 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Malaysian Journal of Medical Sciences, Vol. 9, No. 1, January 2002, pp. 16-20 The Pharmacokinetics of Single Dose vs Steady-State Doses of Propranolol in Cirrhotic Malay Patients Zain-Hamid, R.*, Ismail, Z. *, Mahendra Raj, S.**, Shuaib, I. L.*** & Mohsin, S. S. J.* *Department of Pharmacology, **Department
of Medicine and ***Department of Radiology, School of Medical
Sciences, Universiti Sains Malaysia 16150 Kubang Kerian, Kelantan, Malaysia Submitted-28.5.2000 Code Numbers: mj02004 Pharmacokinetics of propranolol (PRN) given orally were studied in twelve cirrhotic Malay patients [10 males, 2 females], aged 33-62 years [49.83+9.17], body weight 39-72 kg [58.0+8.46] and height 142-168 cm [158.8+7.89] following single 20 mg and steady-state 20 mg tds for 7 days dosing of PRN. Blood samples were withdrawn hourly up to 48 hours. PRN concentrations in the plasma were assayed by HPLC with oxprenolol as the internal standard. Pharmacokinetic parameters were analysed using a non-linear regression program MultiForte. Area under the curve (AUC) as performed using the linear trapezoidal rule. Student's t-test was used to test for statistical significance and AUC in Malay cirrhotic patients was found to be much bigger than that observed in Caucasians. Steady-state AUC was significantly increased following multiple dosing (961.31+7.47 vs 2954.19+1153.34 ng.hr/ml), however, the volume of distribution (Vd) declined (543.89+292.91 vs 224.14+1003.12 L) significantly compared to that of a single dose. The apparent systemic clearance (CL) was significantly reduced at steady-state (436.04+209.4 vs 129.51+48.42 ml/min) in comparison to single dose therapy. The peak plasma concentration (Cpmax) was greatly increased at steady-state (54.32+22.37 vs 136.10+38.63 ng/ml). Based on the AUC, PRN bioavailability was greater in cirrhotic Malay patients compared to Caucasians who took only 20 mg instead of 80 mg doses. The decline in drug clearance following steady-state was due to saturation of the metabolizing capacity of hepatic enzymes and a decreased portal blood flow. Reduced Vd was believed to be caused by increased drug-receptor interactions and decreased tissue/protein binding of PRN in these patients. Key words : propranolol, pharmacokinetics, cirrhosis, bioavailability, steady-state INTRODUCTION Propranolol is a non-selective beta adrenergic blocker which
is used to treat a number of diseases including cirrhosis. It has proven useful
for the treatment of portal hypertension when once bleeding of varices had
stopped. This study is a sequel to a previous pharmacodynamic study where propranolol
was used at various doses to control portal hypertension. We found that 20
mg given three times daily (tds) was the optimal dose required to control
variceal bleeding in cirrhotic patients in
comparison to 10 mg or 30 mg tds (1). Thus, we would like
to observe the pharmacokinetic profile of this
chosen dose in these patients at single dose and also
at steady-state. This is a first attempt to document
the pharmacokinetic profile of propranolol in Malays.
The aims of the study were to determine the
single dose and the steady-state dose
pharmacokinetic profiles of propranolol in cirrhotic Malay
patients and to compare the pharmacokinetic parameters
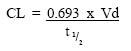
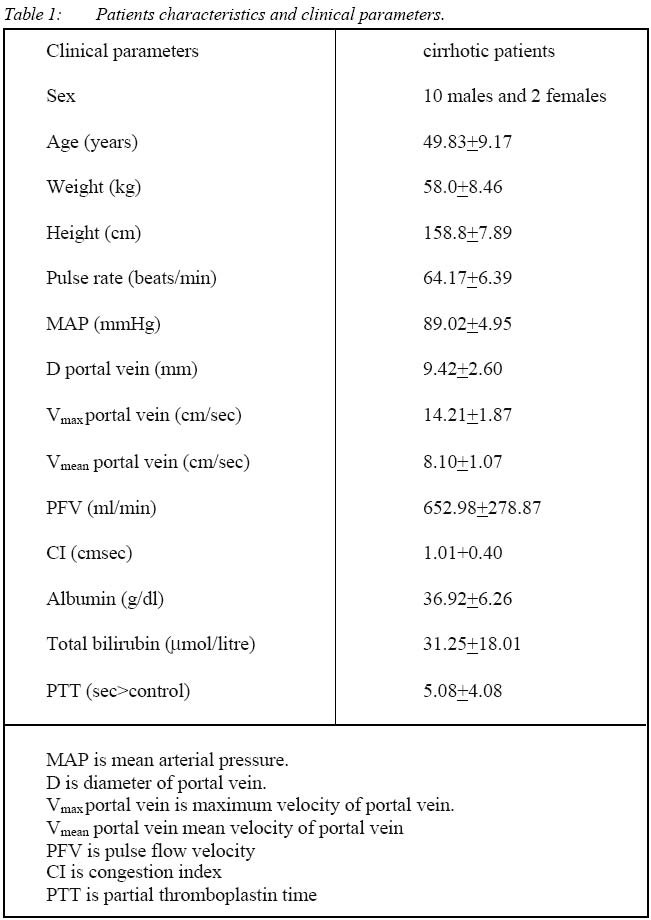
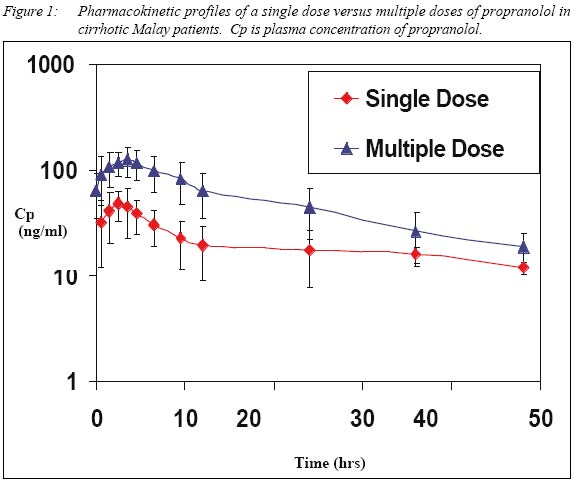
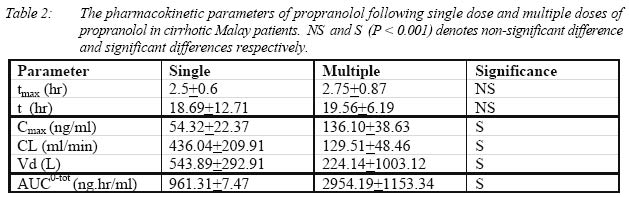
of the two conditions. Subjects There were 12 subjects involved in the study, consisting of 10 males and 2 females, who ranged in age from 33 to 62 years (49.8+9.17 years), body weight from 39 to 72 kg (58.0+8.46 kg) and height from 142 to 168 cm (158.8+7.89 cm). These are the same patients who had completed a previous pharmacodynamic study (1). All subjects gave an informed consent and the study protocol was approved by the university's ethical committee. Inclusion criteria were Malay patients with liver cirrhosis, (11 were post-hepatitis B and 1 with biliary cirrhosis). The diagnostic criteria were based on clinical, biochemical and ultrasonagraphic analysis. Based on Child-Pugh classification (2), 6 patients were in Grade A, 4 in Grade B and 2 in Grade C. Table 1 shows the patients characteristics and clinical parameters. All had experienced previous variceal bleeding, but had no variceal bleeding at least 6 months prior to this pharmacokinetic study and were not on any other medication at the time of the study. Study protocol For single dose study, volunteers fasted overnight and for 3 hours after oral administration of the drug. For steady-state study, subjects were not hospitalised and had no dietary control for the first 7 days of dosing, however, all volunteers were kept in the hospital ward for blood sampling and for observation. For the single oral dose study, patients were given 20 mg propranolol while for the multiple dosing study, propranolol was given 20 mg tds orally for at least 7 days. A cannula was inserted into the antecubital vein of each subject for ease of blood sampling. Ten (10) ml of blood were withdrawn into heparinised tubes at hourly intervals up to 48 hours after dosing. The samples were centrifuged immediately and stored frozen (-20oC) until analysis. For the steady-state levels, blood samples were taken on the 8th day of medication. All analyses were performed within two weeks after blood sampling. Analysis of propranolol One ml of plasma and 75 ml oxprenolol, (100 mg/ml) as internal standard, were placed in a screw-capped glass tube. To each tube, 100 ml water and 50 ml 5N NaOH were added, followed by vortexing for 30 seconds. The drugs were extracted with 3 ml of the extraction solvent (isoamyl-alcohol [1.5 ml]:n-heptane [95.5 ml]) and shaken on a rotator for twenty minutes. This was followed by centrifugation (3000 rpm) for 30 minutes. The organic phase was then transfered by aspiration to clean glass tubes. The extraction procedure was repeated with the remaining samples. A gentle flow of nitrogen (10 ml/min) was used to dry the organic phase. The residue was reconstituted in 100 ml of methanol and vortex-mixed for 20 sec. Twenty microlitres of the sample was injected directly onto Lichrosorb C18 HPLC (12.5 cm) column and detection was by ultraviolet detector set at 295nm. The HPLC system comprised of a Waters` 610 peristaltic pump, a Waters` 600 system controller, a Waters` variable wavelength UV detector, a Rheodyne 7125 manual injector and a Hewlett-Packard 3390A intergrator. The mobile phase constituted of a mixture of water, methanol, acetonitrile, acetic acid and triethylamine in the proportion of 160 ml:80 ml:70 ml:2.5 ml:125 ml respectively. The pH was adjusted to 3.4 using 1N NaOH before the addition of triethylamine. The mobile phase was filtered with 0.45 mm filter paper under vacuum suction to filter all residues and to remove dissolved gas. The mobile phase flow rate was 0.5 ml/min. Under these conditions, the retention times for propranolol and oxprenolol were 6.31 and 8.80 mins respectively. The limit of detection for propranolol was 9 ng/ml, the recovery from plasma was between 92.3 to 103.6% and the intra-assay coefficient of variation (CV) was 6.41% over a concentration range of 15 to 180 ng/ml in plasma (3). Pharmacokinetic and statistical analysis Compartmental modelling was accomplished with the aid of a non-linear regression program MultiForte (4). AUC calculations were performed using the linear trapezoidal rule. Single versus steady-state doses pharmacokinetic parameters were compared using Student's t-test. RESLUTS The pharmacokinetic profiles following single and multiple doses of propranolol are shown in Fig. 1. There is a wide interindividual variation in drug levels in these groups of patients following propranolol intake. With multiple dosing, a bigger area under the curve (AUC) was produced compared to a single dose. Comparisons of each pharmacokinetic parameter are as shown in Table 2. At steady-state dosing, there were no significant differences in tmax (time to maximum concentration) and t1/2 (elimination half-life) as compared to single dose values. Significant differences (P<0.001) were however, seen in Cmax, CL, Vd and AUC. On multiple dosing, AUC had tripled, Cmax had doubled while CL had decreased to a quarter of that of the single dose regimen while Vd had decreased to half. DISCUSSION On multiple oral dosing, the time taken to reach maximum plasma concentration (tmax) and the half-life (t1/2) did not change significantly. Changes in t1/2 is dependant on CL and Vd. The Cmax had doubled on multiple dosing indicating more drug was made available at steady-state than single oral dose of propranolol. Our study has shown that in cirrhotic Malay patients there was no change in the t1/2 of the drug studied. This is different from the study done by Chidsey et al, 1975 (4), who found that in non-cirrhotics, the t1/2 increased from 2.5 hours during single dose to 5.5 hours on chronic dosing. The clearance had decreased tremendously, in fact to a quarter of that of a single dose (Table 2). On chronic use of propranolol, the enzyme systems of the liver would be saturated. There would be a decrease in clearance due to a decline in portal blood flow. Propranolol has significant first-pass effect and thus also a high hepatic clearance. Therefore, a decline in hepatic blood flow will significantly affect its removal by the liver (5). Thus, theoretically, there should be an increase in drug bioavailability and also an increase in t1/2. The present study showed an increase in drug bioavailability by an increase in AUC but no change (prolongation) in t1/2. Repeated doses caused a decline in Vd indicating that there was less tissue binding of propranolol so that more free drug was made available for a pharmacological response. Multiple dosing increased the drug bioavailability, decreased protein binding and decreased the amount of drug being distributed to tissues, thus the Vd dropped. The decline in Vd was parallel to that of CL. This is in agreement with the equation of:
As there was no change in t1/2, the decline in CL would parallel that of Vd. This is in agreement with the study done by Arthur et al (1985) (7) whereby propranolol protein-binding declined in cirrhotic patients in comparison to non-cirrhotics which resulted in more free drug being available and a small Vd. Decreased clearance was supported by a triple increase in AUC at steady-state dosing (Table 2). The AUC seen in these patients was much larger than that observed by other workers (8) despite these patients taking only 20 mg tds instead of 80 mg tds of propranolol. The AUC was larger than the previous study (8) probably due to the degree of cirrhosis (which may be due to delay in getting immediate treatment by our patient group). On continous dosing, levels of propranolol measured at 48 hours were still much higher than the corresponding single dose plasma concentrations. This in a way contributes to a bigger AUC and a decrease in CL. It takes longer for propranolol to leave the body. CONCLUSION This study showed that repeated dosing of propranolol in cirrhotic Malay patients produced no alteration in t1/2, a lower Vd, a larger AUC and poor drug clearance, indicating accumulation of propranolol in comparison to a single dose regimen.
ACKNOWLEDGEMENTS We are grateful to R & D Grant, Universiti Sains Malaysia, A/C No. 31/0500/3570 and UPHA Corpn, Bangi, Selangor, Malaysia and to Encik Abdul Razak Ahmad for his technical assistance. REFERENCES
Copyright 2002 - Malaysian Journal of Medical Sciences The following images related to this document are available:Photo images[mj02004t2.jpg] [mj02004f1.jpg] [mj02004t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}