 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
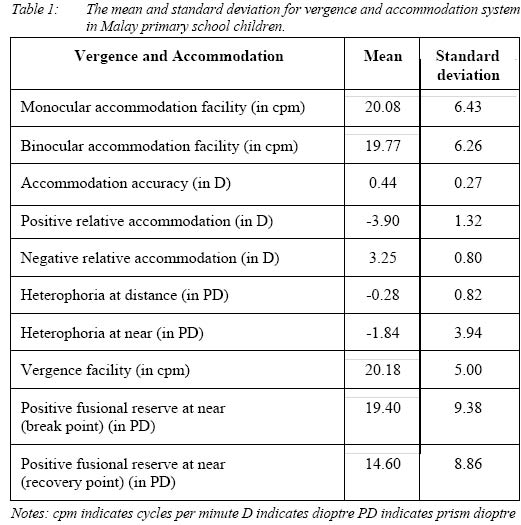
Malaysian Journal of Medical Sciences, Vol. 9, No. 1, January 2002, pp. 9-15 Vergence and Accommodation System in Malay Primary School Children Ai Hong Chen & Ahmad Hakimi Zainol Abidin Department of Optometry, Faculty of Allied Health Sciences,
Universiti Kebangsaan Malaysia, Jalan Raja Muda Abdul Aziz,
50300 Kuala Lumpur, Malaysia
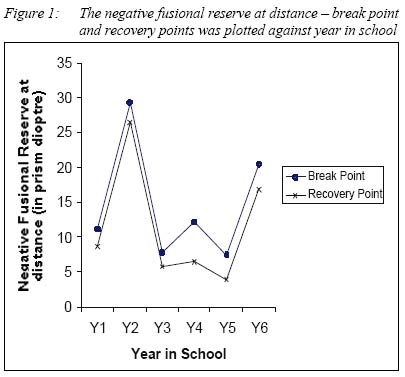
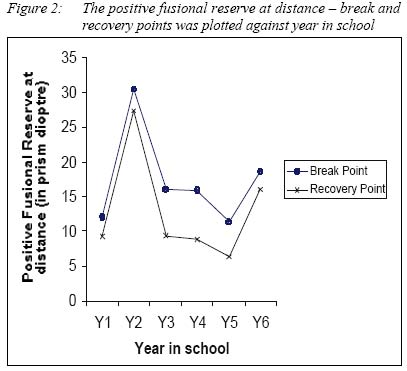
Submitted-22.5.2001 Code Numbers: mj02003 Sixty primary school children, were measured for for accommodation and, vergence facility, accommodation accuracy, relative accommodation, fusional vergence / reserve and heterophoria. Analysis of Variance revealed that no - single factor was significant by involved among the six age groups for all the above (p>0.05). However, a significant age difference (p<0.05) was found in the fusional reserve. The mean and standard deviation was 20.08 (±6.43) cpm for the monocular accommodation facility, 19.77 (±6.26) cpm for the binocular accommodation facility, 20.18 (±5.00) cpm for the vergence facility, 0.44 (±0.27) D for the accommodation accuracy, -0.28 (±0.82) PD for the heterophoria at distance, -1.84 (±3.9) PD for the near heterophoria, 3.25 (±0.79) D for the negative relative accommodation, and -3.90 (±1.32) D for the positive relative accommodation. There was no age difference in the accommodation and the vergence status between years the ages of 7 and 12 years old but the fusional reserve component of the vergence system varied with age. The vergence and the accommodation findings in our subjects were discussed and compared with previous studies to serve as a guideline in clinical data interpretation and diagnosis for binocular vision problems in Malay children. Key words : Vergence, accommodation, children's vicion INTRODUCTION The normative data for vergence and accommodation parameters found in textbooks on binocular vision has been used worldwide as guidelines to diagnose and to treat binocular anomalies (1-6). However, the clinical application of the norms from the textbooks (mostly based on Caucasian data) under different ethnic background and different age groups might be complicated and demand different data interpretation to take into the consideration of the influence of the age and race factors. The effect of race has been reported to influence the amplitude of accommodation (7-8). However, the race effect on other binocular parameters is negligible in adults (9). The age differences on binocular parameters like the near point of convergence, the amplitude of accommodation, the heterophoria and the accommodation facility have also been reported (10-11). Since both the race and age might influence the norms for vergence and accommodation system, it is important to investigate the vergence and accommodation status in Malay primary school children that had not been reported previously. The baseline data from this study might lead to a better interpretation and diagnosis for binocular vision problems in Malay primary school children. MATERIALS AND METHODS Sixty Malay primary school children, Year 1 to Year 6, participated in this study. Ten subjects (5 males, 5 females) were randomly selected from each Year in school. The selection criterion was 6/6 visual acuity or better with no previous history of ocular problems. Measurements were taken for accommodation facility, vergence facility, accuracy of accommodation, relative accommodation, fusional reserve and heterophoria. The accommodation component was examined under both monocular and binocular viewing conditions, while the vergence component was tested binocularly only. All the procedures were performed under room illumination. Description of procedures for accommodation measurements The accommodation facility was measured with ±1.50 Dioptres flippers, fixating N5 font size text at 40cm. One cycle was measured as +1.50 / -1.50 / +1.50 or -1.50 / +1.50 / -1.50. Each subject was told to clear the +1.50DS lens and -1.50DS lens alternately as fast as possible within one minute. The ±1.50DS flippers were placed first over the right eye and then both eyes to measure monocular and binocular accommodation facility respectively. The number of cycles per minute (cpm) was recorded. The accuracy of accommodation was measured by using the retinoscope and near card - the Modified Estimation Method (MEM). The accuracy of accommodation was recorded as the total spherical power in dioptre (D) to neutralize the retinoscopic reflex movement. The relative accommodation was measured with minus (negative) and plus (positive) lenses. Subject fixated at the N10 font size text at 40cm, while the power of the spherical lenses was increased in 0.25D step until blur vision was reported by the subject. Plus lenses were first used and followed by minus lenses. The highest positive lens power before blur vision was recorded as negative relative accommodation, while the highest negative lens power before blur vision was recorded as positive relative accommodation. The findings were recorded in Dioptre (D). Description of procedures for vergence measurements Vergence facility was measured by using the loose prisms (3 prism dioptres base-out and 3 prism dioptres base-in) while looking at the N5 text at 40cm. One cycle was measured as base-out / base-in / base-out or base-in / base-out / base-in. This procedure was conducted under binocular viewing only with the base-in and base-out prisms alternately placed in front of the right eye within 30 seconds. Each subject was told to fuse the target as fast as possible. The findings were recorded in cycles per minute (cpm). The heterophoria was measured with the Maddox Rod Method at 6 meters and the Howell Card Method at 33 centimeters. In the Maddox Rod Method, the Maddox rod lens was placed in front of the right eye, while the measuring prism was place in front of the left eye. The right eye of the subject saw a red streak light while the left eye saw the light spot. The subject was asked to report the position of the red streak light relative to the position of the light spot. Crossed position indicated exophoria, while uncrossed position indicated esophoria. Base-in prism was used to measure the exophoria and base-out prism was used to measure the esophoria. In the Howell Card Method, an 8D base-down prism was placed in front of the right eye. The patient was instructed to report to which number or picture on the bottom number/picture bar the top arrow pointed. Odd numbers or pictures on the yellow side indicated esophoria while even numbers or pictures on the blue side indicated exophoria. The findings were recorded in prism dioptres (PD). The fusional vergence / reserve was measured with a prism bar at 6 meters (target: 6/9 Snellen) and 40 centimeters (target: N5 text). The prism bar was placed in front of the right eye. Base-out prisms were used to measure positive fusional reserve while base-in prisms were used to measure negative fusional reserve. The break and recovery point was determined objectively by observing the eye movements. The break and recovery points were recorded in prism dioptre (PD). RESULTS Analysis of Variance (ANOVA-single factor) did not show any significant difference for the six age groups (Year 1 to Year 6) in the monocular accommodation facility [F=1.68, df=5,54, p>0.05], the binocular accommodation facility [F=2.29, df=5,54, p>0.05], the vergence facility [F=2.57, df=5,54, p>0.05], the accuracy of accommodation [F=2.55, df=5,54, p>0.05], the positive relative accommodation [F=1.52, df=5,54, p>0.05], the negative relative accommodation [F=0.45, df=5,54, p>0.05], the heterophoria at distance [F=1.31, df=5,54, p>0.05], the near heterophoria [F=0.60, df=5,54, p>0.05], the positive fusional reserve at near - break point [F=3.33, df=5,54, p>0.05], and the positive fusional reserve at near - recovery point [F=2.67, df=5,54, p>0.05]. Table 1 showed the mean and standard deviation for the above ten parameters. However, a significant age difference was found in the fusional reserve (both positive and negative fusional reserve at distance, negative fusional reserve at near). ANOVA-single factor showed significant difference for the six age groups (Year 1 to Year 6) in the negative fusional reserve at distance - break point [F=13.34, df=5,54, p<0.05], the negative fusional reserve at distance - recovery point [F=18.33, df=5,54, p<0.05], the positive fusional reserve at distance - break point [F=7.80, df=5,54, p<0.05], the positive fusional reserve at distance - recovery point [F=11.66, df=5,54, p<0.05], the negative fusional reserve at near - break point [F=4.40, df=5,54, p<0.05], and the negative fusional reserve at near - recovery point [F=5.24, df=5,54, p<0.05]. The changes of the above parameters with age were shown in Figures 1, 2 and 3. DISCUSSION There is no age difference in the accommodation status (facility, relative and accuracy) and the vergence status (heterophoria and facility). However, the fusional reserve component of the vergence system varies with age, except for the positive fusional reserve at near. The accommodation facility found in our study was higher than the norms reported by Scheiman & Wick (1). They reported 7 (±2.5) cpm for monocular accommodation facility and 5 (±2.5) cpm for binocular accommodation facility. The monocular and binocular accommodation facilities in our study were 20.08 (±6.43) cpm and 19.77 (±6.26) cpm respectively. The lower power of flippers (±1.50D) used in our study might be the contributing factor to our higher readings, compared with their ±2.00D flippers because the range of the relaxation and stimulation of the accommodation system was smaller in lower power lenses. The vergence facility (20.18 ± 5 cpm) reported in our study was approximately three times higher than the vergence facility (7.0 cpm) reported by Scheiman & Wick (1). The power of the prisms used in previous study (8 base-in and 8 base-out) was approximately three times higher than the prism power (3 base-in and 3 base-out) used in the present study. The difference in the prism power might contribute to the difference of the vergence facility findings between the two studies. We used lower lens or prism power for the accommodation facility and the vergence facility assessment respectively because readings were difficult to obtain for the lens and prism power suggested in Scheiman & Wick (1) for comparison purpose. The school children were found to be more co-operative in performing the test when lower power lenses and prisms were used. The accuracy of accommodation reported in our study was +0.44 (± 0.27) D. It was very similar to the norms reported in previous studies. Scheiman & Wick reported the norm for accommodation accuracy as +0.50 (±0.25) D (1), while Bruce & Philip reported that the accuracy of accommodation ranged from +0.25D to +0.75D (12). The heterophoia at distance (-0.28 ± 0.82 PD) and at near (-1.84 ± 3.94PD) reported in this study was still within the normal range previously reported for adults. All researchers found a high incidence of orthophoria at distance (14-16, 20, 22, 24, 26). Most researchers had reported exophoria of about 0 to 6 prism dioptres at near (13, 17-19, 21, 23, 25, 27-29). The relative accommodation reported in this study was higher than those adult norms reported by Scheiman & Wick (1). In our study, the positive relative accommodation was -3.92 (±1.32) D while the negative relative accommodation was +3.25 (±0.80) D. Scheiman & Wick reported +2.00 (±0.50) D for the negative relative accommodation and -2.37 (±1.00) D for the positive relative accommodation (1). According to Grosvenor (30), the relative accommodation depended on two factors such as the amplitude of accommodation and the range of fusional vergence. Since the amplitude of accommodation had been reported to decrease with age (31), the higher relative accommodation found in our study was most likely due to our younger subjects (school children) with higher amplitude of accommodation (Scheiman & Wick`s values were based on adults). Children were reported to have different fusional reserve from adults (32-33). For children between 7 and 12 years old, the break and recovery values of the positive fusional reserve at near were 23 (±8) PD base-out and 16 (±6) PD base-out respectively. The break and recovery values of the negative fusional reserve at near for children were 12 (±5) PD base-in and 7 (±4) PD base-in respectively. Meanwhile, the break and recovery values of the positive fusional reserve at near for adults were 19 (±9) PD base-out and 14 (±7) PD base-out respectively. The break and recovery values of the negative fusional reserve at near for adults were 13 (±6) PD base-in and 10 (±5) PD base-in respectively. Age differences were found in the fusional reserve of primary school children from Year 1 to Year 6 in this study. However, the trend of changes with age was not absolutely clear because our sample size was small. In order to provide a clearer picture of the age differences on fusional reserve, more subjects are needed in future investigation. It is important to investigate the fusional reserve because the normal and abnormal values of the break and recovery point indicate the compensation and incompensation of the binocular system of the eye respectively. Binocular instability has been associated with myopia progression (34-35). The age range of our subject sample coincides with the age range when school myopia develops. Therefore, the variation found in the fusional reserve data might be associated with exposure of school near task (one of the risk factor for myopia progression). However, fusional reserve has not been correlated with the school myopia progression. The association needs further investigation in a longitudinal study. In summary, there is no age difference in the accommodation status (facility, relative and accuracy) and the vergence status (heterophoria and facility) between 7 and 12 years old but the fusional reserve component of the vergence system varies with age. REFERENCES
Copyright 2002 - Malaysian Journal of Medical Sciences The following images related to this document are available:Photo images[mj02003t1.jpg] [mj02003f1.jpg] [mj02003f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}