 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
SUITABILITY OF PARKINSON'S PATIENTS FOR SURGERY IN THE NORTH EAST COAST OF PENINSULAR MALAYSIA: A PROSPECTIVE ANALYSIS J. Abdullah MD, Phd*, M. R. Abdullah MD, Phd**, *Neurosciences Unit, **Department of Community Medicine, School
of Medical Sciences, Universiti Sains Malaysia, 16150 Kubang Kerian, Kelantan,
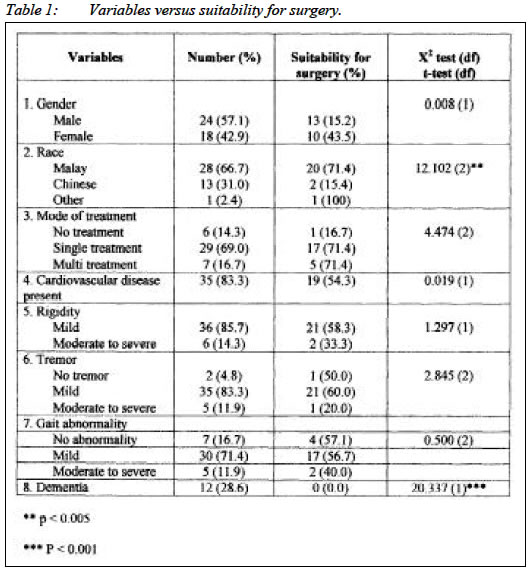
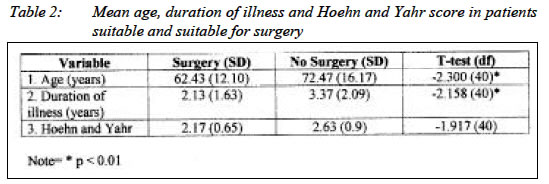
Malaysia. Submitted-6.12.2001, Code Number: mj04011 There is no report in the English literature on the criteria for neuroablation or neuroaugmentation for the treatment of Parkinson's disease in a developing country like Malaysia. A prospective study of patients with Parkinson's disease from the north-eastern peninsular Malaysia was done to assess their suitability of surgery. Age, race, duration of illness and dementia were considered important factors towards the success of such surgical procedures. A mathematical model is suggested for future cases deemed to be suitable for neuroaugmentative or ablative surgery. Key words : Parkinson's disease, Malaysia, prospective analysis, mathematical model, ablative surgery. INTRODUCTION The prevalence of Parkinson's disease in a developed country is estimated to be 19 per 100,000 people (1). As the rate of cardiovascular diseases increases, so will stroke cases as well as cases of Parkinson's disease. There is no published data on Parkinson's disease from the Malaysian population. Neuroablative procedures are those procedures where certain areas in the midbrain are coagulated with low current (2) whereas neuroaugmentative procedures uses an electrode attached to a battery that gives low current for the purpose of negative or positive feedback (3). Neuroablative or neuroaugmentative programme is expensive costing up to RM 60,000 especially for Deep Brain Stimulation (DBS), but may be cost effective if compared, in the long run, to medications. A scoring system was developed prospectively by analysing our patients in order to develop guidelines for our institution prior to augmentative procedures. Objective Our objectives were to determine the proportion of patients and the factors making them suitable for neuroablative or neuroaugmentative procedures in the treatment of Parkinson's disease in the North East of peninsular Malaysia. Materials and Methods All 42 patients registered in the year 2000 were selected from the Hospital Records ICD-9 and follow up prospectively. Univariate and multivariate analyses were done covering various important criteria ie age, sex, medical illness and dementia in the context of clinical assessment for surgery. Suitability for surgery was defined as those patients with rigidity, tremor or bradykinesia and suitable for stereotactic functional neurosurgery which consisted of pallidotomy, thalamotomy (neuroablative) or deep brain stimulation (neuroagmentative) (4). Statistical Analysis Univariate analyses were carried-out to determine the variable associated with the suitability for surgery. The suitability for surgery was assessed clinically by the same neurosurgeon in all cases to avoid variability in the assessment methods and criteria for decision making. Logistic regression & Chi-squared test were performed for categorical variables and independent t-test was used for numerical variables. Multiple logistic regression was used in the multivariate analysis to examine the variable that influenced the suitability for surgery in the study. The gender, age, race, presence of cardiovascular diseases, mode of treatment, severity of rigidity, duration of illness, severity of tremor, gait abnormality, presence of dementia and Hoehn and Yahr score were analysed in all patients to examine their association with the suitability for surgery. Results Forty-two patients with Parkinson's Disease were studied of whom 24 (51.1%) were male. Two thirds (66.7%) were Malays followed by 13 (31.0%) Chinese and 1 (2.4%) Indian. The ages of the patients ranged from 24 to 94 years. The majority of patients (95.2%) had a long history (> 1 year) of illness. Seven (16.7%) patients had a history of cardiovascular disease. At the time of study, 85.7 percent of the patients were on treatment of which 16.7 percent were on more than one drug. Six (14.3%) patients presented with severe rigidity, five (11.9%) with severe tremor and a further five (11.9%) with severe joint abnormality. The Hoehn and Yahr score ranged from 1 to 4 of which the majority (59.5%) had a score of 2. Dementia was one of the most important exclusion criterion for surgery. In this study, 12 (28.6%) patients had dementia. Based on the clinical assessment of the patients in the neurosurgical unit, 23 (54.8%) out of the 42 patients were deemed suitable for surgery. Malay patients were found to be more suitable for surgery compared to Chinese patients (p < 0.05). The mean age of the patients was significantly lower in the patients suitable for surgery (t=-2.300, df=40, p < 0.05). The duration of illness was also significantly shorter in patients deemed suitable for surgery (t=-2.158, df=40, p < 0.05).The rest of the variables did not show significant association with the suitability of Parkinson's patients for surgery. Multivariate Analysis Multivariate analysis was performed to confirm the association detected after the univariate analysis. All the variables, as for univariate analysis, were tested against the independent variable of suitability for surgery. The model showed a good fit and significant improvement in the -2 log likelihood from the initial to the conclusion of the model. Four variables were selected by the model as factors that influenced the suitability for surgery in the studied patients. The younger the age, the more suitable the patients were for surgery. Patients of Chinese ethnicity were found to be less favourable for surgery compared to Malays. Another significant variable included in the model was "the duration of the illness" of which, the longer the advanced illness, the less suitable the patients would be for surgery (5). Dementia had excited a very strong influence on the model. The absence of dementia increased the suitability for surgery > 20 folds compared to if these patients had dementia. The final model is as follows ln Surgery = -0.0479 -0.2498 (age in years) - 4.1969 (Chinese) +8.6007 (other race) -1.0163 (duration of illness in years) + 24.0960 (no dementia). The cut-off point can be calculated based on the model if a mathematical model is required. Otherwise, the model can be used with clinical guidelines to determine the suitability of the patients for surgery. DISCUSSION This prospective study revealed known factors such as age and dementia that determined suitability of patients for surgical intervention. Surprisingly, race and duration of illness were also important factors. Malays were found to be more suitable for surgery than the ethnic Chinese. Those with a short duration history of Parkinson's disease, that is one year or less, were found to be more suitable for surgery. This is also supported by a number of other studies (6-8). Managing diseases like Parkinson's disease can be tedious and complicated, especially when an attending physician or surgeon is required to decide on whether or not to perform an invasive procedure. There are many factors that may decide the outcome of the procedure, and these have to be examined carefully before the decision is made on whether or not to proceed with the invasive procedure. In this study, we look at the relationship and significance of all the variables in determining whether our Parkinson's patients are candidates for surgery or not. For this purpose, multiple logistic regressions were performed to give a provisional working model to predict the suitability of patients for surgery. The word provisional is used as the model is still subjected to global testing on a bigger pool of Parkinson patients instead of to be accepted uncritically (9). A stepwise procedure was used to assess the impact of a variable on the coefficient of the remaining variables and to find the "best fit" of the model (10-11). As shown by the model, dementia is a very strong predictor on whether the patients are suitable for surgical procedures or not. In fact, if dementia is present, the odds will almost definitely be not favourable for surgery, unless the patients are very young. To examine the working example of this model, let us set a situation where dementia is absent and the duration of illness is 2 years. For a 60 years old Chinese and 60 years old Malay, the odds favourable for surgery are 1.040 and 2.7490 respectively. When we lower the age to 50 years, the odds are 1.67 and 2.897 for Chinese and Malay patients respectively. When we raise the age to 70 years, Chinese patients are no longer suitable for surgery, whereas Malay patients still give the odds favourable for surgery of 2.5749. The odds will of course change if we replace the duration of illness with higher or lower figures. In general, the model suggests that for patients with no dementia, we can enter the selected parameters to assess whether the patients are suitable for surgery. The responsible clinician has to decide on the cut-off point for the suitability of a patient for surgical procedures. Conclusion Our observations reveal that age, rase, duration of illness and dementia are important considerations when deciding on the suitability of a patient for neurosurgical procedure. This research also supports other findings that dementia may be an absolute contraindication for surgery (6,12-15). The findings also showed that Chinese patients older than 60 years with 2 years or more of illness may also be another contraindication for surgery. For Malay patients contraindication for surgery in non-demented patients are a combination of age as well as duration of illness but with a definitely higher age and longer duration of illness compared to Chinese patients. However we could not define a cut off point from this study. This would require a larger study group for a conclusion to be made. Reference
Copyright 2003 - Malaysian Journal of Medical Sciences The following images related to this document are available:Photo images[mj03011t1.jpg] [mj03011t2.jpg] |
| |||||||||

{kind=link}
{kind=link}