 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Middle East Fertility Society Journal, Vol. 13, No. 1, 2008, pp. 11-15 OPINION Luteal phase support in assisted reproduction: United Kingdom survey Ahmed S. Kassab, M.R.C.O.G.*, Gehan El-Bialy, M.D.†, H.Hashesh, M.D.‡, Santanu Baruah, M.D.*, Talha Al-Shawaf, F.R.C.O.G.* Centre for Reproductive Medicine, St
Bartholomew’s Hospital, London; Department of Obstetrics and Gynecology Royal
Devon and Exeter Hospital and Department of maxillofacial surgery North Staffordshire University Hospital U.K. Code Number: mf08002 ABSTRACT Objective: Probing practices of luteal phase
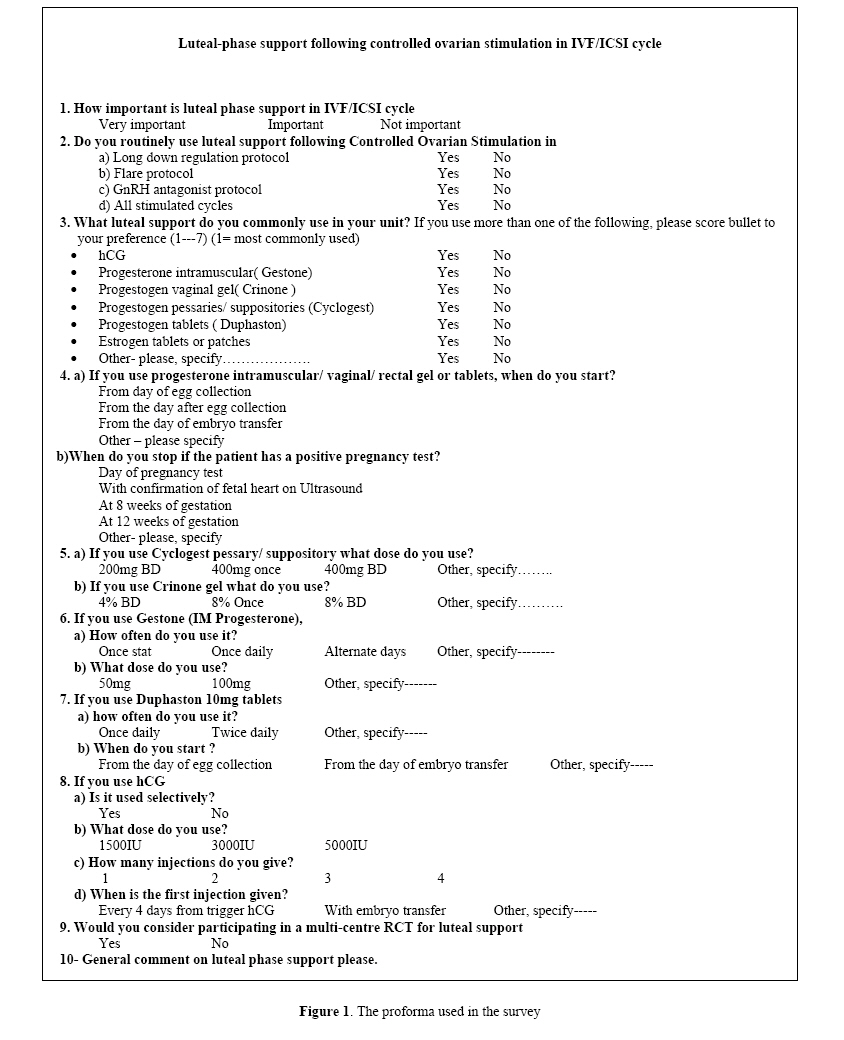
support in assisted reproductive technology (ART) centers in U.K. Key words: ART, hCG, Luteal support, Progesterone, Survey. During luteal phase of IVF cycles it might be expected that controlled ovarian hyperstimulation (COH) with exogenous gonadotropins yields multiple corpora lutea that might sustain supraphysiologic serum concentrations of estradiol and progesterone. However co-treatment with gonadotrophin-releasing hormone (GnRH) analogs for prevention of premature Latinizing hormone (LH) surges, leads to abnormal low levels of LH during the luteal phase which is insufficient to stimulate and maintain the level of luteal function required to promote timely endometrial maturation in preparation for implantation or to support an early pregnancy. This suppression could last up to 10 days after treatment with long-acting GnRH agonist ends (1). Although the GnRH antagonists have a much shorter half life and a reduced time of application, they often have the same effect (2). In an attempt to compensate for this abnormality, many reproductive centers are in use of luteal support with either single or combined drugs. This preparation has consisted of hCG, progesterone and estrogen and to be used during luteal phase and beyond for patient undergoing ART cycles. Different types, regimes are used but the best dose, length or type of treatment remains controversial. MATERIALS AND METHODS All United Kingdom licensed reproductive centers were identified through HFEA (Human Fertilization Embryology Authority) registry for year 2005. The lead clinician was posted by the questionnaire. A second reminder through the post or telephone was conducted after certain period if no reply was received. The Questionnaire (Figure 1) included questions about the importance of luteal support following COH. The routine use of luteal support and if so for which protocol; long down regulation protocol, flare up protocol, or GnRH antagonist protocol. Type and route of luteal support that are in common use in the unit. This includes progesterone intramuscular (gestone), vaginal gel(crinone), pessaries/ suppositories (cyclogest), tablets (duphaston), hCG, estrogen tablets or patches or any others types. Time, dose and length of administration were included in the survey. Time ranged from day of oocyte retrieval, after oocyte retrieval or from day of embryo transfer. Length varied from the time of pregnancy test, confirmation of fetal heart on ultrasound scans, or till eight-twelve weeks gestation (Figure 1). Lastly if the centre would consider participating in a multi-centre randomized control trial (RCT) for luteal support. Outcome measures The main outcome measures were importance, optimal hormone, and optimal route, dose, length of progesterone, estrogen and hCG administration. Statistical analysis Data were statistically described in terms of frequencies (number of cases) and relative frequencies (percentages) whenever appropriate. RESULTS The survey was conducted between January 2005 and May 2005, 82 questionnaires were sent. All the centers were 100% licensed centers for IVF/DI. Of those, 69 centers perform IVF/ICSI. The overall response rate was 84% (69). Among the IVF centers response rate was 87% (60). The importance of luteal phase support was reflected in the IVF/ICSI centers by 65% (39) as very important and 30% (18) as important one. 97% used it in long down regulation protocol, 65% for flare up protocol but for GnRH antagonist protocol was 75%. The routine use of luteal support following COH with all stimulated cycles was 80%. HCG was ranked second behind progesterone. HCG total use was 38% (23). Cyclogest was the first choice of those selected a preference in 55%. 92% of IVF/ICSI centers who responded to the questionnaire use cyclogest. Gestone use was 42%, crinone vaginal gel was 25%. Duphaston tablets were far behind the scale for luteal support (9.6%). Surprisingly estrogen patches were used in 9 centers (15%). Optimum time for the start of progesterone varied from the day of oocyte retrieval (48%), day after oocyte retrieval (19.3%) and from day of embryo transfer (25.8%). Length of use for luteal support again was again variable but up to 12 weeks of gestation represented (48%), followed by up to day of pregnancy test (24.1%). The dose of cyclogest was 400mg BD as the favorable dose in (55%), but for crinone 8% gel once daily was (16.1%), followed by gestone intramuscular once daily (33.8%). HCG was used selectively in 19 centers and in 52.3%, 1500 IU was the recommended dose and to be given twice in (38%) with the first injection on the day of embryo transfer (47.6%). 53.2% of the centers consider participation in a multi-centre RCT for luteal support. DISCUSSION Recently two meta-analyses including a Cochrane review meta-analysis were published. Both confirmed the need to offer luteal support in ART which significantly increase the live birth (3,4). Progesterone and hCG were concluded to provide highest rate (3,4). But hCG for ART cycle has been found to be associated with higher risk of ovarian hyperstimulation syndrome which can be a life threatening condition (3). In spite of lack of statistical significance, the intramuscular route seemed to be more beneficial than the vaginal route when considering rates of ongoing pregnancy and live birth (3,5). Studies have revealed that vaginal progesterone has the advantage of first pass uterine effect in comparison with the oral progesterone and that was reflected in reduction in pregnancy rates are noted on oral administration (5). Chantilis et al (6). and Schoolcraft et al (7). showed comparable rates of implantation, clinical and ongoing pregnancy rates with progesterone gel and intramuscular progesterone however it showed a difference regarding the intolerability of the patient towards the intramuscular route. On the other hand the vaginal route could be complicated by perineal irritation, erythema and vaginal discharge (6,7). Our survey showed that 90% of ART centers in U.K., representing 23,500 cycle/ year majority of the lead clinician (person responsible) in those centers support the fact that luteal support is very important/ important in the field of ART. Cyclogest was the most widely used for luteal support with 55% choose it as their first choice where it is being used in the long protocol where most of the centers deploy in comparison with other types of protocols. Although there was some difference in the starting time of the use of cyclogest in the ART cycle (day of oocyte retrieval versus day of embryo transfer), the majority of the centers continue to use cyclogest once pregnancy was confirmed and up to twelve weeks gestation. The idea of extending the duration of luteal support up to twelve weeks gestation is related to the timing of luteoplacental shift where the trophoblast will take over the steroid maintenance of pregnancy (8).Ogino et al., (8) showed that there is a distinct difference before and after tenth weeks of pregnancy in regard the productivity of estrogens when the placental localization is established. Other studies involving embryo donation program noted that E2 levels increased quickly from the fifth week of pregnancy, even with the same dose of E2 supplementation indicating that the luteoplacental shift may occur earlier than the tenth week (9). On the other hand, Navot et al., (10) observed a rise in E2 during the eleventh week and progesterone during the twelve week of pregnancy (10). The usual dose prescribed was 400 mg pessaries/suppositories twice daily. The long use of cyclogest can provide some reassurance on its safety. The pessaries /suppositories can be regarded more convenient by modifying the size or shape of the delivery system. The role of E2 in the human luteal phase is still under evaluation although that in non human species the influence of the luteal phase E2 level on implantation is controversial (11). The results published by Ghosh et al. (12) and Ortiz et al. (13) did not reach a firm conclusion (12,13) but the results published by Farhi et al. (14) and Lukaszuk et al. (15) was supporting the addition of high dose of E2 to daily progesterone supplement in long agonist protocol (14,15). The importance of luteal phase support is well recognized. Our observational study highlights existence of a wide variation in practice in the UK. Progesterone preparations are the most preferred drugs. Current evidence, the clinician’s own preference, cost-effectiveness and patient choice probably contribute towards the use of progesterone preparations for luteal support. However, there is definite role of hCG under limited circumstances. This recommendation was adapted by National Institute of Clinical excellence (NICE). However NICE guidelines do not state any detail of progesterone preparation (16). So there is a need for more research to examine the type, dose, route, duration, patient acceptability, cost-effectiveness and outcome of luteal support with both progesterone and hCG preparations. REFERENCES
©Copyright 2008 - Middle East Fertility Society The following images related to this document are available:Photo images[mf08002f1.jpg] |
| |||||||||

{kind=link}