 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
TUBERCULOSIS IN AIDS PATIENTS Veeranoot Nissapatorn, *Christopher Lee, Init Ithoi, Fong Mun Yik, Khairul Anuar Abdullah Department of Parasitology, University of Malaya Medical
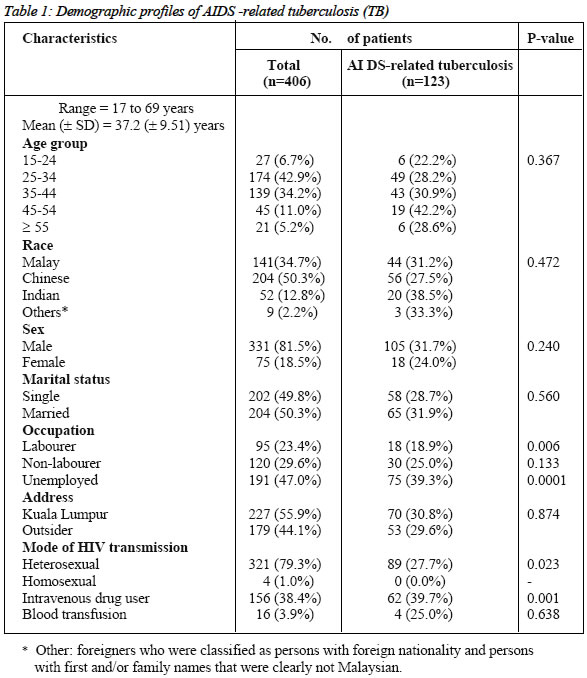
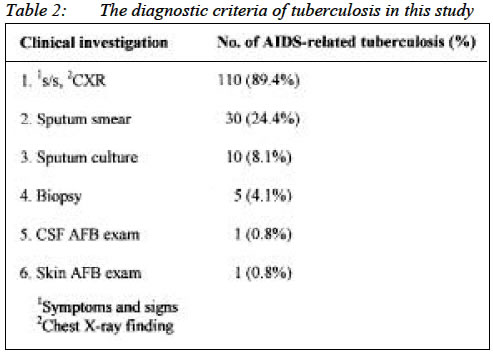
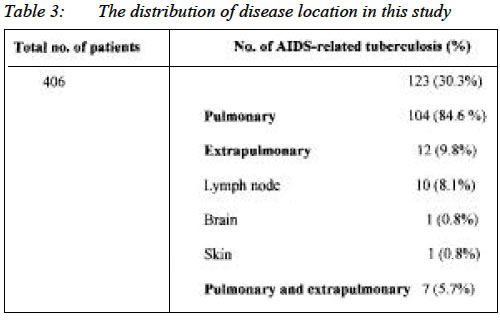
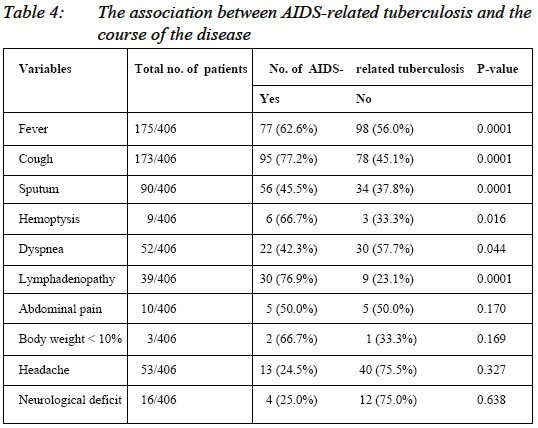
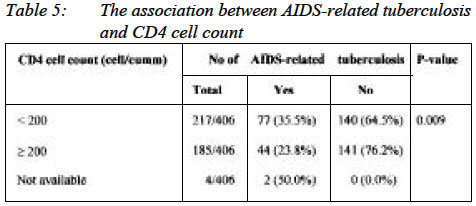
Centre, 50603, Kuala Lumpur, Malaysia. Submitted-11.7.2002, Code Number: mj03009 Tuberculosis is the top agenda among opportunistic diseases and the most leading cause of death in HIV/AIDS patients. A total of 406 AIDS patients were recruited in this retrospective and descriptive study. 123/406 (30.3%) were diagnosed as AIDS-related tuberculosis (TB). Their age range from 17 to 69 years with a mean (±SD) of 37.2 (±9.51. There were significant association between occupation, or mode of HIV transmission and tuberculosis infection (p< 0.05). Pulmonary tuberculosis 104/123 (84.6%) was the most common disease location among TB patients. We found the significant association between the clinical presentations i.e. fever, cough, sputum or hemoptysis and TB patients (p<0.05), moreover, the level of CD4 cell count plays a significant role in association with the disease (p<0.05) in this study. Key words : Tuberculosis, AIDS, Malaysia INTRODUCTION Since the start of the epidemic, issues around HIV and the acquired immunodeficiency syndrome (AIDS) have had a high profile in industrialized countries, however, the burden of disease continues to fall most heavily, and often less visibly, in the developing countries, particularly in Africa (1). Tuberculosis is a disease of great antiquity and it remains a major disease of mankind on a worldwide basis both in term of disease burden and resistance to conventional antibiotic therapy (2). Globally, 9% of all deaths due to TB occur in HIV-infected persons and will be increased to 17% by the year 2000 due to the increasing occurrence of HIV infection in populations already infected with M tuberculosis (3). From this point of view, we conducted the study to determine the frequency distribution of tuberculosis among AIDS patients, and determined the association between demographic profiles, clinical presentations and tuberculosis infection among these patients. The data obtained would guide clinicians to deal with the disease and provide affective management. Materials and methods The retrospective and descriptive study was conducted the Out-Patients Department (OPD) for infectious diseases in Hospital Kuala Lumpur (HKL) which is the largest government tertiary referral hospital, with 81 wards and 2,502 beds. There are about 30 new and 300 follow-up patients with HIV-infection per month that came for medical treatment in this hospital. We examined all medical records of HIV positive patients with various opportunistic infections from January 1994 to April 2001. The inclusion criteria for the study subjects were (1) HIV seropositivity as determined by any serological tests (ELISA (I,II), CLIA or LA) and confirmed by means of Western blot assay according to the 1993 CDC criteria for AIDS diagnosis, (2) patients aged >14 years, and (3) all patients, who were diagnosed as having developed tuberculosis if they fulfilled any one of the following criteria: clinical diagnosis of TB or laboratory tests i.e. CXR, sputum smear positive, culture positive from the sputum or other fluid, histology suggestive of TB that were noted in the patients medical record which were documented in the standardized data collection sheet. Statistical analysis The data was analyzed by using of the statistical software, SPSS. The data for quantitative variables were estimated by median and range while qualitative variables were estimated by frequency and percentage. Statistical analysis was performed using either chi-square test or Fisherís exact test as appropriate. A p-value < 0.05 was regarded as statistically significant. Results Demographic profiles of the study subjects were elaborated in Table 1. The range of age was 17 to 69 years with a mean (± SD) of 37.2 (± 9.51) years. Age group wise, it was found that the preponderant age group was 25 to 34 years (42.9%). The majority of patients were Chinese (50.3%), males (81.5%), married (50.3%), unemployed (47.0%), and city's dwellers (55.9). The most frequent risk behavior to HIV infection was heterosexual. We found the highest significant association between patients with tuberculosis and occupation, or risk behavior to HIV infection (p<0.05). The diagnostic criteria of AIDS-related tuberculosis shownin table 2, was mainly on the basis of clinical symptoms and signs with chest X-ray finding (89.4%) followed by sputum smear (24.4%), sputum culture (8.1%), biopsy (4.1%), CSF AFB exam (0.8%) and skin AFB exam (0.8%) in this study. Tuberculosis made up of 123/406 (30.3%) among AIDS patients in this study. Pulmonary (lung) type 104/123 (84.6%) was the most common disease location, while, lymph node 10/123 (8.1%) was the most common site for extrapulmonary tuberculosis as shown in Table 3. The clinical presentations i.e. fever, cough, sputum, hemoptysis, dyspnea, or lymphadenopathy showed a significant association with tuberculosis infection as illustrated in Table 4. This study showed the study subjects had a mean CD4 cell count of 190.64 cells/cumm (range, 0-881 cells /cumm). However, a significant association was found between patients with tuberculosis and CD4 cell count of less than 200 cells/cumm, as presented in Table 5. DISCUSSION Our demographic data showed that the unemployed and labourers among AIDS patients had a significant association with the risk of developing tuberculosis (p<0.05). It reflects well the real problem of tuberculosis being the most common cause of morbidity and mortality in many parts of the world particularly those developing countries lacking the infrastructures and proper management in dealing with this contagious disease. Moreover, tuberculosis is still a disease of the poor and the low socio-economic background particularly among the developing countries. A significant association was also found between heterosexuals and intravenous drug using with tuberculosis infection. This could explain the concurrence of HIV and tuberculosis infections worldwide. Unfortunately, homosexuals were not taken into consideration either because of it had too small sample size to be compare with tuberculosis infection or it is under-reporting. However, it would be interesting to investigate the socioeconomic risk factors associated with tuberculosis after adjusting for HIV, in different setting. The diagnostic criteria was mainly on the basis of clinical manifestations, chest radiology finding, as a result of therapy in HIV-associated with tuberculosis, we require the urgent need for quick, inexpensive, and precise method which gives a high positive results (4). Therefore, precaution should be seriously taken in the x-ray finding which needs expertise and there is a chance of error in interpretation (5). Confirmation by sputum culture for Mycobacterium tuberculosis, which is the gold standard in diagnosis of tuberculosis and it takes about 4 to 6 weeks for obtaining the outcome, however, is still in use in this study. We found the number of AIDS-related tuberculosis was 123/406(30.3%). This result is much lower than a previous study showed in the prevalence of tuberculosis was 56% (6). In 1990 there were only 6 cases of TB-co-infection with HIV cases reported among the 10,873 TB cases registered. In 1999 the number had escalated to 690 cases or 4.6% of the total number of TB cases (14,908 cases). Cumulatively in the last 9 years TB/HIV cases had contributed about 16.95% of the total TB cases detected in Malaysia (7). However, different studies showed varying figures of tuberculosis i.e. 32% in Brazil (8), 61% in India (9), 18%-28% in Sub-Saharan Africa (1), 31% in Thailand (10). Despite the difficulties in making comparisons due largely to differences in methodology, it is striking that in almost every study from developing regions, tuberculosis is the most frequent identified opportunistic disease (1). Therefore, we suggest screening for tuberculosis infection and disease should be effectively implemented among HIV-positive patients who are living in high risk position in order to curb the incidence of tuberculosis in the future. It is interesting to regard the matter of the significant clinical relevants (fever, cough, sputum, and hemoptysis) with the present of tuberculosis infection (p<0.05) as to be encountered in this study. This finding supports the view that the routine clinical diagnosis of the disease is still largely benefit in tuberculosis case management which we also hope that this co-infection will definitely show less impact in term of public health problem particularly in developing countries. From the present study, we found that patients with tuberculosis infection were associated with CD4 cell count of < 200 cells/cumm. This observation is in agreement with those reported in previous studies (11,12,13). The result indicates that tuberculosis is a useful clinical indicator and one of the most profitable be discussed in the progression of HIV infection with severe immunosuppression or signs of the present of AIDS defining condition. Hence, it is still feasible to monitor CD4 cell count as one of the prognostic markers for HIV/AIDS patients prior to develop more complicated and life-threatening conditions. In conclusion, spectrum of AIDS-related opportunistic infections has been recognized worldwide and it is agreed to the extent that tuberculosis stands on the top list killer disease. From this study is concerned the finding definitely gives us some clues in dealing with tuberculosis in all HIV/AIDS patients. In addition, if all medical personnel are motivated to combat with this challenge, we would be able to expect the incidence of tuberculosis will be remarkedly decreased in the near future. REFERENCES
Copyright 2003 - Malaysian Journal of Medical Sciences The following images related to this document are available:Photo images[mj03009t1.jpg] [mj03009t2.jpg] [mj03009t5.jpg] [mj03009t4.jpg] [mj03009t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}