 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Middle East Fertility Society Journal, Vol. 12, No. 2, 2007, pp. 133-139 Comparison of laparoscopic drilling by diathermy and laser for ovulation induction in clomiphene citrate-resistant women with polycystic ovary syndrome Abbas Aflatoonian, M.D.*,Maryam Asgharnia, M.D.† ,Naeimeh Tayebi, M.D.‡ Clinical and Research Center for Infertility, Shahid Sadoughi University, Yazd, Iran *Professor of obstetric & gynecology, Clinical and Research Center for Infertility, Shahid Sadoughi University, Yazd, Iran. Correspondence: Bouali Ave, Safaeyeh, Yazd, Iran Email: Abbas_aflatoonian@yahoo.com Received on December 16, 2006; revised and accepted on April 15, 2007 Code Number: mf07023 ABSTRACT Objective: The aim of the present study was to
compare the effectiveness of laparoscopic ovarian drilling (LOD) with monopolar
diathermy and CO2 laser on the serum levels of hormone and pregnancy outcome in
clomiphene citrate (CC) resistant infertile women with polycystic ovarian
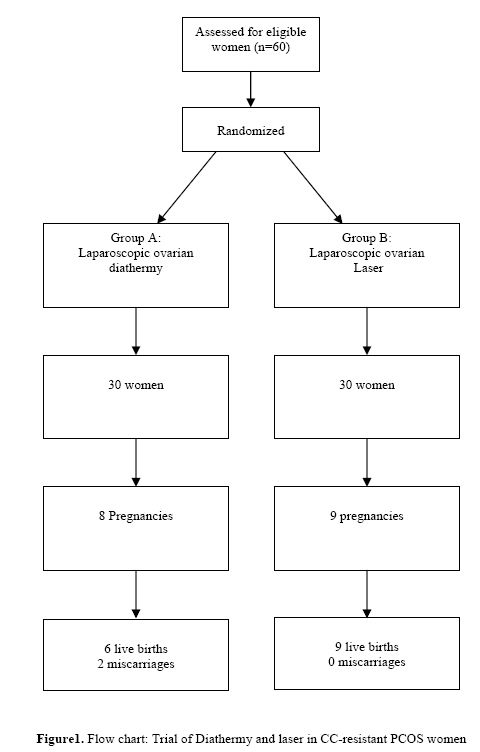
syndrome (PCOS). Polycystic ovarian syndrome (PCOS) is one of the most common endocrine disorders in women of reproductive age. The prevalence of this syndrome is approximately 6% of women in their reproductive years. Infertility due to ovulatory dysfunction is a common problem for women with PCOS (1). Clinical signs of this syndrome are menstrual disorder, oligo-ovulation or anovulation, hirsutism, acne, and in severe cases alopecia. Obesity is common in this syndrome but it is not universal (2). Although the primary defect in PCOS remains unclear, a genetic factor is suspected to play a role in the etiology of the disease (3). The optimal management of PCOS is uncertain, but treatment focuses on amelioration of the chemical features. For the most part, treatment aims to restore ovulatory cycles so that pregnancy can be achieved. The first line treatment for PCOS related anovulatory infertility is clomiphene citrate (CC) (4). The ovulation rate with this drug is more than 80 % (5). However, 15% to 20% of women remain anovulatory despite treatment with incremental doses of CC, and pregnancy rates are disappointing (33% to 40%). In addition, the miscarriage rate is high (30% to 40%) (6). Because of its anti-estrogenic effects, an increasing dosage of CC will lead to thickening of the cervical mucus and failure of endometrial development. Therefore, women resistant to CC medication will usually be treated with exogenous gonadotrophins. As a result, another treatment for PCOS is gonadotropins or pulsatile Gonadotrophin-releasing hormone (GnRH). In fact, Gonadotrophins are more effective than GnRH (7), but they have a higher risk of serious side effects, such as multiple pregnancy and the ovarian hyperstimulation syndrome (OHSS); while GnRH therapy is effective with lower risk of these side effects (8, 9). It has now been recognized that laparoscopic ovarian drilling (LOD) is an effective second-line treatment for CC-resistant anovulatory infertility associated with PCOS (10). Grzechocinska et al (2000) assessed the results of CC ovarian stimulation vs. Laparoscopic diathermy of the ovaries in infertile women with PCOS. Results showed that the ovulation rate was 68% vs. 90.9% and the pregnancy rate was 28% vs. 63.3% respectively. Therefore, it seems that much more successful results could be achieved by LOD in comparison with stimulation of the ovaries with CC in PCOS women (11). Kriplani et al (2001) applied LOD using monopolar diathermy on seventy women with CC resistant PCOS and followed up them for 4.5 years. Their results showed that ovulation and pregnancy rates were 81.8% and 54.5% respectively, which means that LOD is an effective surgical procedure in women with CC resistant PCOS (12). With laparoscopic surgery, the possibility of inducing ovulation by LOD was raised. The other advantages of LOD are decreasing the risk of OHSS and multiple pregnancies and occurrence of consecutive ovulations without the need for further treatment; while the disadvantages are the need for a surgical procedure and creation of tubo-ovarian adhesions (13). The aim of this study was to compare resumption of menstrual regularity, biochemical changes, ovulation, pregnancy and miscarriage rates in women who had CC-resistant PCOS and were treated by laparoscopic drilling by diathermy or laser for ovulation induction. MATERIALS AND METHODS A randomized controlled trial was conducted to compare the success rate of two different surgery methods, namely laparoscopic ovarian diathermy and laparoscopic ovarian CO2 laser vaporization in the treatment of PCOS. Written informed consent was obtained from all patients and has been written in paper. Also, Ethical committee of Yazd Shahid Sadughi University of Medical Science approved this study (figure 1). In total, 60 women who attended at Yazd Clinical and Research Center for Infertility were diagnosed with PCOS between August 2004 and September 2005. The inclusion criteria for this study were as follows: 20 to 38 years of age, CC resistance (no ovulation after three cycles of up to 150 mg of CC from day 5 to day 9 of menstrual each month), infertility of more than 12 months duration, a body mass index(BMI) of less than 35kg/m2, and typical findings on sonography, such as ovarian stromal hypertrophy and multiple (≥10), small (6-8mm) follicles arranged in the periphery of the ovary (14). All the women’ husbands had normal semen analysis (>20 million per milliliter, >30% normal forms, and >50% motility) (15). The other inclusion criteria were early follicular phase (defined as days 2-5 of the menstrual cycle) serum LH/FSH ratio more than 2 and /or raised serum androgen levels (testosterone≥2.5nmol/l) and oligo or amenorrhea. The exclusion criteria were included other endocrinological abnormalities such as hyperprolactinaemia, and thyroid dysfunction, Women with tubal disease diagnosed by laparoscopy and partners with male factor. Randomization was performed using computer-generated sequences that were sealed in number opaque envelopes. Ovarian diathermy or laser surgery was performed by one expert surgeon as follows; the procedure was undertaken in the operating theater under general anesthesia. Routine pneumoperitoneum was achieved using a Verres needle (Karl Storz, 30675ND, Germany), and the laparoscope (Olympus, JAP AN) was introduced at Table1. The characteristics of 60 women who underwent laparoscopic ovarian diathermy (groupA=diathermy, groupB=laser) for anovulatory infertility due to polycystic ovarian syndrome. Values are given as mean ±SD and number of observations as n (%). The results of hormonal levels shown are those obtained before the operation. T test and Chi-Square was used for statistical analysis.
the umbilicus. Two ports were used; one at the suprapubic level and one in the left iliac fossa, both 5 mm. Under laparoscopic control, each ovarian pedicle was grasped using an atraumatic forceps. The pelvic organs were inspected and tubal assessment was confirmed by transcervical injection of methylene-blue dye. The ovary was lifted up and sited to the anterior wall of the uterus away from bowel. In group A, a monopolar electrocautry needle of 0.5 cm in length was used to drill 6 holes with the depth of 5 mm in each ovary. The diathermy was done with cutting power at 30 watt and was continued for 6 seconds; while in group B, Laser therapy was performed with CO2 laser, with the power setting at 30 Watt and 15 punctures with superficial penetration were made in each ovary and this power was continued for 6 seconds. At the end of the procedure, to avoid adhesion formation, extensive pelvic lavage was performed with 250ml of Ringer Lactate’s solution. At hospital discharge, the women in both groups were not treated with any drugs for 1 year. Following ovarian laparoscopic diathermy or laser, women were asked to keep a record of their menstrual cycle. A blood sample was taken on day 21 after the first spontaneous menstruation for measurement of serum concentration of LH (mIu/ml), FSH (mIu/ml), Progesterone (ng/ml) and Testosterone (nmol/l) level. The following outcome measures were collected and reported for 1 year. Ovulation rates were determined by progesterone levels of more than 10 ng/ml in the luteal phase (timed 21 days after the first spontaneous menstruation) for both groups. Pregnancy outcomes included serum B-HCG of more than 50 IU/L, and fetal heart activity on abdominal ultrasound scan, after 8 weeks of gestation. SSPS version 13 was used to do the appropriate statistical tests including Student's T Test, Chi-square and Fisher exact test. The results are expressed as means and standard deviation. Differences were considered to be statistically significant if p-value was <0.05. RESULTS The main demographic, clinical and endocrinological characteristicsin groupAandB are shown in Table 1.Our results showed that the women suffered mainly from primary infertility. Only in 11 cases (6 in group A and 5 in group B) secondary infertility was diagnosed. Mean duration of infertility was more than 5 years in both groups. The mean age of women and BMI in both groups was similar. Their hormonal profiles before treatment did not differ concerning LH, FSH, LH/FSH ratio and Testosterone concentrations. Also, the rates of acne and hirsutism (Ferriman Gallwey score>8) was similar in both groups. The percentage of women with PCOS resumed regular menstrual cycles after surgery were 22 women (73%) in group A and 23 women (76%) in group B (P-value=0.5). Table2. The impact of laparoscopic ovarian drilling on hormonal levels (after surgery) in women with polycystic ovarian syndrome. Values are given as mean ±SD. T test was used for statistical analysis.
Table 2 showed the impact of LOD on hormonal levels in women with PCOS. There was no significant difference in LH, FSH, LH/FSH ratio, Testosterone and Progesterone on 21st day of the first menstrual cycle between two groups. The mean progesterone on 21st day of cycle was more than 12ng/ml in both groups. The treatment results of laparoscopic ovarian by diathermy and laser were similar (See Table 3). After treatment and 1 year follow up, in the group A (women with diathermy) ovulation occurred in 12 out of 30 women (40%) and pregnancy in 8 out of the 30 women (26.7% ); accordingly in the group B (women with laser) ovulation occurred in 13 out of 30 women (43.3%) and pregnancy in 9 out of 30 women (30% ). Two of the eight pregnancies in group A and none of them in group B ended with miscarriage at 8 weeks of gestational age. The live birth rate was not significantly different between the groups (P-value=0.2). Finally, there were no multiple pregnancies in any groups and all of the live births were singleton. Table3. The outcome of pregnancy of the 60 women with polycystic ovarian syndrome after laparoscopic ovarian drilling in both groups. Fisher exact test was used for statistical analysis.
DISCUSSION Anovulation in PCO patients can be treated medically in some cases with antiestrogen. Gonadotrophin therapy may be more successful, but there is a significant risk of OHSS and multiple pregnancies (16). In addition, therapy with Luteinizing hormone-releasing hormone (LHRH) has been used but the results have been disappointing and the miscarriage rate has also been high (17). More recently LOD is known to be a successful form of treatment in resistant cases of PCOS (18, 19). In the present study, two laparoscopic techniques (diathermy and laser) for the treatment of PCOS have been compared with each other. In general, there are four laser systems (CO2, Nd-YAG, argon, KTP) for surgery, but in this study only CO2 was used for laparoscopic ovarian laser. Our results have demonstrated that the total ovulation rate was not statistically different between both treatment groups (40% vs. 43.3% in group A and B respectively); in addition, the pregnancy (26.7% vs.30%), the miscarriage (6.6% vs.0%) and the live birth (20% vs.30%) rates were not significantly different between two groups. Similarly, Saleh (2004) found that there was no statistically significant difference in the ovulation rate following LOD with diathermy and laser in anovulatory infertile women with PCOS (83% vs.77.5%); while there was a significantly higher cumulative pregnancy rate at 12 months after diathermy surgery (65% vs. 54.5%). He concluded that LOD with diathermy is superior to laser drilling and gonadotrophin therapy (20). Amer et al (2002) investigated long term follow-up of PCOS women after LOD. They showed the proportion of women with regular menstrual cycles increased from 8% before LOD to 67% post-operatively, but there was no comparison between diathermy and laser therapy in their report (21). In our study, the proportions of women with regular menstrual cycles increased from 6.7% before diathermy to 73% after that and from 3.4% before laser therapy to 76% post operatively. There was no significant difference in regular menstrual cycle between laparoscopic ovarian diathermy and laser (73% vs. 76%) (P-value=0.5), but a significant difference was in regular menstrual cycle before and after LOD in both groups (P-value=0.012). Api et al (2005) showed the serum levels of Testosterone, LH, FSH, and LH/FSH ratio were significantly reduced after LOD (22). In the present study, serum levels of Testosterone, LH, FSH, and LH/FSH ratio between laparoscopic ovarian diathermy and laser have been compared. There was no significant statistical difference between these values before and after surgery in both groups (P-value=0.08); whereas, there was a reduction in these levels after surgery in both groups and this reduction in laser group was more than this reduction in diathermy group. There were no multiple pregnancies in any groups of LOD in the present study. Similarly, According to the other studies, multiple pregnancy rates are reduced in those women who conceive following Laparoscopic drilling compared with this rate in gonadotrophin study (23-26). Initially, Keckstein et al (1989) reported that no clear advantages have so far been shown to exist for any of the available techniques, i.e. laparoscopic diathermy and laser therapy, but it appears, however, that the laser techniques will be the methods of choice for the future (27). CONCLUSION The present study confirms that LOD is the method of choice in the treatment of CC resistance PCOS women, but there is no difference between diathermy and laser. ACKNOWLEDGMENT This research was granted by Clinical and Research Center for Infertility, Shahid sadoughi University, Yazd, Iran. The authors express their thanks to Dr Mohammad Hassan Sheikhha (The Editor of IJRM) for editing and MS Habibeh Gheisari and Leila Motamedzadeh for cooperation in laboratory. REFERENCES
Copyright © Middle East Fertility Society The following images related to this document are available:Photo images[mf07023f1.jpg] |
| |||||||||

{kind=link}