 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Middle East Fertility Society Journal, Vol. 13, No. 1, 2008, pp. 44-51 The predictive value of pronuclear morphology screening on embryo development and pregnancy outcome in ART cycles Mohammad Ali Khalili, Ph.D.*, Vida Razavi, M.D.†, Farahnaz Mardanian, M.D.†, Navid Esfandiari, D.V.M., Ph.D., H.C.L.D.‡ Research and Clinical Center for
Infertility, Shahid Sadoughi University of Medical Sciences, Yazd, Iran; Fertility
and Infertility Research Center, Isfahan University of Medical Sciences,
Isfahan, Iran; and Division of Reproductive Sciences, Department of Obstetrics
and Gynecology, University of Toronto, Toronto, Canada. Received on June 26, 2007; revised and accepted on December 16, 2007 Code Number: mf08010 ABSTRACT Objective: To evaluate the predictive value of
zygote pronuclear (PN) morphology on embryo development and pregnancy outcome
in in-vitro fertilization (IVF) and intracytoplasmic sperm injection (ICSI)
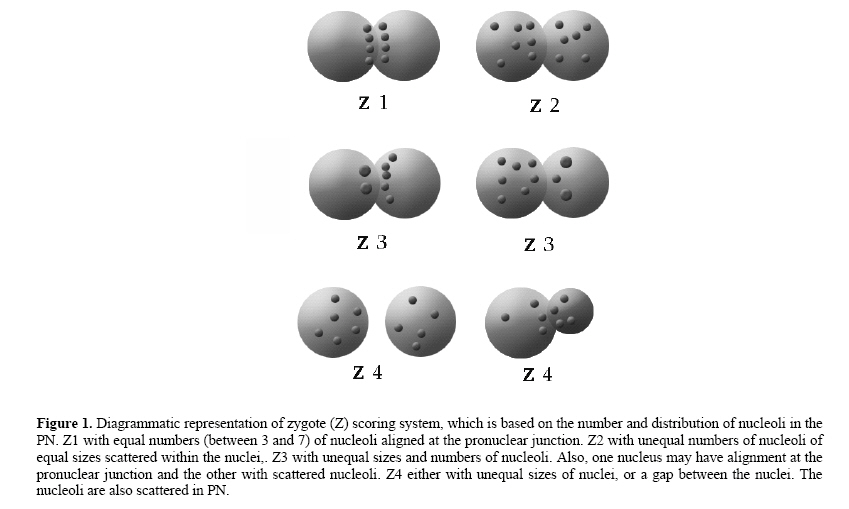
cycles. Key Words: pronuclear morphology; zygote scoring; IVF; ICSI; cleaving embryo; blastocyst. In the past two decades, a great deal of effort has been made to correlate the morphological appearance of embryos with the chance implantation and successful pregnancy. Amongst the alternative prognostic parameters that have been introduced by reproductive specialists, screening embryo’s morphology assist the embryologist in selecting the best embryos for embryo transfer (ET) (1). Morphology evaluations should be applied early in development to avoid a possible negative impact of prolonged in-vitro culture, while the extra embryos can be frozen at early developmental stage (2, 3). In recent years, there has been much research done at zygote stage. Scott and Smith were the first to establish a day-1 score encompassing PN morphology as an indicator of embryo development (4). Since, this scoring system is easy and requires a limited time, it can be adopted as a routine in ART laboratories. Z-scoring system is applied with great success to predict blastocyst formation (5), Ludwig and co-workers used this zygote scoring system and to improve the pregnancy and implantation rates. They indicated that PN pattern has prognostic value in clinical ART program (6). The analysis of PN pattern was further refined by Tesarik and Greco who focusing on the inter-pronuclear synchrony of nucleoli; which is the in terms of number and distribution (7). The effectiveness of this scoring was further supported by Balaban et al. (2001) and Chen et al. (2003) (8, 9). However, other studies did not find a correlation between PN patterns and treatment outcome in ART cycles (10, 11). It is recommended that the embryos showing an ideal PN pattern should be selected for transfer (12, 13). Moreover, abnormal patterns of PN morphology are correlated with a higher rate of cleavage arrest, as well as lower blastocyst development (8). Current studies have found that zygotes with different PN sizes present a significantly higher incidence of both embryo cleavage arrest and mosaicism in day-3 embryos (9). Since, both embryo chromosomal status and PN patterns seem to be related to embryo cleavage ability, a link may exist between the PN score and embryo chromosome constitution (14). The objective of this study was to evaluate the predictive value of zygote pronuclear scoring with quality of cleaving embryos as well as blastocyst development and pregnancy outcomes in IVF and ICSI cycles. MATERIALS AND METHODS Patient Selection A prospective study was conducted on patients undergoing infertility treatment from Sep 2005 to Dec 2006. The morphology of each zygote PN from IVF (n=35) and ICSI (n=35) cycles were evaluated and compared. The cycles that did not reach the embryo transfer were excluded. The cause of infertility for IVF and ICSI patients were tubal and male factor of infertility, respectively. Controlled ovarian stimulation was carried out with human menopausal gonadotrophin (hMG, Pergonal; Serono, Swiss) or recombinant FSH (Gonal F; Serono, Swiss). Follicular growth was monitored with serial ultrasounds and serum estradiol levels. When the diameter of two lead follicles exceeded 18mm, 10,000 IU human chorionic gonadotropin (hCG, Pregnyl, Organon, Germany) was given s.c. Transvaginal ultrasound-guided oocyte retrieval was performed 36 h after hCG administration. This study was approved by our University ethics committee. Semen Analysis and Sperm Preparation Semen analysis was performed according to WHO guidelines (15). A 5µL aliquot of liquefied semen was loaded on a microcell counting chamber (Conception Tech, CA, USA) and examined under 200x magnification. Sperm concentration was expressed as x106 /mL semen, while motility was expressed as a percentage. Geimsa staining was used for evaluating sperm morphology. Sperm was prepared with two-step density gradient technique. Briefly, 1ml of liquefied semen was layered on top of 1ml of 45% and 1ml of 90% pure sperm (Nidacon Co; Switzerland), and centrifuged once (2,000 rpm for 20 min). After pellet collection, 3 ml of Ham’s F10 medium (Medicult Co., Denmark) was added and the sample was centrifuged twice (2,000 rpm for 10 and 5 min, respectively). Following supernatant removal, 0.2-0.5 ml of the culture medium was added, and suspension was then incubated at 37C in 5% Co2 until use (1). In vitro fertilization For the ICSI procedure, oocyte denuding was performed 2-4 hrs following retrieval. The cumulus–corona removal was performed using 80-mIU/ml hyaluronidase (Sigma chemical Co., St Louis, MO) in HTF supplemented with 0.5% human serum albumin (HSA) for 30-45 seconds. The oocytes were then washed in three consecutive washes of 37°C HTF/SSS. ICSI was then performed as described earlier (1, 16). For IVF, 3 to 4 oocytes were placed in the center well culture dish (Becton Dickinson, Franklin lakes, NJ), and 50-100,000 motile washed sperm per oocyte was added to the dish. Pronuclear Evaluation Approximately 18 hrs after injection or insemination, oocytes were checked for signs of fertilization (two distinct PN and two polar bodies) and the morphological feature of PN of each zygote was evaluated (Figure 1). Each zygote was placed in individual 10 µl drops of medium (Medicult, Denmark) under mineral oil. They were then scored on an inverted microscope using Hoffman differential contrast optics and bright field inverted optics with heated stage and at different magnification. The examinations of PN were completely non-invasive, which did not last for more than 15 sec. The criteria employed for the morphological evaluation as described by Scott and Smith (4). Cleaving Embryo Evaluation Embryos were monitored daily at the same time in the morning. The number of fertilized oocytes, embryos cleaving to 4 to 8-cell, morula, blastocysts (early, expanding, expanded) was recorded. At 40–42 hrs and then after 69–71 hrs, embryos that had cleaved to the two-cell stage or further were identified and graded using criteria based on blastomere number, symmetry, and degree of fragmentation. The grading system used was based on the scale A-D where grade A represents the highest quality. Blastocyst Evaluation Blastocyst quality was determined according to the modified method of Gardner and associates (17). A good grade blastocyst have a blastocoel, well defined trophectoderm with enough cells to form a continuous layer without a single cell flattening on the surface. Also, a well- defined and organized inner cell mass (ICM) are present. Embryo Transfer ET was performed on day two- or five-post retrieval using Edwards-Wallace catheter (Smiths Industries, UK). Only embryos of the highest quality at the 4-6-cell stage or high quality blastocysts were transferred. Any excess cleaving embryos with more than 4-cell and less than 25% fragmentations were cryopreserved.. Luteal support was started after oocyte retrieval with progesterone (50 mg/ day) (18). A pregnancy test was performed 14 days after ET. A clinical pregnancy was defined as a gestational sac within the uterus (which excludes ectopic and biochemical pregnancies). Table 1. Clinical results of infertility cycles with tubal factor infertility (IVF) and male factor infertility (ICSI).
NS= non-significant. Statistical Analysis The fertilization rate (percentage of oocytes that fertilized) and cleavage rate (percentage of zygotes that underwent at least one cell division) were calculated. Clinical pregnancy rate was defined as the number of couples with a fetal heart rate on ultrasound divided by the number of couples undergoing IVF or ICSI. Data are presented as means ± standard deviation. SPSS for windows version 11.5 (SPSS, Chicago, IL) was used for statistical analysis. Chi- square and Fisher's exact tests were used to analyze normal variables in the form of frequency tables. Statistical significance was set at p<0.05. RESULTS The general characteristics of ART cycles are presented in Table 1. The highest percentage of grade A embryos were from Z1 and Z3 zygotes. All pregnant women in IVF group had at least one embryo transferred, which resulted from Z1 zygote. This was also true for over 97% of ICSI cases. In both IVF and ICSI, over one-third of zygotes were grade Z1. However, Z4 were the least frequent patterns found in ART cases (Table 2). In IVF group, a total of 34 and 23 were grades A and B embryos for day-2 ET. The highest rate of grade A embryo formation was found in IVF cycles. In ICSI group, a total of 25 embryos with grade A were formed for day-2 ET, while 30% of embryos were grade B. The data related to the correlation between the zygote scoring (Z1-4) and the quality of cleaving embryos and blastocyst formation is presented in Table 3. The results showed that Z1 was involved in about half of grade "A" embryo formation in IVF and ICSI cycles with day-2 ET. In all embryo development, the Z4 category was found to be the least frequent. In IVF, almost 43% of the low quality (grade "D") embryos were from Z3; while, in ICSI, the majority of grade "D" embryos were from Z2 embryos. The other objective was to find out which type of zygote scoring is involved with generation of blastocysts. Results showed that all 4 zygote scores have the potentials to develop into blastocyst stage. In both IVF and ICSI, Z2 was the most frequent; while, Z4 had the least correlation to blastocyst formations. The results also showed that in cases resulted in clinical pregnancy, Z3 were the dominant zygotes that resulted in cleaving embryos to be transferred on day 2. However, Z4 were the least zygote type involving with embryos that were transferred into uterus. In regards to blastocyst development for transfer, Z1 and Z2 were the dominant zygotes in IVF and ICSI that resulted in pregnancy, respectively. Z3 patterns were the least found in both IVF and ICSI (Table 4). The rate of pregnancy/ cycle started was 25.7% for IVF and 22.9% for ICSI. Table 2. The distribution of zygote types in both IVF and ICSI.
n= total number of zygotes in each group. DISCUSSION With introduction of extended culture and blastocyst transfer, the rates of pregnancy and implantation have been increased. This allows selecting one or two blastocysts for transfer without reducing the chances of pregnancy, while minimizing the incidence of high-order multiple pregnancies (8). However, only half of the zygotes placed in extended culture may reach the blastocyst and, of these 30%-40% implant, meaning that even extended culture with blastocyst transfer is inefficient. In the current study, 20 cycles were performed with extended culture and the ET took place 5 days post oocyte retrieval. We aimed to investigate whether zygote scoring is correlated with embryo development on day-2 and -5 of culture. There is a clear relationship between zygote morphology and the ability to implant; therefore, screening embryos at the zygote stage and again at the blastocyst could increase the implantation rate, enabling single blastocyst transfers (17, 19). A second level of embryo screening could also help in selection of patients for extended culture. It has been reported that the PN pattern of the zygote is closely related to blastocyst formation and quality (5, 8). Other studies stated that PN morphology also predicts embryo chromosomal constitution (9, 14). Further, it has been reported that in patients >38 years, zygotes with similar PN size and polarized nuclear polar bodies present the best prognosis based on embryo quality and incidence of chromosomal abnormalities (20). All of our patients were under age of 40, whom were enrolled for ART treatment according to the etiology of their infertility In a recent study, the morphological pattern of PN according to Scott's Z system was evaluated to determine if PN morphology is a better predictor of pregnancy than traditional embryo morphology scoring (21). In this study, the data showed that Z1 and Z3 embryos resulted in significantly higher quality embryos than other Z groups. Our results, however, showed that in both IVF and ICSI with day 2 ET, Z1 and Z3 were the most common patterns. In addition, pregnancy rates reported from Payne and colleagues were similar between Z1 and Z3 embryos (21). Their findings also showed that using embryo morphology, pregnancy rates were highest in transfers with 1 or 2 best quality embryos, which is in agreement with our findings. Table 3. The correlation between zygote scoring and quality of cleaving embryos and development to blastocysts in IVF or ICSI.
*P<0.05 between A+B and C+D embryos. **P<0.05 between Z4 in IVF vs ICSI. Table 4. The correlation between zygote scoring and clinical pregnancy outcome in cases with day 2 or day 5 embryo transfers (ET) in IVF and ICSI cycles.
*P<0.05 between Z2 in IVF vs ICSI. **P<0.01 between Z1 in IVF vs ICSI. They believed that method on embryo morphology was equal to or even better that the Z-score model in predicting pregnancy. The Z-score distribution in Payne et al.'s study (21) was different than Scott et al.'s (22) in that they had mainly Z1s (27%) and Z3 (50%), while Scott et al.'s had primarily Z1s (38%), Z2 (32%), Z3 (27%), and Z4 (5%). In our study the blastocysts generated from IVF cycles, 36.5% and 24.3% were Z1 and Z2, respectively. These rates were changed to 35.9% and 31.3% in ICSI group. Scott et al.'s study showed that all patients who achieved clinical pregnancy had at least one Z1 or Z2 embryo transferred (22). Our cases with clinical pregnancies from day-2 ET were the ones with highest rates of Z1 and Z3. However, in cases of clinical pregnancies from day-5 ET, Z1 and Z2 were the highest rates of zygote patterns. In all cases with pregnancies, Z4 were the least zygote pattern found, which is in agreement with report from Arroyo et al. (23). Their study also showed that patterns Z1 and Z2 were associated with good quality embryos and higher rates of ongoing pregnancy (23). Another study also reported that day 3 E.T. with combined evaluation at the PN and cleavage stages compares favorably with blastocyst transfers (24). It seems that PN scoring combining with other embryologic strategies are useful tools to overcome the ART failure. In addition, Lan et al. have recently reported that a combined evaluation of the Z-score and embryo morphology significantly increases implantation rates and is highly predictive in assessing embryo survival on day-5 blastocysts (25). This is in agreement with our findings as well. In contrast, Jaroudi et al. compared the transfer of the two best zygotes on day-1 versus the two best cleavage-stage embryos on day 3 and concluded that day-3 E.T. result in better implantation rates and that the present PN scoring does not reliably select the zygotes for transfer (26). Recently, Guerif et al. (2007) and Nicoli et al. (2007) reported that the predictive power of pronuclear morphology is weak in assisted reproduction outcomes (27, 28). Guerif and co-workers employed the Tesarik’s zygote scoring system to predict the blastocyst developmental potential (27). Their results showed that early cleavage was the most powerful parameter to predict the development of a good morphology blastocyst in IVF and ICSI cycles. In addition, Z- scoring system was applied by Nicoli et al. (2007) to investigate its role as predictor of pregnancy outcome in ART program. It was shown that the most common pattern was Z3 (72.4%), followed by Z1 and Z2. Also, the incidence of pregnancy as well as implantation rates were not significantly different among the Z- groups. Therefore, they concluded that Z-score is not superior to the standard morphologic criteria for selecting embryos with a better chance of successful pregnancy (28). The development potential of PN zygotes in relation to their orientation has been studied (29). The investigators observed that the four different types of PN orientation were independent of the fertilizing spermatozoon; also, there was no association with implantation or pregnancy rates. They reported that Z1 and Z3 embryos had similar high quality morphology and pregnancy rates. Therefore, the decision model based on the Z-score model is not superior to standard embryo morphology in predicting pregnancy outcome. Recently, it has been reported that PN morphology scores of 1, 2, or 3 do not correlate with live birth rates when assessing PN morphology score (10). Indeed, we did not evaluate the correlation between zygote scoring and live birth rates in our patients. Our results are correlated with clinical pregnancies. Also, the relationship of PN morphology and chromosomal status at the cleavage stage has been investigated (9). They scored the PN morphology using Scott Z-score system. After ET, arrested or non-transferred 2PN embryos were spread for fluorescence in situ hybridization (FISH) staining. The results demonstrated that over 70% of Z1 group were normal diploid, which was significantly more than Z3 and Z4 groups. Therefore, their findings confirmed a high probability to get normal diploid embryos if good morphology at PN stage was used as selection criteria. In conclusion, our results confirm that PN morphology assessment can predict embryo development and pregnancy outcome in ART cycles. The Z-scoring criteria is a useful tool in the selection of embryos, both in cellular and blastocyst stage, and the most suitable embryos for transfer. ACKNOWLEDGEMENT The authors are very grateful to Professor Safaa Al-Hasani, ART center, University of Lubeck, Germany, for his critical review of the manuscript. We thank Dr. Naimeh Tayebi for her assistance with data analysis. The assistance of Mrs. L. Sharegh, N. Shekar-Riz, and S. Baghazadeh is also appreciated. REFERENCES
©Copyright 2008 - Middle East Fertility Society The following images related to this document are available:Photo images[mf08010f1.jpg] | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| |||||||||

{kind=link}