 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
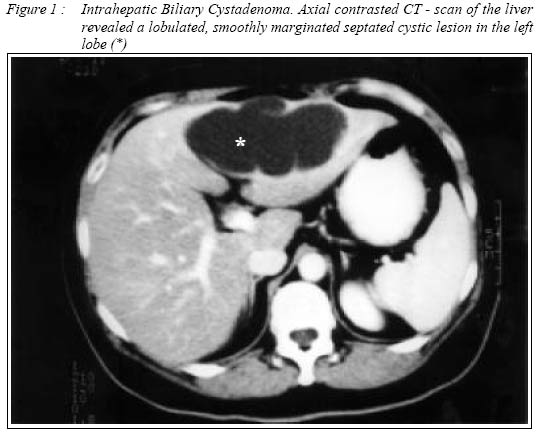
Malaysian Journal of Medical Sciences, Vol. 9, No. 1, January 2002, pp. 49-51 Case Report BILIARY CYSTADENOMA - Computed Tomography Findings Ariff AR, Haida Hassan & John G* Department of Radiology, Hospital Universiti Sains Malaysia,
16150 Kubang Kerian, Kelantan, Malaysia. *Department of Radiology,
University Malaya Medical Centre, 50603 Kuala Lumpur, Malaysia Submitted-28.5.2000 Code Number: mj02009 Biliary cystadenoma is a rare neoplasm of the biliary ductal system. Surgical management yields an excellent result. We present a case of recurrent biliary cystadenoma in the left lobe of the liver. The cyst was successfully treated with hepatic segmentectomy. The lobulated smoothly marginated septated cystic lesion noted on computed tomography (CT) were highlighted and the other imaging studies, differential diagnosis and management were reviewed. Key words : Biliary cystadenoma , Computed tomography. INTRODUCTION Biliary cystadenomas are large, usually multiloculated benign tumours. They arise from intrahepatic or, rarely extrahepatic ducts and represent less than 5 % of solitary non parasitic cysts of biliary origin. This multilocular cyst is lined by cuboidal or columnar epithelium. Their cause remains unknown, although presence of aberrant bile ducts in cystadenomas suggest congenital etiology. No association with oral contraceptive use has been documented. If the cystadenomas are of developmental origin, then their late presentation must be ascribed to very slow growth and/or accumulation of fluid (1). This paper will outline the CT findings of a biliary cystadenoma and discuss the other diagnostic imaging modalities, management and the possible differential diagnosis of the cystic lesions. Case report A 56 - year - old medium built Chinese woman was admitted to the University Hospital for hepatic segmentectomy for a recurrent biliary cystadenoma which was identified by ultrasound during follow-up assessment at an out patient clinic, where a large thick walled septated cystic mass in the left lobe of the liver was found. A review of her past surgical history revealed that she had undergone an operation to deroof a cystic lesion in the left lobe of the liver 8 months previously. One hundred millilitres of clear yellowish colour fluid was aspirated. The histopathological report of the removed specimen revealed a biliary cystadenoma. She had also undergone hysterectomy for a carcinoma of the cervix 2 years ago. Her post hysterectomy was complicated with deep vein thrombosis which was succesfully treated with warfarin. She was also hypertensive on oral propanolol 40 mg b.d for the past 2 years. On her present admission, she complained of nausea and vomiting for the past two months associated with severe epigastric pain and diarrhoea. She had neither fever nor jaundice. Physical examination revealed an abdominal mass in the epigastrium measuring 6.0 x 8.0 cm. The haematological and biochemical investigations were normal. Computed tomography of the liver showed a well defined lobulated septated 9.5 x 6.5 x 6cm cystic lesion in the left lobe occupying segments II and III ( figure 1 ). The CT values of the cyst were ranging from +10 - +13HU. In view of past history of cervical carcinoma, the possibility of cystic metastases was put into consideration. The lesion was completely removed with a left lateral hepatic segmentectomy. Pathologic examination of the excised specimen was a biliary cystadenoma. The multiloculated cyst was well encapsulated and sharply demarcated from the adjacent tissue. The cystic spaces were filled with mucinous fluid. Patient made an uneventful and complete recovery. DISCUSSION The majority of biliary cystadenomas occur in middle aged women presenting with an abdominal swelling or a right upper quadrant mass of weeks to years duration. Pain and biliary obstruction may be present. Our patient had most of these features. Other clinical presentations include weight gain or loss, increased abdominal girth, anorexia, nausea, vomiting, jaundice and biliary colic. CT examination is useful in assessing the extent of involvement. CT and ultrasound are complementary for the evaluation of internal morphology, size and extent of this tumour (2). The characteristic CT appearance of this tumour is that of a low-density intraheptic mass with internal septae and mural nodules. Typically, such lesions are multiloculated having low attenuation cystic regions ranging from 0 to + 40 HU. However CT attenuation numbers are of little value in separating these from other cystic lesions. Contrast enhancement is seen along the internal septa and wall. However CT failed to display the thick cyst wall (3) as in our patient. Sonography usually depicts the true internal morphology of cystic hepatic lesions more clearly . Biliary cystadenomas are characterised on sonograms as septated, thick-walled, anechoic lesion with mural nodules and cysts. These findings virtually exclude a simple cyst. Septations are uncommon in abscesses or complicated cyst but occur commonly in cystic metastases. Septations, multiple loculations, internal echoes and fluid filled levels have been described in liver metastases (3). Percutaneous cyst aspirations should be considered in indeterminate cases. Aspiration biopsy or surgery is usually required to differentiate metastases from primary biliary neoplasm. Cyst aspiration usually allows differentiation of a cystadenoma from a hematoma, abscess or cyst complicated by haemorrhage or infection. Biliary cystadenomas contain mucinous bile-tinged or brownish cloudy fluid without cells. Cholesterol crystals are detected occasionally (4). However, differentiation from cystadenocarcinoma or solitary cystic metastases may remain difficult. The presence of a solid nodular mass or calcifications along the wall or septa in a multilocular cystic mass indicates a more likely diagnosis of biliary cystadenocarcinoma. Other imaging tests may be useful. Angiographically these tumours are usually hypovascular though abnormal clusters of vessels are frequently seen within their walls. Accumulation of contrast materials within the wall or septum may be seen on delayed imaging (3). Endoscopic retrograde cholangiopancreatography (ERCP) to investigate the cause of jaundice may demonstrate communication of the tumour with the bile ducts. Regardless of the diagnostic modality used, cystadenoma and cystadenocarcinoma cannot be differentiated macroscopically. Resection of cystadenomas is usually curative and since cystadenocarcinomas are beleived to arise from benign cystadenoma, complete surgical resection when possible, is warranted to avoid malignant transformation of these rare tumours. Ultrasound, computed tomography and angiography are the imaging modalities required to evaluate these tumours adequately prior to surgery (2). REFERENCES
Copyright 2002 - Malaysian Journal of Medical Sciences The following images related to this document are available:Photo images[mj02009f1.jpg] |
| |||||||||

{kind=link}