 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
REVIEW ARTICLE Permeability of dentine Farid Bin Che Ghazali School of Health Sciences, Universiti Sains Malaysia, 16150, Kubang Kerian,
Kelantan, Malaysia. Code Number: mj03004 This is an update on the present integrated knowledge regarding dentine permeability that assumed a role in dentine sensitivity and contribute clinically to the effective bonding properties of restorative dental materials. This paper will attempt to refer to in vivo and in vitro studies of dentine permeability and the various interrelated factors governing it. Key words : dentinal tubules, permeability, odontoblast and fluid movement. INTRODUCTION Dentine forms the bulk of the tooth and is perforated by tubules that extend from the pulp to the enamel-dentine or cement-dentine junction. Dentine is a permeable mineralised tissue, which often becomes exposed by disease or restorative procedures. Once exposed the dentine can be very sensitive and any fluid within its tubules can affect the bonding properties of restorative materials. Interest in the permeability of dentine arises partly from the hydrodynamic hypothesis of dentine sensitivity. This hypothesis states that fluid movement occurs within the tubules when dentine is stimulated. The movement is thought to be rapid enough to stimulate nerve endings in the inner parts of the tubules. There is evidence for fluid movement through dentine both in vivo (1, 2) and in vitro (3). The permeability of a material may be defined as its capacity to allow the passage of a solvent or solution through it. The permeability of a membrane to water may be total i.e. all water may pass through. On the other hand solutes in water may or may not be able to pass through depending upon the size of the solute particles with respect to the pore size in the membrane. The term reflection coefficient is used to denote the extent to which solute particles may pass across a membrane and it is assigned a numerical value of 1.0 when no particle may pass across and 0.0 when all such particles may pass through. `The first description of permeation of substances across the dentine was given by Fritsch in 1914' (4). The relationship between differences in the permeability of dentine and its topography has been investigated. The permeability coefficient, which is the opposite of reflection coefficient, measures the ease with which solutes can diffuse across membranes down a chemical gradient in the absence of bulk fluid movement. These terms have been taken from physiology (where the permeability of e.g. capillary membranes is of great interest) and have been extrapolated to research in dentine permeability mostly by Pashley and his colleagues (5, 6, 7). In dentine the permeability coefficient of glucose, sucrose and dextran are all different, because their molecular size and intrinsic diffusibilities are different (6). The permeability coefficient and flow rates vary widely with the highest permeability observed over the regions of the pulp horns and the lowest in the center of the occlusal dentine (7). The density and diameter of the dentinal tubules increases with dentine depth from the EDJ (Enamel dentine junction) to the pulp region. The permeability of dentine is lowest at the EDJ and highest at the pulpal ends. The permeability of dentine has been said to be related to the functional diameter of the dentinal tubules; the greater the functional diameter, the higher the flow rate and thus the rate of permeation. The permeability increases (hydraulic conductivity increases) rapidly as the pulp chamber is approached as permeability of dentine is proportional to the product of tubule numbers and diameter both of which increase as the tubules converge on the pulp (8). Thus the lower permeability of central dentine compared with that over the pulp horn might be due to fewer tubules per unit of the cross sectional area and that central tubules may have smaller diameters because they are further away from the pulp. Each tooth appears to have its own permeability characteristics that differ from other teeth and there are also permeability differences between different age groups (6, 9). Factors that may reduce the permeability of dentine include a) normal appositional growth of intratubular dentine, b) deposition of calcium phosphate crystals e.g. whitlockite in the tubules in the translucent zone ahead of the demineralised areas of caries, sometimes referred to as caries crystals, c) the coagulation of plasma proteins (fibrin) from pulpal blood vessels in the tubules beneath a recently cut cavity (10), d) pathological precipitation of intratubular materials i.e. mineral deposits, collagen fibrils, proteoglycan linings and bacteria and e) the formation of a smear layer of dentine debris on its cut surface during cavity preparation. All these factors can contribute to intratubular occlusion that reduces permeability. Flow in dentine shows similarities to systems of porous media in which flow occurs through an assembly of channels that vary in diameter and shape, and such systems include membranes, plant cell walls, wood and soils. As flow in such systems is complicated by interruptions between the solvents and solutes, so flow in dentine is influenced by the presence of organic material, cellular elements and the residual dentinal fluid. Pashley, (11), has shown that evaporative, thermal and osmotic stimuli applied to the dentine surfaces can induce fluid movement. He postulates that fluid lost is replaced by transudates that arise from pulpal vessels. However, the influence of the odontoblast layer on dentine permeability has effectively been ignored in studies of fluid movement. Information on permeability and its influence on the ultrastructure of the odontoblast layer in humans is lacking. The basic concept of fluid movement in the tubules was proposed long ago (12, 13). A summary of the forces that are thought to affect fluid flow through dentine today include the following: (1) diffusion involving concentration and electrical gradients. (2) filtration flow down a hydrostatic pressure gradient. (3) capillarity forces. (4) evaporation. (5) osmotic pressure. An understanding of dentine permeability depends upon knowledge of fluid flow characteristics under controlled conditions. Among the factors that influence the conditions are the tissue morphology. Although there is considerable information on fluid flow, however only little information has been focused on the morphology related to fluid flow experiments. This present review attempts to address this issue. Dentine permeability studies in vitro. In recent decades efforts have been made to study fluid flow phenomena in detail. In vitro studies on fluid movement provide means of studying diffusion of chemicals through dentine and thus assist the safe undertaking of clinical trials through dentine (14, 15, 16, 17). Brannstrom's significant contributions include studies on whole extracted teeth in which the pulp has been removed and the chamber filled with physiological saline. The crown was either heated or cooled with water and the solution in the chamber moved out of the apex with heat and into the tooth on cooling. It was concluded that heating the tooth induced centripetal fluid movement in the tubules i.e. towards the pulp and centrifugal fluid movement on cooling (18). Anderson, et al., (19) examined the possibility that osmotic stimuli can induce fluid movement through dentine. They placed saturated calcium chloride solution in cavities prepared in extracted teeth and observed that saline placed in the pulp chamber moved towards the cavity preparation. The fluid was observed in a capillary tube attached to the pulp chamber and movement was said to have occurred because the meniscus moved towards the pulp. This was among the early publication attempts to examine the influence of osmotic gradients on fluid movement in dentine. The hydraulic conductance of a tissue expresses the ease in which fluid can move across a unit surface area under a unit pressure per unit time (5). The gradient can be driven by hydrostatic or osmotic forces. The measurement of hydraulic conductance in vitro has provided information about the physical factors governing tubular fluid movements and dentine permeability. The hydraulic conductance of dentine is determined by a number of variables that include the pressure moving fluid across the dentine, the length of the dentinal tubules, the viscosity of the fluid and the radius of the tubules. In 1974 Outhwaite, et al., (20), established their first in vitro method to measure the hydraulic conductance of dentine. The measurements were derived from experiments with a split chamber device that uses slices of coronal dentine of 1 mm thickness from extracted human third molars. These slices were placed on a piece of plexiglass with one end connected to a source of hydrostatic pressure. The other end was used to collect the fluid in order to measure the flow rate. This set-up was then modified (one end of the specimen was acid etched) to study convection and diffusion across dentine with active pressure with the help of a pressure transducer that created a hydrostatic pressure to activate fluid flow. The calculation of the hydraulic conductance (Lp) of dentine was based on a mathematical equation as follows, Lp = Jv /At (P) where
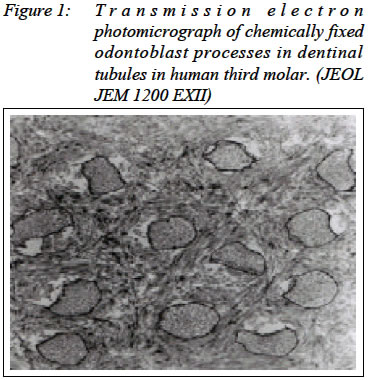
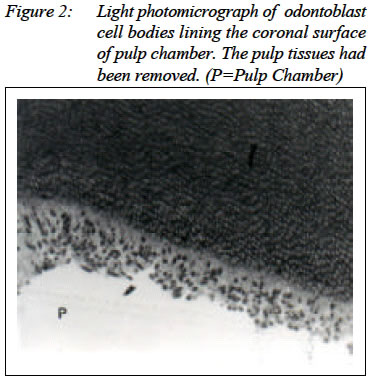
The values for hydraulic conductance (Lp) in various different specimen preparations e.g. cryo preserved, unpreserved and freshly extracted teeth ranged from 1.5 x 10-3 µL.cm-2. min.-1. cm.H2O-1. to 8.97 x 10-3 µL.cm-2. min.-1 .cm.H2O-1. These results have been obtained using a range of hydrostatic pressure gradients (21, 22, 23, 24). Between different research groups there has been little standardisation of hydrostatic pressure and time of application. Pashley and his colleagues (23) have investigated numerous dentine permeability phenomena in extracted teeth and dentine disc preparations. For example they have shown that resistance to fluid movement across crown segments under pressure is composed of three parts, the pulpal resistance, the intratubular resistance and the surface (smear layer) resistance (6). According to this early study the smear layer accounted for 86% of the total resistance (25). The pressure applied across the crown segment in these experiments was high (non- physiological) and a lot of faith was placed in the integrity of the odontoblasts and pulp despite lack of chemical fixation or control of their vitality. In other experiments using dentine discs Pashley, et al., (23), have demonstrated the effects of temperature and acid etching on fluid flow. An increase in temperature of 400 gave a 1.8 fold increase in fluid flow in `unetched' (one side etched) dentine and an increase of 4 fold in dentine that had been etched on both sides. In more recent work Pashley and Matthews, (29) have shown that diffusion of molecules can occur across dentine in the opposite direction to forced convective flow. Physiological studies by Pashley, et al., (23) and other workers (26, 27) did suggest that the hydraulic conductance of the dentine is governed by its biological variability but surprisingly there is yet to be published a proper morphological description of the dentine preparations used. In addition, there are important questions that need to be answered; these include the level of preservation of the tissue and whether it represents the condition in vivo or not. It would also be interesting to study the ultrastructure of the tissue following dentine permeability studies and compare them with non-experimental tissues. Another issue that is also of concern is the permeability of acellular dentine in which all the organic elements have been removed during tissue preparation. Among the methods used to remove the organic components is the maceration technique using 2.5N NaOH aqueous solution (28). Comparison of fluid flow either spontaneous or pressure induced supported by morphological investigation could offer valuable insight into the understanding of dentine permeability. Diffusion or passive transport is the net movement of particles from an area of high concentration within a medium such as water to an area of low concentration due to the random molecular movement of particles. According to Pashley & Matthews (29) diffusion is a relatively slow process across dentine requiring 30-120 minutes depending on the size of the molecules across a thickness of 1-2 mm of dentine. Very little detailed information is available about the diffusion of drugs across dentine. Knowledge of diffusion properties in dentine may be useful for studying the diffusion of drugs across the dentine. For example is it possible for local anesthetics or medicaments to move into the pulp by intratubular diffusion? Diffusion of radionuclides such as 14C-urea, 3H-cortison, 85 Co-hydroxycobalamin and 3H-tetracycline in dentine has been studied using autoradiography (30) and the diffusion of epinephrine and methylene blue through dentine by Bitter (31) and Ciarlone et al., (32). Epinephrine permeability was observed to increase with decreasing thickness of the dentine disc used and increased significantly with the removal of the smear layer. As the investigation of dentine permeability reaches new frontiers, the measurement of dentine permeability becomes more specialised. Hughes, et al., (33) used scanning electro-chemical microscopy (SECM), a relatively new chemical imaging technique that can be use to measure fluid flow across individual dentine tubules. They scanned a microscopic electrode near the surface of a dentine disc in a raster pattern. Potassium ferrocyanide was placed in a chamber below the dentine slab and allowed to diffuse across open dentinal tubules to reach the scanning electrode tip, where it was electrochemically oxidized. After obtaining the baseline diffusional transport rates across dentine they then increased the pressure of the pulpal side of the chamber to 20 cm H2O to induce convective transport of potassium ferrocyanide along with the diffusive transport. They were then able to detect and analyse from images created to localise the fluid flow of individual dentinal tubules. The conclusion is that the fluid flow across that dentine was far from uniform and those dentinal tubules that permitted fluid flow did so at a very high velocity. Other methods of studying dentine using complex mathematics have been introduced. Examples are an impedance technique (34), an electrochemical technique (35), and an alternating current impedance technique (36, 37, 38) but a proper description of the histology of the specimens used is still lacking. Another possible approach to the study of dentine permeability in vitro is to remove the pulp from the odontoblast layer leaving the latter in situ. Evidence that such an approach might be possible is provided in studies by Kramer, (39) and Rockert (40). Chadha and Bishop (41), Ghazali and Bishop (42) showed excellent retention of postmitotic human odontoblasts after pulp removal from third molars. Recently Ghazali and Bishop (43) have improved the technique of pulp removal, as compared to the earlier study with light microscope by Chadha and Bishop (41), odontoblasts with well-defined morphology (cell bodies and cytoplasmic processes) was well retained in the dentinal tubules of third molar crowns following pulp removal. The ultrastructural evidence was documented using transmission electron microscope. JEOL JEM 1200 EXII The results of this study creates possibility of maintaining the viability of odontoblasts retained in situ without the pulp and of investigating the permeability of that layer. Dentine permeability studies in vivo. In, Pashley et al. (44), published study on the hydraulic conductance of dentine in dog teeth in vivo; they applied positive or negative hydrostatic pressures to the exposed dentine of canines and molars. The pressure was applied by means of a conical chamber cemented to the dentine. The base of the chamber was attached to a reservoir of Dulbecco's phosphate buffered saline via a micropipette. Positive pressure was applied when the reservoir was raised above the tooth (up to 240 cm) and negative pressure was applied when the reservoir was lowered beneath the level of the teeth (up to 85 cm below). Fluid movement was observed by the movement of an air bubble within the micropipette. The bubble moved towards the tooth when the pressure was positive and away from the tooth when the pressure was negative. This implies that fluid can move into or out from the dentine and it was the first time that dentinal fluid movement was demonstrated in a live animal. At the same time these workers calculated the hydraulic conductance of the dentine and found that it was significantly higher in the molars than in the canines even though the dentine thickness was comparable. In later experiments it was shown that the smear layer influences permeability of dentine (45). Pashley, et al., (46) then showed that the permeability of dentine in live dogs decreased with time. This was found to be due to the accumulation of inflammatory products including plasma protein and possibly fibrin in the tubules. Next the permeability of dentine in fibrinogen-depleted dogs was shown to be greater than that in which no fibrinogen depletion had been induced (10). Although this work is very significant it also shows that fluid movement has been demonstrated under conditions that seem to be pathological. No attempt seems to have been made by Pashley and his colleagues (44, 45, 46) to examine the morphology of their preparations. Byers, et al., (47), and others (48, 49) have shown that the odontoblasts can easily be disrupted if the dentine is drilled and if deeper preparations into dentine is made the damage could be severe. In the light of the evidence for a permeability barrier consisting of tight junctions between the odontoblasts (50, 51) it is difficult to see how such rapid fluid movement can occur across dentine without its disruption. Another significant contribution to knowledge of dentinal fluid movement has been made by Vongsavan and Matthews (1, 2). Among the most significant findings is the demonstration that fluid pours out of the cut ends of dentine tubules in cat canines (1, 2). They observed under a light microscope the procession of fat droplets in a micropipette that was connected to an exposed dentine surface of an anaesthetized cat. Thus a novel technique for measuring fluid flow across cat dentine in vivo has been devised. This fluid flow has been carefully monitored and its rate has been shown to increase following electrical stimulation of the sensory supply to that tooth and to decrease following sympathetic stimulation. The latter stimulus can also stop the flow or even reverse its direction. In the case of sensory stimulation it seems possible that the axon reflex may be initiated. As such stimulation of the sensory supply electrically in addition to stimulating the nerve endings may stimulate nearby vessels supplied by a branch of the same axon. This use of the axon reflex pathway results in vasodilatation of the vessels involving presumably the production of more vascular transudate all assisting to produce more fluid movement out through the tubules. By observing the movement of lipid droplets in dilute milk solution they established that the resting outward fluid flow is around 13pl/s. The mean flow per tubule is 0.6fl/s, which corresponds to a mean tubular fluid velocity of 1.4 µm/s at the outer dentine surface (1, 2, 52). Vongsavan and Matthews (11) showed that the rate of outward fluid movement in cat dentine in vivo was sufficient to prevent the inward diffusion of Evans blue dye. This study gave evidence that the rate of inward diffusion of chemicals through exposed dentine is affected by the rate of outward flow of fluid through the dentinal tubules. In attempting to test the hydrodynamic theory of dentine sensitivity directly in cats by inducing known fluid flow rates across dentine while simultaneously recording intradental nerve activity, they reported that outward fluid movement activates intradental nerves at lower velocities than inward fluid flow (52). Evaporation of water from dentine. Dentine exposed to air is likely to lose water by evaporation. Air currents or air blasts such as those used clinically are probably effective in evaporating water from dentinal fluid if the humidity of the air is below 100%. The lower the humidity, the higher is the rate of water evaporation. Among the variables involved in evaporative water loss from dentinal fluid are the humidity of air, velocity of air, clinically the distance of an air syringe from a tooth and the temperature of the air (52). In 1993, Matthews and colleagues (53) reported that spontaneous evaporative water loss from dentine in vitro is about 1 µl. cm-2. min.-1, both in the presence or in the absence of a smear layer. It was observed that smear plugs and layers permit water vapour to permeate almost as easily as if they were absent. The smear layer. The smear layer is an aggregation of inorganic and organic substances or debris produced by cutting or burnishing the dentine (53, 54, 55, 56, 57). It is found on the surface of the cut dentine forming a carpet lining which covers the exposed tubules and intratubular zones. The smear layer has been found to be 1-5µm thick and can be identified as a thin white coat in the SEM (58). It adheres tenaciously to the underlying dentine. The presence of the smear layer has been said to have a profound influence on the permeability of dentine (11, 59). Its removal can lead to increases in the rate of fluid permeation across dentine (60, 61). In some cases the presence of the smear layer has been reported to reduce the flow rate to zero (56). It had been shown previously by Stevensson, (62), that grinding the dentine in vitro markedly reduced its permeability. This reduction may have been due to the formation of a smear layer. The permeability of dentine was reported to decrease up to 35% in the presence of the smear layer (25). Other studies by Pashley and colleagues (6, 63), on the permeability of slices of human dentine with and without the smear layer showed that the presence of smear layer on both sides of the discs reduced the rate of transport of 3H20 by 72% and 86% respectively. Hence it was calculated that removal of the smear layer from one side of the disc would produce a decrease in the permeability of dentine by about 40%. Some workers have observed that following cavity preparation a number of the orifices of the cut dentinal tubules contain plugs of dentinal debris, which they called, smear plugs (64). The smear plugs extend varying distances into the dentinal tubules (65, 66) and are usually much longer than the thickness of the smear layer. The use of dilute concentrations of EDTA has been shown to remove the smear layer without removing the smear plug. The smear plug alone can prevent adhesive resin penetration into the dentinal tubules (67). On the other hand if sufficient etching time is permitted, the acid will dissolve both the smear layer and the entire length of the smear plug. While this would permit the penetration of restorative resins into the tubules, it would also permit the outward flow of dentinal fluid that may interfere with the bonding of dental restorative resin to the walls of the tubules. The permeability of normal dentine increases following acid etching (24, 68, 53. 69). However, Kurosaki, et al., (70) demonstrated that the tubules in acid etched excavated carious dentine was occluded by plugs that would make dentine impermeable. Recently Pashley, et al., (71), confirmed that extremely low values for permeability in studies of excavated carious dentine. In normal dentine which has been cut the combination of smear layer and smear plug forms a continuum that is responsible for reducing the permeability of dentine. Bacteria, caries and dentine permeability. Dental caries is a multifactorial tooth disease that results in various mineralisation changes in the tooth structure. There has been intense interest in the permeability of sclerotic and tertiary dentine because it can form beneath carious dentine in a symptom free tooth. Studies with the use of dyes, solvent and radioactive ions have shown that sclerotic dentine production can cause a decrease in the permeability of dentine (72). The presences of caries crystals are also believed to be effective in blocking fluid movement within the tubules (71, 73, 74). Some workers (75, 76) believed that these two types of dentine were permeable but Pashley in 1989 (73), suggested that the presence of sclerotic dentine would enhance the role of dentine as a barrier. The irregular reparative dentine was said to reduce permeability and fluid flow in dentine and thus decrease dentine sensitivity by blocking the pulpal ends of the tubules. Regular secondary dentine on the other hand only affected the permeability by increasing diffusion distances (77). Over the years bacteriological studies have also demonstrated that dentine can act as an effective barrier to bacterial infiltration (64, 78). On an exposed cut surface of dentine, generally it was thought that the presence of a smear layer would prevent microorganisms from invading into the dentinal tubules but these studies have shown that even in its absence, if the microorganisms are able to penetrate into the tubules, their advancement will be halted. The microorganisms have great difficulty penetrating the whole thickness of the dentine due to the varying shape and diversity of the tubules. The physical presence of the microorganisms entrapped within the dentinal tubules is thought to reduce dentine permeability. Trowbridge, (79) suggested that the any entrapped bacteria can interact with the local intratubular dentine. This, Trowbridge believed would result in the formation of caries crystals and sclerotic dentine that would reduce the permeability of that dentine. The permeability properties of the dentinal tubules indicate that functionally they have much smaller dimensions than their actual microscope dimension (5, 74). Although the microscopic diameter of the dentinal tubules at the EDJ has been reported to be 0.5 µm to 0.9 µm; it was suggested that they have a diameter of 0.1µm. To support this, Pashley in 1985 (55) reported that dentine was able to remove 99.8% of a bacterial suspension that had diameters of approximately 0.5µm. Effect of storage medium on permeability. Investigators have used many different types of storage solutions and storage time periods for teeth prior to their permeability studies. Dentine discs or crown preparations have also been stored before permeability experiments were performed. The type of storage medium affects the permeability of dentine in vitro. However there is no standard storage protocol for either whole teeth or prepared specimens. The solutions used for storage have included distilled water (80, 81), formalin (82, 83), ethanol (84, 85) saline solutions (86, 65) and phosphate ringer's buffers solutions (8). Most of the data have not compared the effects of one storage solution to another and therefore it is possible that the results of any one study cannot be compared directly to any other study (87). Salt precipitation has been observed to occur in dentine stored in sodium phosphate buffered saline, which could explain its decrease in permeability over time (46). Elsewhere the decrease in permeability due to type of storage medium used was due to dissolution and redeposition of either mineral or organic components of the dentine into the lumen of the tubules (88, 89). The use of fixatives was reported to give low but consistent permeability values (87). The fact that fixed dentine showed little variation in permeability suggests that the residual material in the tubules such as the odontoblast process and collagen were controlled (preserved). Outhwaite, et al., (8) reported that there was a modest increase in dentine permeability between hour one two days after extraction. No further changes were observed over the following 3-4 weeks. Reeder, et al., (24) used various storage times between 2 days and 1 month in their studies to determine the hydraulic conductance across dentine but did not mention whether the different times of storage had any significant influence on conductance. Goodis, et al., (90) stated that individual specimens have variable permeability in different solutions and thus different solutions affect permeability differently. Pashley and Metthews (29) reported that steam sterilisation did not alter dentine permeability. Apparently neither high nor low temperatures can alter the functional properties of dentine as long as the teeth are intact and dentine is mineralised. (91). On the other hand refrigerated storage with antiseptics modifies dentine permeability by intratubular precipitation of mineral components (92) or organic components such as odontoblast processes, or intratubular collagen fibres (87, 90). In any dentine permeability experiment performed in vitro the variables should be controlled as well as possible. It is quite clear that much work in this field has been done in specimens that have been stored. Conclusion The understanding of the importance morphological role of the odontoblasts and its processes within the dentinal tubules and the tubules physiological characteristics is a structural linked asset to dentine fluid flow and its permeability. Controlled clinical trials should not underestimate this role as a gold standard in clinical trial to effective prompt treatment of dentine hypersensitivity especially with the usage of dentine desensitizing agents. REFERENCES
Copyright 2003 - Malaysian Journal of Medical Sciences The following images related to this document are available:Photo images[mj03004f1.jpg] [mj03004f2.jpg] |
| |||||||||

{kind=link}
{kind=link}