 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Middle East Fertility Society Journal, Vol. 12, No. 2, 2007, pp. 104-109 Rectal versus vaginal bromocriptine mesylate suppositories in hyperprolactinemic patients: an active comparator trial Atef M. Darwish, M.D.*Ehsan Hafez, Ph.D.†Ibraheem El-Gebali, PhD†,Sahar B. Hassan, MSc†,Mohammad E. Ali‡ Departments of OB/GYN and Andrology, Faculty of Medicine and Department of Pharmaceutics, Faculty of Pharmacy, Assiut University, Assiut, Egypt * OB/GYN dept., Faculty of Medicine, Assiut University. Correspondence: Prof. Atef Darwish, Women’s Health Hospital, Department of Ob/Gyn, P.O. Box: 1, 71516 Assiut, Egypt, Fax: (88)333327, e-mail: a_darwish@mailcity.com Received on November 15, 2006; revised and accepted on April 15, 2007 Code Number: mf07018 ABSTRACT Objectives: to compare the clinical effectiveness,
side effects and tolerability of rectal versus vaginal bromocreptine/pluronic
F-127suppositories as compared to oral bromocriptine tablets for treating
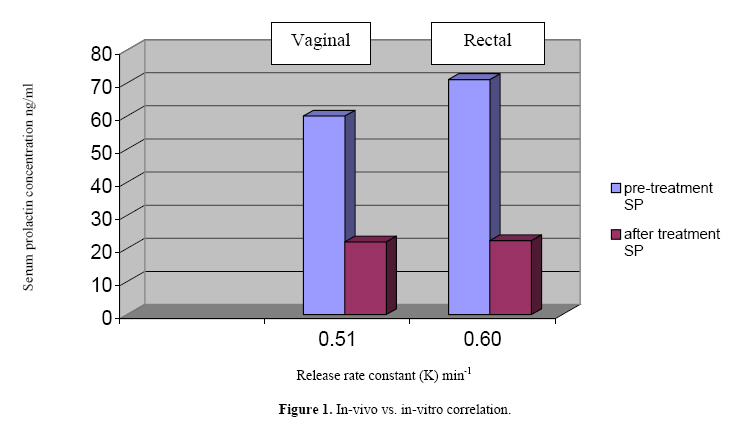
pathologic hyperprolactinemia. Key words: Bromocriptine, pluronics, oral, rectal, vaginal. Hyperprolactinemia represents a real challenge for the gynecologists, endocrinologists, andrologists, and neurosurgeons. Symptoms of hyperprolactinemia include signs of gonadal dysfunction, and female patients frequently present with oligomenorrhea, amenorrhea and galactorrhea (1). Pathological hyperprolactinemia is also associated with infertility (1) and reduced libido (2) and an increased risk of long-term complications including osteopenia and osteoporosis (3-5). These long-term complications associated with elevated prolactin levels suggest that even patients who are unconcerned by their clinical symptoms or who do not wish to receive therapy in order to restore fertility should be considered for long-term therapeutic intervention (6). Bromocriptine mesylate, a dopamine agonist, is a derivative of lysergic acid that binds to dopamine receptors and is therefore a useful tool in the treatment of many prolactin-dependent disorders. Due to its numerous adverse effects, vaginal approach had been successfully used in intolerant cases (7). As it is a poorly water soluble drug, we introduced a new formulation by mixing it with a pluronic F127 that resulted in increased dissolution rate of the drug by 39-fold than the pure drug alone (8). However, local side effects and inconvenience were encountered with this new formula in 11(55%) and 3(15%) of cases respectively. Based on these data, it was assumed that vaginal approach would not be a suitable alternative to oral route in all cases. Rectal route is a well documented effective and rapid approach used for many of medications since a long time. Comparison of the rectal and the vaginal administration of the commercial bromocriptine tablets are not published so far. Rectal and vaginal lisuride hydrogen maleates were equally effective in lowering SP if compared with oral administration in a pilot study (9). The aim of this study is to compare the clinical effectiveness, tolerability, and side effects of rectal versus vaginal bromocriptine/pluronic F-127 suppositories as compared to oral bromocriptine mesylate in hyperprolactinemic patients. MATERIALS AND METHODS This study has two phases. A pharmaceutical phase which was carried out at the department of Pharmaceutics, Faculty of Pharmacy, Assiut University between May, 2003 and June 2005. This phase included preparation of vaginal and rectal suppositories by incorporating bromocriptine mesylate solid dispersion with pluronic F127 in a ratio of (1:7) in water soluble base composed of polyethylene glycol 20000 and propylene glycol (20:80) using a fusion method under ultraclean laboratory conditions. Suppositories were cone shaped, 1 gram in weight, 20 mm in length, and 424 mm3 in size. The detailed steps of creation were previously published (8). The row material of bromocriptine mesylate was kindly supplied by Novartis Pharma Co., Cairo, Egypt. The clinical phase was conducted at the out-patient Infertility clinic of Assiut University hospital from February 2004 to August 2005 and included 69 female patients with pathologic hyperprolactinemia who were randomly divided into 3 groups regardless the possible cause of this pathologic hyperprolactinemia. A basic inclusion criterion was non-use of any prolactin-normalizing drug before entering this study for at least 1 month. Group A comprised 22 patients who used rectal suppositories once daily for one month. Group B included 20 patients who used vaginal suppositories once daily for one month. Group C comprised 27 patients who received 2.5 mg bromocriptine tablets twice daily for one month. Three males with proved hyperprolactinemia were recruited from the Andrology out-patient clinic who received rectal suppositories once daily for one month. SP was measured before and after therapy in all cases. This study was approved by the Institutional Review Board (IRB) of the Faculty of Medicine. All patients gave a written consent to participate in it. All study patients had high pretreatment baseline SP and were advised to take the drug regularly in a fixed time. All female patients were instructed to minimize touching the nipples and to avoid eating various fowl which contain prolactin releasing factors during the course of therapy (10). After one month of therapy, the patient was instructed to come 12-24 hours following the last insertion of the drug to be subjected to venepuncture for the estimation of serum prolactin using ELISA method (DIMA, Germany ELISA kits). At the end of the course of treatment, the patient was asked to assess her experience with this approach of therapy. Data were collected and analyzed with SSPS version 11 and expressed as mean ±SD. Student t-test was used to determine significance between two groups, while ANOVA test was used for all groups. RESULTS The pharmaceutical phase revealed that the release pattern of the rectal suppository of bromocriptine mesylate in phosphate buffer pH(7.4) was similar t o that of the same formula in citrate buffer (pH 4) which was formulated previously for vaginal use, their release rate constants were 0.60 min-1 and 0.51 min-1 respectively (Figure 1). The clinical part of the study comprised 69 female patients with definite high pretreatment SP levels. Demographic data are shown in Table 1. The pre-treatment clinical situation of all patients is shown in table 2. The main side effects and the clinical data are shown in table 3. Pretreatment SP was high and showed marked decline after one month of treatment in all groups as shown in table 4. The 3 males had high pretreatment SP (74,52,39 ng/ml)that showed an evident decline on rectal treatment (21,15,10 ng/ml respectively). Their results were not included in statistical analysis of this study. DISCUSSION Bromocriptine methylate, as a dopamine agonist, is being used for treatment of hyperporlactinemia since a long time. It is proved to be effective in causing dramatic decline of SP after its oral use. However, it frequently causes Table 1. Demographic data of patients in all groups
Table 2. Indication of study inclusion in all groups.
adverse side effects if given orally like nausea, vomiting, fatigue, headaches, dizziness, and faintness in 50-70% of women (11). Non-oral approach may eliminate most of these symptoms (7). Advantages of vaginal route over oral use are well established in many studies (7,8,11). The non-oral routes of administration of drugs avoid destruction or inactivation by the pH or enzymatic activity of the stomach or intestine, eliminate stomach irritation, and omit drug destruction by portal circulation by first pass through the liver. Moreover, these routes are convenient for patients who may be unable or unwilling to swallow medication and it is an effective route in the treatment of patients with vomiting episodes. For systemic effects, the mucous membranes of the rectum and the vagina permit the absorption of many soluble drugs. Although the rectum is used frequently as the site for the systemic absorption of the drugs, the vagina is less frequently used for this purpose (12). In this study, we prescribed therapeutic doses of bromocriptine methylate for the three groups as previously described. The optimal therapeutic oral dose is usually 5 mg/day because the half-life after oral administration is 3 to 7 hours (11). On the other side, 2.5 mg daily dose was sufficient with the vaginal use as the vagina allows slow absorption of the drug and hence SP level remains elevated longer with the vaginal approach. There is no sufficient data about the half-life after insertion of rectal bromocriptine suppositories. Serum levels of bromocriptine after oral, vaginal and rectal administration were estimated at our institution and will be published later on. Many studies have attempted to compare the efficacy of drugs administered rectally versus orally. For example, diazepam and propranolol have been shown to exhibit greater bioavailability when administered rectally (13). This may be due to that the drugs absorbed rectally carried by the inferior or middle veins which drain the rectum go directly into the systemic circulation, the rectal cavity is also drained by extensive lymphatic circulation which facilitates absorption and systemic exposure of absorbed drugs (14). Table 3. Clinical follow-up of patients in all groups.
* More than one item was reported in the same patient. Table 4. Serum prolactin (SP) before and after treatment in all groups.
Several investigations revealed that many drugs showed higher effect when used vaginally or rectally than when used orally such as leuprolide, indomethacin and misoprostol (15-17). In this study, the in-vitro in-vivo correlation can be explained by the presence of the non-ionic surfactant pluronic F127 which increases drug solubility and enhance drug penetration through the rectal or vaginal mucosa. It is assumed that rectal absorption is better than vaginal absorption as vaginal epithelium is formed of five layers (18), while rectal mucosa is formed of only one layer of columnar absorptive cells (19). However, in this study, the rectal route was proved to be as effective as vaginal approach in terms of SP decline after one month of therapy. The in-vitro part of this study showed similar release rate of the drug in media like the vaginal and the rectal environments. The exact estimation of drug absorption after both approaches will be published by our institution in a coming study using photochromotography. This pilot study tested the same formulation of bromocriptine mesylate in two groups of hyperprolactinemic patients who were similar as regards age, parity and gravidity. Most of the study patients were intolerant to oral route constituting good candidates for testing the tolerability of the drug via alternative approaches. However, to test the efficacy in term of lowering SP levels, we included patients with pituitary micro or macroadenoma(s) as proved by MRI or CT and patients with persistently high SP despite prolonged oral treatment. Efficacy was evaluated by comparing pretreatment and post-treatment SP. We decided not to rely on measurement of bromocriptine in serum as its absorption after vaginal approach is already proved to achieve a significant reduction of serum bromocriptine starting 7 hours after vaginal administration (20). Furthermore, it adds unnecessary costs for a research in a developing country. The best parameter of the efficacy of a prolactin-normalizing drug is to measure the level of SP. The duration of therapy in this study was just one month as it was noticed before that SP levels started to be within normal range after about twenty days of use of the drug (21). However, longer duration of bromocriptine/pluronic F-127 suppositories would make this work more valuable which is planned for in a phase III large sample sized clinical trial. Inclusion of 3 males with high SP level and achievement of marked reduction of SP highlight the tolerability and efficacy in males with minimal systemic adverse effects. Pluronics are widely used solubilizing agents and work essentially by the formation of micelles. They show thermo-reversible gelatin behavior. The dissolution rate of bromocriptine mesylate, which is poorly water soluble drug, was improved 39-fold greater than that of the pure drug in a previous study (8). From this study, it is concluded that the approached bromocriptine suppositories containing pluronic F-127 were proved to be effective in lowering SP whether used vaginally or rectally. Rectal approach has minimal side effects, more convenient for patients who don’t accept to manipulate the vagina especially virgins, others fail to use the drug during menstruation, postpartum or postabortive, and those patients who believe that the drug may affect their fertility by interfering with sexual relationship. Furthermore, it can be used by intolerant hyperprolactinemic males. . Its use as an alternative non-oral approach should be considered during counseling of patients in the formerly mentioned situations. We recommend a large sample-sized, better to be multicenter, clinical trial to define the exact role of this alternative approach in clinical practice. REFERENCES
Copyright © Middle East Fertility Society The following images related to this document are available:Photo images[mf07018f1.jpg] |
| |||||||||

{kind=link}