 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Middle East Fertility Society Journal, Vol. 12, No. 2, 2007, pp. 77-85 REVIEW Gonadotrophins for idiopathic male factor subfertility: a Cochrane systematic review Abdelhamid M. Attia, M.D. ,Hesham G. Al-Inany, M.D., Ph.D. ,Michel L. Proctor; M.Sc. Department of Obstetrics and Gynecology, Cairo University, Cairo, Egypt Correspondence: Hesham Al Inany, M.D., E-mail: kaainih@link.net Received on January 18, 2007; revised and accepted on March 6, 2007 Code Number: mf07015 ABSTRACT Objectives: To determine the effectiveness of
gonadotrophins administration to men with idiopathic subfertility on
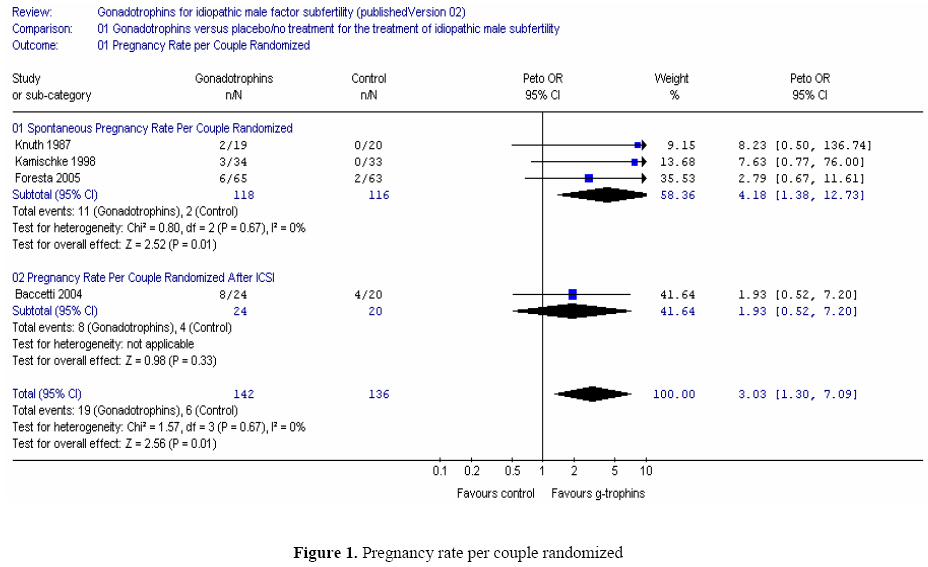
spontaneous pregnancy rate and in assisted reproductive techniques. BACKGROUND Infertility represents a problem in 15% of couples who try to have a child. While male factor alone is responsible for 30% of cases of infertility, a combination of male and female factors affect another 20%. Thus, it is estimated that male factor contributes to 50% of infertile couples (1). Gonadotrophins, follicle stimulating hormone (FSH) and luteinizing hormone (LH), play an important role in the process of spermatogenesis maintaining the production of adequate numbers and good quality sperm cells. LH affects spermatogenesis via its effect on testosterone synthesis. The mechanism by which FSH regulates spermatogenesis is poorly understood. In animal models (adult male rhesus and bonnet monkeys) blocking FSH receptors by active immunization or pituitary FSH desensitization leads to suppression of spermatogenesis, a drop of sperm count, poor sperm motility and deficiency of acrosomal enzymes leading to infertility (2,3). Neutralizing circulating endogenous FSH by ovine anti-FSH antibodies in human volunteers was associated with a drop in both the quality and the quantity of sperm cells produced (4). Acosta and colleagues reported that the systemic administration of FSH to men with severe male factor infertility, improved fertilization and pregnancy rates in vitro fertilization (IVF) cycles (5, 6). More recently the effect of FSH administration on sperm parameters in subfertile men has been examined in randomized controlled trials. One study reported that administration of recombinant human FSH (r-hFSH) was not associated with a change in sperm parameters in men with idiopathic infertility (7); other studies on men with idiopathic oligozoospermia reported an increase in sperm concentration and spermatogonial population on fine needle aspiration (8,9). The administration of gonadotrophins was associated with a significant increase in fertilization rate in IVF cycles in a subgroup of men with poor sperm motility, morphology, and count (oligoasthenoteratozoospermia) (10). Such an increased fertilization rate was not observed in men with severe male factor or oligoasthenoteratozoospermia undergoing intra cytoplasmic sperm injection (ICSI) cycles in other studies (11). Therapeutic modalities that use semen quality rather than pregnancy rates as an outcome measure might prove misleading. Randomized controlled trials that report pregnancy rate after gonadotrophin administration to subfertile men have been conducted. The use of r-hFSH or purified FSH in men with idiopathic subfertility, was not associated with a significant increase in pregnancy rates in intra-uterine insemination (IUI) and ICSI cycles in some studies (7,11) and was associated with a significant increase in pregnancy rate in others (12). Thus, we decided to conduct a meta-analysis to review the evidence for gonadotrophin administration for idiopathic male factor. Objectives To determine the effectiveness of systemic FSH administration to men with idiopathic subfertility on spontaneous pregnancy rate and in assisted reproductive techniques (IUI, IVF, ICSI). Criteria for considering studies for this review Types of studies: Any randomized controlled trial where gonadotrophins were administered for the treatment of idiopathic male subfertility. Trials where couples received more than one cycle of IUI, IVF or ICSI after randomization were included and the number of cycles recorded. Types of participants Men with idiopathic infertility diagnosed by subnormal semen parameters, according to the WHO 1999 criteria, including oligospermia, teratospermia, asthenospermia, and non obstructive azoospermia. Subnormal sperm parameters are defined as (13): sperm concentration = < 20 million sperm/mL. motility = < 50% motile sperm. normal morphology = < 30% Types of interventions Systemic administration of all types of FSH (urinary, purified or recombinant) to men with subfertility whose partners are undergoing assisted reproductive techniques (IUI, IVF, ICSI). Types of outcome measures Primary outcome * Live birth rate per couple randomized or, if not reported Secondary outcomes * Clinical pregnancy rate per couple randomized (confirmed by fetal heart on ultrasound) * Miscarriage rate per couple randomized: confirmed by ultrasound and urine or blood pregnancy test. * Adverse effects of the drugs used, if any. Methods of the review Trials identification The search strategy described above was used to obtain titles and, where possible, abstracts of studies that are potentially relevant to the review. The titles and abstracts were screened by one reviewer *A. Attia, who discarded studies that were clearly ineligible but aiming to be overly inclusive rather than risk losing relevant studies. Two reviewers, A. Attia and H. Al-Inany, independently assessed studies for inclusion in accordance with the mentioned criteria. Disagreements were resolved by consensus or through arbitration by M. Proctor. Further information was sought from the authors where papers contained insufficient information to make a decision about eligibility. Quality assessment and data extraction All assessments of the quality of trials and data extraction were performed independently by two of the three co-reviewers (AA & HA) using forms designed according to Cochrane guidelines. A third co-reviewer (MP) resolved discrepancies. Additional information on trial methodology and/or actual original trial data were sought from the authors of trials which appeared to meet the eligibility criteria but have aspects of methodology that are unclear, or where the data are in a form unsuitable for meta-analysis. Trials were analyzed for the following quality criteria and methodological details; this information is presented in the table of characteristics of included studies and helps provide a context for discussing the reliability of results. (1) Method of randomization: randomized (e.g. by computer, or random number tables or drawing lots), quasi-randomized (e.g. by hospital number or date of birth) - these trials were excluded from the review, not clear (e.g. stated but not further described). (2) Concealment of allocation: (A) adequate (e.g. by third party or sealed opaque envelopes), (B) not clear (e.g. not stated, or 'envelopes' stated without further description), (C) inadequate (e.g. open list of allocation codes). (3) Presence or absence of blinding to treatment allocation (4) Duration and type of follow-up (5) Number of participants recruited, randomized, excluded, analyzed or lost to follow up (6) Location of trial; single-centre or multi-centre (7) Timing of trial (8) Whether an intention to treat analysis was done (9) Whether a power calculation was done (10) Source of funding (11) Criteria for including participants and assessing outcomes Data Analysis Statistical analysis was performed in accordance with the guidelines for statistical analysis developed by the Menstrual Disorders and Subfertility Group. Heterogeneity between the results of different studies was examined by inspecting the scatter in the data points and the overlap in their confidence intervals and, more formally by checking the results of the chi-squared tests. A priori, it was planned to look at the possible contribution of the factors listed above to any heterogeneity identified in this manner. Where possible, the outcomes were pooled statistically. All the outcome measures for this review used dichotomous data (for example, pregnancy rate is the number of pregnancies over the number of couples treated). Results for each study was expressed as odds ratio with 95% confidence intervals and combined for meta-analysis with RevMan software using the Peto-modified Mantel-Haenszel method using a fixed effect model. Although all potential included trials might be statistically homogeneous, difference in clinical parameters may be considerable (clinical heterogeneity). These differences were taken into account when analyzing and interpreting the pooled results. Clinical heterogeneity in subfertility cannot be avoided because most centers use their own "materials and methods", which can vary along a number of parameters. When trials met the inclusion criteria and they have performed the same intervention, we considered it appropriate to pool their results. The pregnancy outcomes are considered positive consequences of treatment therefore a higher proportion of women achieving pregnancy is considered a benefit, whereas the outcome of adverse effects is a negative consequence therefore higher numbers are considered to be detrimental. This will need to be taken into consideration when viewing the summary graphs. Description of studies A total of fourteen trials were identified. The electronic searches identified thirteen controlled trials that used gonadotrophin treatment for idiopathic male subfertility and one trial was obtained via personal communication with the author (14). All trials were thoroughly appraised for their eligibility in the review and their methodological quality. Excluded studies: Eight trials were excluded as they did not fulfill our inclusion (or met our exclusion) criteria. Three RCTs were excluded as pregnancy rates were not compared (8, 9, 15). We contacted the authors of these three trials for possible data on pregnancy rates that was not published but received confirmation on the absence of such data. Another RCT was excluded as it was a partial cross-over study and pregnancy rates, also, were not reported (10). The other four trials were excluded as they were all non-randomized (16-19). Included studies: Five studies met the inclusion criteria (7, 12, 14; 20, 21). A sixth trial, of quasi randomized design (11) has been included in the discussion but excluded from all analysis. Details of each study are provided in the table "Characteristics of Included Studies". Participants: Males: All trials included males with idiopathic infertility based on subfertile semen parameters. Male infertility was diagnosed in a different way by each trial. Diagnostic criteria were according to World Health Organization (WHO) 1987 criteria (21), WHO 1992 criteria (7), WHO 1999 criteria (12), sperm count between 0.1-10 Mil/mL (20) and sperm count < 10 Million/mL in at least three separate occasions (14), and one study (11) included males with severe idiopathic infertility defined as sperm count < 5 Million/mL, <10% sperm progressive motility, and < 4% normal forms (strict Kruger criteria). Age of the participants was comparable in the six trials (details in table of characteristics of included studies). Female partners: Female partners had normal fertility in four trials (12; 14; 7; 20). In the trial of Ashkenazi 1999 (11) there was no mention to the state of fertility of the female partners. Female partners in the trial of Matorras 1997 (21) had a variety of causes of infertility but comparing the distribution of female causes among the two groups no significant difference was found. Interventions: Males: HMG/HCG treatment was used in one study (20), purified or highly purified FSH was used in three studies (11; 12; 21) and recombinant FSH in two studies (14; 7). HMG/HCG was used in a dose of 150 IU hMG three times a week and 2500 IU hCG twice/week for 13 weeks (20). Purified FSH was used in a dose of 75 IU daily for 50 to 71 days (11), 150 IU/day for 12 weeks (12), and three times per week up to eight months (21). Recombinant FSH was used in a dose of 150 IU daily for 12 weeks (7) and 100 IU r-hFSH i.m. on alternate days for three months (14). FSH therapy was compared to placebo in two trials (7; 20) and to no treatment in the control group in the other four trials (11; 12; 14, 21). Female partners: Female partners received no treatment in one trial (20), IVF or ICSI and ET was performed after ovarian stimulation, follicular monitoring and aspiration in two trials (11; 12) with luteal phase support in the former and ovarian stimulation and IUI in one trial (21). The trial of Kamischke 1998 (7) did not state which interventions may have been used with female partners although pregnancies were reported to occur either spontaneously, after IUI, IVF, or ICSI. In the trial of Foresta 2005 no intervention was used with the female partners in the first six months of the trial then patients were re-randomized into either IVF, ICSI, or IUI. Such a design invalidates the results of the last three months period in the study as it interferes with the first randomization and renders the chances of pregnancy due to the treatment studied unequal between the two groups. (14) Outcomes: Live birth rate per couple randomized: None of the six trials reported live birth rates. Pregnancy rate per couple randomized: Pregnancy rate was reported in the six trials. Pregnancy was diagnosed by ultrasound (US) at 6 to 7 weeks (21), by US six weeks after embryo transfer (12), by US and B-HCG concentration increase (7), by measuring B-HCG plasma level (14), and two studies did not mention the method of diagnosing pregnancy (11; 20). Miscarriage rate per pregnancy: None of the six trials reported miscarriage rate. Adverse events: Only two trials clearly addressed the side effects of the drugs used (20, 21). Other outcomes: Other surrogate outcomes such as fertilization rates, effects on sperm count, motility, and morphology were not included in the analysis as we excluded studies that reported only such surrogate outcomes without reporting pregnancy rates and because such outcomes are intermediate ones that are of secondary importance compared with the patient-oriented outcome (e.g. live birth or pregnancy rate). Duration of follow-up The duration of follow-up periods varied between the studies. Couples were followed up only during the treatment period in two studies (12; 21). In one study couples were followed up during treatment then for further 12 weeks after (20). In Kamischke 1998 (7) trial patients were followed-up during the treatment period then for another 12 weeks during which assessment examinations were done then for another three months follow up period during which pregnancies were recorded. In Foresta 2005 trial couples were followed up during treatment and for three months after end of treatment then, depending on their sperm count, they were either allocated directly or re-randomized into groups to receive either three cycles of IUI or one cycle of IVF/ICSI. In Ashkenazi 1999 trial the follow up period ended by the end of the treatment but pregnancies were reported several months after the end of the follow-up period. Methodological quality of included studies Randomization and Allocation Concealment Two trials stated they used true randomization by third party without reporting any further details of the method (12; 7). One trial reported randomization using a random numbers table (14). One trial used a computer generated random table (21). One trial stated it was random but did not report the method of randomization (20) and one trial used quasi-randomization by alternate assignment (11). The quasi randomized trial was not included in the analysis. Allocation concealment was considered to be adequate in the three trials that used third party randomization (12; 14; 7). One study did not use allocation concealment (11) and in two studies allocation concealment was unclear (20; 21). Blinding Two trials were double blind (7; 20) and the other four trials were open (11; 12; 14; 21). Withdrawals and Dropouts Numbers of withdrawals and dropouts in trials were generally low. Four studies did not have any withdrawal or dropout in assessment of pregnancy rates (11; 12; 20, 21) while in the study of Kamischke 1998 four patients were excluded from pregnancy analysis. In the trial of Foresta 2005 six patients were excluded from the study after randomization and ten dropped out (see the table of characteristics of included studies for further detail). Power calculation None of the studies included an adequate sample size and five studies did not include power analysis to detect differences in pregnancy rates. Only one trial reported a power calculation to detect differences in pregnancy rates (21). However, the authors reported in their study that the calculated sample size to demonstrate that the pregnancy rates per woman found were statistically different (should that be the case), with a power of 90% and an alpha error of 0.05 would require 878 study couples and 878 control couples. Sources of funding Three trials did not report sources of funding (11, 14, 21). The trial of 12 was funded by a grant from the Italian Ministry for Universities and Technological Research, 2000, that of Kamischke 1998 was supported in part by the Federal Health Ministry (Bonn), the Deutsche Forschungsge-meinschaft (DFG, Bonn) and Ares-Serono (Unterschleissheim, Germany), and the study of Knuth 1987, HMG/HCG and placebo preparations were offered by Serono Co. RESULTS Live birth rate per couple randomized None of the included trials reported the live birth rate. Pregnancy rate per couple randomized Five trials with 426 participants were included in the meta-analysis (12, 14, 7, 20, 21). The trial with quasi randomization was excluded from the meta-analysis (11). We analyzed the results on the intention to treat basis adding the 16 excluded and drop out cases in the trial and the four drop out cases in the trial of Kamischke 1998 trial to the their corresponding groups and using the worst case scenario by considering the excluded pregnant case in Kamischke 1998 trial in the control group. Owing to the "temporary effect of treatment" we analyzed the results in three subgroups as follows: Pregnancy rates per couple randomized during the treatment period, pregnancy rates per couple randomized during the treatment period and for three months post-treatment follow-up, and, pregnancy rates per couple randomized during the treatment period and for more than three months post-treatment follow-up. Overall pregnancy rate per couple randomized (during treatment period): Pooling the results from the five trials showed a significant difference in the overall pregnancy rate per couple randomized (during treatment period) in favor of the FSH treatment group; OR 1.8, 95% CI (1.03 - 3.17) with a 21.9% pregnancy rate (46/210) in the FSH group and 16.6% (36/216) in the control group. The fixed risk difference is 0.07, 95% CI (0.00 - 0.13) and the number needed to treat is 14, 95% CI (8 - 100). Overall pregnancy rate per couple randomized (during treatment and up to 3 months post-treatment follow-up): Pooling the results from the five trials showed a significant difference in the overall pregnancy rate per couple randomized (during treatment and up to 3 months post-treatment follow-up) in favor of the FSH treatment group; OR 1.92, 95% CI (1.15 - 3.20) with a 25.7% pregnancy rate (54/210) in the FSH group and 18% (39/216) in the control group. The fixed risk difference is 0.09, 95% CI (0.02 - 0.16) and the number needed to treat is 11, 95% CI (6 - 50). Overall pregnancy rate per couple randomized (during treatment and up to > 3 months post-treatment follow-up): Pooling the results from the five trials showed a favorable but non-significant difference in the overall pregnancy rate per couple randomized (during treatment and up to 3 months post-treatment follow-up) in the FSH treatment group; OR 1.52, 95% CI (0.99 - 2.33) with a 34.3% pregnancy rate (72/210) in the FSH group and 26.9% (58/216) in the control group. Pregnancy rate after IUI/IVF/ICSI per couple randomized: There was a favorable but non-significant difference in the pregnancy rate after IUI/IVF/ICSI cycles either during the treatment period (OR 1.13, 95% CI 0.62 - 2.06), or during treatment and 3 months follow-up period (OR 1.16, 95% CI 0.65 - 2.09). When the follow-up period was extended to more than 3 months post-treatment the still non-significant difference was in favor of the control group (OR 0.94, 95% CI 0.59 - 1.49) (Figure 1). Spontaneous pregnancy rate per couple randomized: There was a favorable and significant difference in the spontaneous pregnancy rates in favor of the treatment group. During the treatment period the OR was 4.16, 95% CI 1.45 - 11.88 with a fixed risk difference of 0.05, 95% CI 0.01 - 0.09 and a number needed to treat of 20, 95% CI 11 - 100. When the follow-up period was extended to 3 months after treatment the spontaneous pregnancy rate was still significantly higher in the treatment group than in the control group with an OR of 3.87, 95% CI 1.72 - 8.69 with a fixed risk difference of 0.08, 95% CI 0.03 - 0.13 and a number needed to treat of 13, 95% CI 8 - 33. Extending the follow-up period to more than 3 months post-treatment resulted in, still, a significant difference in favor of treatment group with OR of 3.99, 95% CI 1.80 - 8.82 with a fixed risk difference of 0.09, 95% CI 0.04 - 0.14 and a number needed to treat of 11, 95% CI 7 – 25 (Figure 1). Miscarriage rate per pregnancy None of the trials reported this outcome. Adverse effects Only one case developed temporary side effect in the form of breast tenderness and mild gynecomastia that resolved spontaneously during the treatment period (20). DISCUSSION Patients suffering idiopathic male subfertility are often treated with a variety of empirical treatments. One of the most commonly used treatments is human gonadotrophins. Most of the research addressing this topic has focused on the effects of gonadotrophins on semen parameters such as motility, number, and morphology. However, it is necessary to direct research to patient oriented outcomes such as clinical pregnancy rate or live birth rate rather than on surrogate outcomes as semen parameters. To evaluate patient oriented outcomes properly conducted RCTs of adequate sample size and appropriate follow up are required. Unfortunately, the present systematic review identified five RCTs that addressed the pregnancy rate after gonadotrophin therapy for idiopathic male subfertility (including 426 participants) but none of them was of adequate sample size. Although pooling of different included studies showed positive outcomes in terms of pregnancy rate after gonadotrophin administration the collective sample size was not sufficient to achieve adequate power. The addition of the quasi randomized trial (11) supported the finding of the other five studies; gonadotrophins seem to be beneficial in achieving higher pregnancy rates. The included studies used different types of gonadotrophins (hCG, HMG, purified and highly purified FSH, and recombinant hFSH) in different regimens and doses, and some of them used IUI, IVF or ICSI. This represents an obvious clinical heterogeneity. Subgroup analysis was performed according to whether pregnancy was achieved spontaneously or by assisted reproductive techniques, however it was difficult to perform subgroup analysis according to the type of ART whether IUI, IVF or ICSI. Interestingly, spontaneous pregnancy rate showed the same positive effects of gonadotrophins, but the subgroup analysis of those using ART failed to show significant difference. This could be attributed to the impact of the technology of ART in overcoming many barriers to natural conception as reduced sperm count or motility (effect-modifying factor). Clinical heterogeneity could have been reduced if data of participants' criteria were stratified and available for each infertility diagnostic category. In the absence of these data, the conclusions may be less generalizable, although all trials except one demonstrated a treatment effect in the same direction. REVIEWERS' CONCLUSIONS Implications for practice The number of trials and participants is not enough to draw strong conclusions. However, analysis of the five included trials showed that in men with idiopathic subfertility treated with FSH there is a significant increase in the overall and spontaneous pregnancy rates per couple. This increased pregnancy rate is evident during the treatment period and within three months post-treatment. This increase is not significant in couples who undergo assisted conception. Implications for research A large multimember study with adequate power is needed to allow drawing final conclusions. Potential conflict of interest None known REFERENCES
Copyright © Middle East Fertility Society The following images related to this document are available:Photo images[mf07015f1.jpg] |
| |||||||||

{kind=link}