 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Middle East Fertility Society Journal, Vol. 13, No. 1, 2008, pp. 28-32 Serum-prostatic specific antigen level as a promising marker in infertile women with polycystic ovarian disease Mohamed Abdel Hammid Metawie, M.D., Taher El Sarafy, M.D., Sherif El-Kattan, M.D., Hamdy Azab, M.D., Magdy El-Biely, M.D. Department of Obstetrics and Gynecology,
Department of Biochemistry, Suez Canal University, Egypt. Received on March 11, 2007; revised and accepted on January 17, 2008 Code Number: mf08007 ABSTRACT Objective: To evaluate value of serum prostatic
specific antigen (PSA) as a marker for PCOS infertile women undergoing ovulation
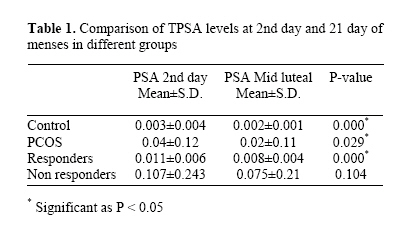
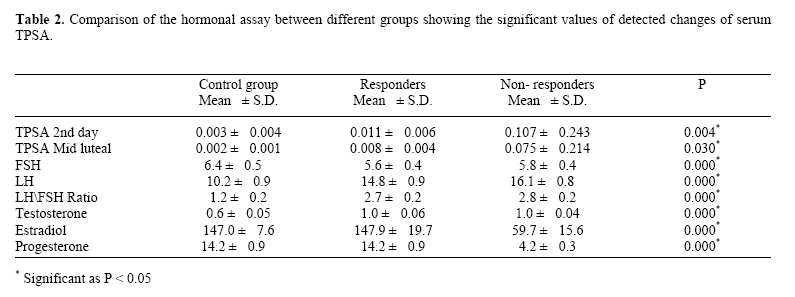
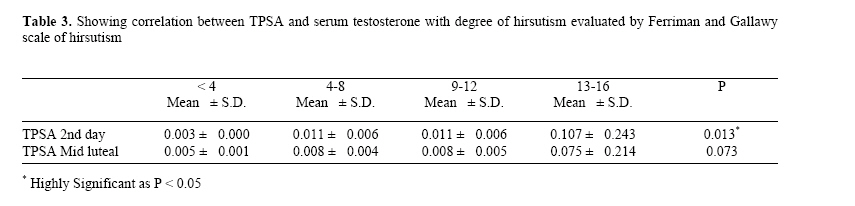
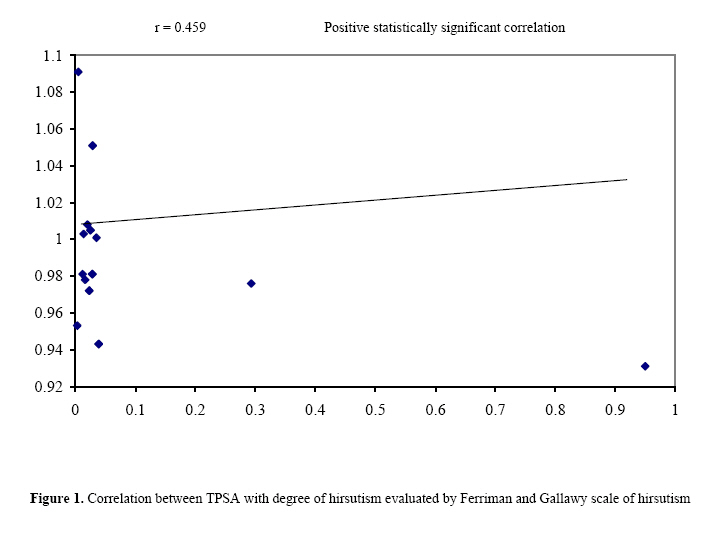
induction. Keywords: prostatic specific antigen, infertility, PCOD, Immulite Prostate-specific antigen (PSA) is a 33-kDa serine protease, the production of which was previously thought to be confined exclusively to the male prostate (1). With the development of ultrasensitive immunoassays, it was shown that TPSA was also produced by a wide variety of female tissues (1-3), mainly breast and peri-urethral glands. Elevated serum TPSA levels were noted in hirsute women (4, 5). The source which seems to be the periurethral glands, an observation that is supported by the fact that these glands in females are highly homologous to the male prostate (6,7). PCOS is an accumulation of many incompletely developed follicles in the ovaries due to a complex state of chronic anovulation with increase in ovarian androgen production (1). Based on the above considerations, we speculated that serum TPSA levels in PCOS women may be high and that the measurement of serum TPSA in these women may have some clinical implications. In this study, we measured TPSA levels in female serum with a highly sensitive TPSA assay and compared the levels between PCOS women and apparently healthy normoovulatory women. MATERIALS AND METHODS This is a prospective clinical trial conducted in the Department of Obstetrics and Gynecology, Suez University from October 2005 till December 2006. Subfertile women with PCOD entitled for induction of ovulation with clomiphene citrate and human menopausal gonadotropin were recruited for the study and compared to normoovulatory women. The study was approved by the local ethical committee. Women were included if they fulfilled Rotterdam criteria for PCOD as chronic anovulation, hirsutism, irregular bleeding, normal hysterosalpingography. We excluded women with any infertility causes rather than polycystic ovarian disease, patient on corticosteroid therapy or male cause of infertility. Subfertile women were further classified according to the serum TPSA after induction of ovulation into: Sub-group I: PCOD with low level of TPSA., Sub-group II: PCOD with high level of TPSA. All patients were subjected to throw medical history with emphasis on the menstrual rhythm. Clinical evaluation was then done with emphasis on weight, height, acne, degree of hirsutism according to clinical assessment of Ferriman and Gallawy scale of hirsutism (8) . Criteria of PCOD diagnosis by transvaginal ultrasonography: Ovarian volume >10 cm³. - 10 follicles each one is less than 10mm., hyperechogenic stroma. Laboratory assay was done for FSH, LH, Testosterone, and day 21 serum Progesterone. PSA level measured by ultrasensitive method in all cases subjected to induction of ovulation with clomiphene citrate (100 mg/day)from the second day of menses till the sixth day (measurements done at first day of menses and at mid-luteal phase). Transvaginal folliculometry was done at days 8, 10, 12, 14 respectively and human menopausal gonadotrophin had be given according to the folliculometry to reach follicular diameter of 18 -21 mm. on day 13 – 14 of the cycle. Human chorionic gonadotropin had been given at this stage. Number of follicles, number of HMG ampoules given to each group, mid-luteal Progesterone and finally the pregnancy rate were recorded. Blood sampling Five ml of blood were collected and left to clot. After centrifugation, serum was separated, aliquoted into 5 aliquots and deep-frozen at - 70 oC until analysis. Measurement of serum total prostate specific antigen by chemiluminescent immunometric assay. This was carried on the IMMULITE auto-analyzer using kit supplied by DPC (Cat N.LKPS1): Diagnostic Production Corporation. Los Angeles. Principle of the procedure It is a solid phase, two-side chemiluminescent immunometric assay. The solid phase, a polystyrene bead enclosed within an Immulite test unit is coated with monoclonal antibody specific for TPSA while the serum sample and alkaline phosphatase conjugated polyclonal antibody are incubated for approximately 30 minutes at 37oC in the test unit with intermittent agitation. TPSA in the sample is bound to form an antibody sandwich complex. Unbound complex is then removed by a centrifugal wash, after which the substrate is added and the test unit is incubated for further 10 minutes. The chemiluminescent substrate, a phosphate ester of adamantly dioxetane, undergoes hydrolysis in the presence of alkaline phosphatase to yield an unstable intermediate. The continuous production of this intermediate results in the sustained emission of light. Thus improving precision by providing a window for multiple readings. The bound complex and thus also the photon output as measured by the luminometer is proportional to the concentration of TPSA in the sample.. Expected Normal Value: 0 - 4 ng / ml. Statistical analysis Quantitative data were presented as mean ± SD for normally distributed data and as medians and percentiles for skewed data. Differences among groups were compared by the student’s t test and Table 1. Comparison of TPSA levels at 2nd day and 21 day of menses in different groups Kruskal-Wallis analysis of variance, and / or Mann Whitney test, for normally distributed and skewed data respectively. All tests were two tailed and considered statistically significant at P <0.05. The results were analyzed using the SPSS computer software, version 10.0 (Chicago, IL, USA). RESULTS Eighty four women were included in the present study in 1: 3 ratio to retrieve as much information as possible about TPSA in PCOS. Participants were divided into Group I: 20 normoovulatory as a control group and Group II: 64 with PCOS. This group was further subdivided into: Subgroup A: who responded to induction of ovulation. Subgroup B: who did not respond to induction of ovulation. PSA both on 2nd day of cycle and midluteal phase was significantly higher in PCOS than in control group and TPSA was significantly higher in those who did not respond to ovulation induction than those who responded.(Tables 1 and 2). There was also a strong correlation between TPSA and serum testosterone with degree of hirsutism evaluated by Ferriman and Gallawy scale of hirsutism as shown in Table 3 and Figure 1. DISCUSSION Prostatic specific antigen (PSA) is the most specific prostatic tumor marker in man. Recently, TPSA has been detected in a variety of tissues and fluids in women and only minor fluctuations of serum TPSA concentrations are observed in healthy pre- and post-menopausal women (1). TPSA expression was found to be under the regulation of steroid hormones, especially androgens and progestins (9). Hirsutism is common in PCOS patients, the prevalence is only about 75% (10). The goal of this study was to assess the level of TPSA in normoovulatory women and those with PCOs and to correlate it to the severity of hirsutism. We found that serum TPSA levels were increased significantly in women with PCO than those in the control group. However, reduction in TPSA was also observed after ovulation induction. This difference was statistically significant in those who responded compared to those who failed to respond. More importantly, the basal level of TPSA on 2nd day of cycle in responders was significant lower than those who did not respond (Table 1). This could be of value to predict the response to clomiphene citrate from the start. In those hirsute women with PCOS where TPSA is higher than 0.1ng/dl, it would be preferable to start with gonadotrophin injections rather than clomiphene citrate. This Advanced technology has allowed now electronic estimation of PSA with high degree of accuracy although it is still not commercial yet (11). keeping this information in mind, PSA could really be the investigation of choice before induction of ovulation. The present study is distinguished being evaluated TPSA before ovulation induction and on day 21 of cycle i.e. to estimate the response of ovulation induction. Interesting findings were obtained where TPSA was found to decreased significantly in those who responded to induction and this decrease was statistically significant than control group. Those who did not respond to induction had still higher levels of TPSA. The source of androgen excess in patients with idiopathic hirsutism is considered to be increased peripheral conversion of androstanediol and testosterone to DHT via the pivotal enzyme, 5-reductase. Although DHT is the most potent endogenous androgen, it is considered to be a poor circulating marker of androgenicity. In this study, positive correlation was found between elevated serum TPSA levels and degree of hirsutism evaluated by Ferriman and Gallawy scale of hirsutism. These findings match well with other investigators who found TPSA levels to be higher in hirsute women than in control subjects (p<0.01). The authors suggested that TPSA can be used to discriminate hyperandrogenemic hirsutism. If more sensitive assays become available, TPSA might be used as a diagnostic criteria for hirsutism and even for some diseases which have hirsutism as a component (4). However, for proper use of PSA, we recommend its use in women with OCOS associated hirsutism not idiopathic hirsutism as recent studies showed conflicting evidence for the value of antiandrogen drugs used in idiopathic hirsutism. While some investigators found them useful in lowering the PSA level (12), other showed that serum PSA level is not a convenient biochemical marker with the available assays for the management of hirsute women treated with the combination of spironolactone and oral contraceptives. (13) In conclusion, the mean serum TPSA could be detected in high significant concentrations in the serum of PCOD infertile women with significant decreasing concentrations after induction of ovulation, thus TPSA can be used as a promising marker for ovarian response in infertile women due to PCOD. REFERENCES
©Copyright 2008 - Middle East Fertility Society The following images related to this document are available:Photo images[mf08007t2.jpg] [mf08007t1.jpg] [mf08007f1.jpg] [mf08007t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}