test among those who have the disease”. It equals number of diseased individuals who tested positive divided by the total number of diseased individuals. For example if you tested 100 diseased individuals with a new test that gave you 92 positive results (which are true positive here) and 8 negative results (which are false negative here) this test has a sensitivity of 92/100 = 92%. Thus it is important to emphasize that there are always false negative results whose probability equals 100 minus sensitivity (%) which mean in this example that 8% of the real patients who would be tested would have a negative test result i.e. diagnosed wrongly by the test as free from the disease. Specificity is “the probability of a negative test among those who are free from the disease”. It equals number of disease-free persons who tested negative divided by the total number of disease-free individuals For example if you tested a 100 free individuals (not having the disease) with a new test that gave you 88 negative results(which are true negative here) and 12 positive results (which are false positive here) this test has a specificity of 88/100 = 88%. Thus it is important to emphasize that there are always false positive results whose probability equals 100 minus specificity (%) which mean in this example that 12% of the free individuals who would be tested would have a +ve test result and would be diagnosed wrongly as having the disease. Sensitivity and specificity are not helpful to clinicians as they only tell us how the test works in the population but not whether a specific patient has the disease or not. Thus given the above sensitivity and specificity for HSG in diagnosing tubal obstruction we can only conclude that HSG correctly diagnoses 65% of patients with tubal obstruction meanwhile 35% would be falsely diagnosed as having patent tubes. While it correctly identifies 83% of women with patent tubes meanwhile 17% would be falsely diagnosed as having tubal obstruction. This can be illustrated more by studying a population of 200 women in which 100 women have tubal obstruction and the other 100 have patent tubes and see how does the test work in them (Table 1). SnNout It is important to know that even a test with 100% sensitivity, in which all diseased individuals would test +ve, is not good for diagnosing or ruling in the disease if it has a lower specificity. On the contrary this test is used better to exclude or rule out the disease rather than to diagnose its presence (Table 2). From the above table we observe that when sensitivity is 100% and specificity is 80% all diseased individuals will test +ve but also 20% of free individuals will test +ve. Thus, there are two possibilities for a patient with a +ve test result. She may have the disease if her result is a true +ve one but she also might be diagnosed wrongly as having the disease if her result is a false +ve one. We can also observe that 80% of free individuals will test –ve and that none of the diseased individuals will test –ve. Thus there is only one possibility for a patient with a –ve test result. She would be diagnosed correctly to be free from the disease. So the mnemonic “snNout” means that: when Sensitivity is high a Negative test result rules out the disease. SpPin It is also equally important to know that even a test with 100% specificity, in which all disease-free individuals would test -ve, is not good for excluding or ruling out the disease if it has a lower sensitivity. On the contrary this test is used better to diagnose or rule in the disease (Table 3). From table three we observe that when sensitivity is 90% and specificity is 100% all disease-free individuals will test -ve but also 10% of diseased individuals will test -ve. Thus, there are two possibilities for a patient with a -ve test result. She may be free of the disease if her result is a true -ve one but she also might be diagnosed wrongly as free of the disease if her result is a false -ve one. We can also observe that 90% of diseased individuals will test +ve and that none of those who are free from the disease will test +ve. Thus there is only one possibility for a patient with a +ve test result. She would be diagnosed correctly to have the disease. So the mnemonic “SpPin” means that: when Specificity is high a Positive test result rules in the disease. Now back to Mrs. A and Mrs. B questions you now know that knowing the sensitivity and specificity of HSG can not help you, as such, to answer their questions. You can only tell them at this moment that HSG misses the correct diagnosis of patent tubes in 17% of the cases and of obstructed tubes in 35% of the cases. What you really need to know is what is the probability of a patient with a +ve test to have the disease and what is the probability of a patient with a –ve test to be free from the disease. So, here it looks that a better measure would be the +ve and –ve predictive values of the test that would be covered in the coming article about diagnosis. REFERENCES
Copyright © Middle East Fertility Society The following images related to this document are available:Photo images[mf07013t3.jpg] [mf07013t2.jpg] [mf07013t1.jpg] [mf07013f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}