 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Heterophoria in young adults with emmetropia and myopia Ai Hong Chen, Abdul Aziz Md Dom Jabatan Optometri, Fakulti Sains Kesihatan Bersekutu, Universiti
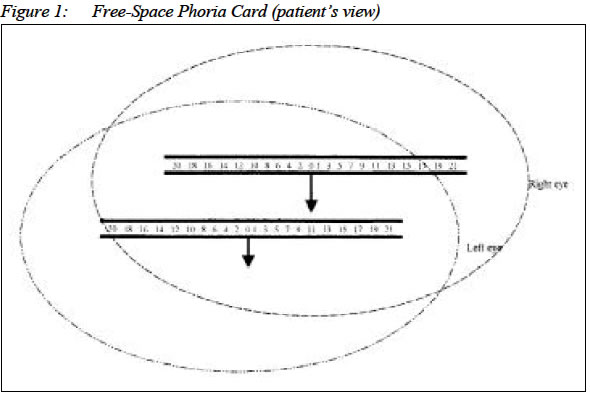
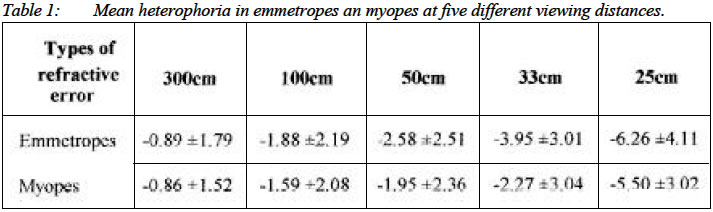
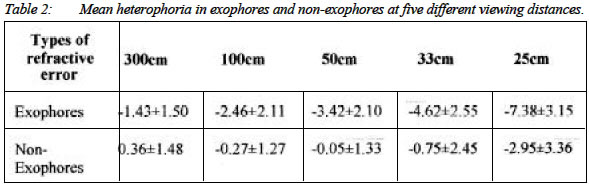
Kebangsaan Malaysia, Jalan Raja Muda Abdul Aziz 50300 Kuala Lumpur Malaysia Submitted-1.4.2002, Code Number: mj03014 The purpose of this study was to investigate the relationship between heterophoria and refractive error. Thirty-six subjects (11 myopes, 25 emmetropes) participated in this study. Heterophoria was measured with the Free-Space Phoria Card at five different viewing distances (25cm, 33cm, 50cm, 100cm and 300cm). Regardless of the types of heterophoria, the amount of heterophoria reduced towards orthophoric position with increasing viewing distance. Emmetropes and myopes did not show any significant difference in the degree of heterophoria at different viewing distances (F = 0.30, p>0.05) or in the type of heterophoria (χ2 = 2, p>0.05). Key words : Heterophoria, myopia, refractive error. INTRODUCTION Heterophoria is the tendency for the two visual axes of the eyes not to be directed towards the point of fixation in the absence of an adequate stimulus to fusion (1). Exophoria and esophoria is the turning of the eye outward and inward respectively from the active position when fusion is suspended (1). Information on the distribution of distance heterophoria and near heterophoria has been well documented in the literature (2-11). There is a high incidence of orthophoria at distance, while most researchers have reported exophoria of about 0 to 6 prism diopters at near viewing distance. Heterophoria seems to vary with different viewing distances. Distance phoria was claimed to be different from tonic vergence due to accommodative divergence (12-14). Distance phoria was predicted by a model (10, 15) that included the subjects' negative accommodation, accommodative vergence and dark vergence {Phoria = dark vergence + (accommodative response - dark focus)(AC/A)}. Emmetropia and myopia are the refractive states of the eye in which, with accommodation relaxed, the images of distant objects are focused on and in front of the retina respectively (1). Heterophoria has been reported to have close association with myopia development (16-19). The nearpoint esophoria has been shown to be associated with childhood myopia progression (16-18). Late-onset myopes displayed higher mean AC/A and dark vergence values and lower mean dark-focus values than the subjects who remained emmetropic (19). The purpose of this study was to investigate the changes in the degree of the heterophoria with varying viewing distances between myopes and emmetropes. Materials and Methods Thirty-six optometry students, aged from 19 to 24 years, participated in this study. All subjects had complete optometric examination within the last two years and did not show any clinical signs of accommodative, fusion, stereopsis or strabismic problems. Written consents were obtained prior to examination. Eleven (8 females, 3 males) of them were myopes (spherical range: -0.25DS to -10.00DS; cylindrical range: -0.25DC to -0.75DC). Twenty-five (14 females, 11 males) of them were emmetropes (Refraction range: plano - +1.00DS). The majority (10 out of 11) of our myopic subjects had early-onset-myopia (onset before 15 years of age). Corrected visual acuity of the subjects was 6/ 6 or better except for two myopes who had a corrected visual acuity of 6/9. Free-Space Phoria Card (20) was used to measure heterophoria in this study (Figure 1). The design of the Free-Space Phoria Card has been reported to have the advantages of providing accommodation accuracy and minimizing fusion. The original Free-Space Phoria Card was modified into five different sizes of the Free-Space Phoria Cards for five different viewing distances so that the numbers, the arrow, and the bar width of each card subtend the same angle (13 minutes of arc) at each testing distance. The acuity size of the optotypes used was 0.95mm, 1.25mm, 1.89mm, 3.78mm, and 11.36mm in height for phoria cards at 25cm, 33cm, 50cm, 100cm and 300cm viewing distances respectively. When a base-down prism (8 prism diopters) was placed in front of the subject's right eye, the line of horizontal numbers on the oval shaped Free-Space Phoria Card became two lines separated vertically. The arrow of the top line would point to numbers on the bottom line that represented the instantaneous heterophoria. The examiner held the testing card for all testing distances to control for the influence of the proximal cue. Since some subjects might exhibit an esophoric shift with sustained fixation (21), alternate occlusion was also incorporated into the technique. Subject was asked to report the position of the top arrow (heterophoria reading) when the occluder was first removed from the right eye. The alternate occlusion was repeated several times (total time involved for each individual was less than 30 seconds) to obtain heterophoria readings when the right eye was first uncovered. The heterophoria of each subject was tested at five different viewing distances: 25cm, 33cm, 50cm, 100cm, and 300cm. Each viewing distance was tested in random sequence immediately one after the other. Two measurements were taken and the average was recorded at each test distance. Binocular fusion was allowed between measurements at different distances. Each subject took less than five minutes to complete the heterophoria measurements for all distances. RESULTS Approximately 24 (69%) subjects had exophoric findings at all distances and only one subject (3%) had purely esophoric findings for all five distances, while the other subjects (28%) had a mix of exophoria and esophoria for the five different testing distances. The remaining eleven subjects, with a mix of exophoria and esophoria, had low esophoria at distance and moderate to high exophoria at near viewing distance except one subject had 2.5 prism diopters esophoria at 25 cm and low exophoria at 33cm, 50cm and 100cm. The mean heterophoria and standard deviation for five different viewing distances in emmetropes and myopes are listed in Table 1. The heterophoria was found to decrease towards an orthophoric position with increasing viewing distance for both emmetropes and myopes. The comparison between myopes and emmetropes was found to be insignificant (F=0.30, P>0.05). However, the variability of the findings appeared to increase for the closer viewing distances because most subjects had heterophoria close to orthophoria at distance but the near heterophoria could be either esophoria or exophoria and the value increased with closer viewing distances. Since the near-point exophoria has been associated with visual stability, where it acts as buffer to the near point stress (22-23), while near-point esophoria is associated with visual deterioration such as faster myopia progression (16-18), the findings from the present study were further analyzed by dividing the subjects into two study groups: exophores (only exophoria findings for all distances) and non-exophores (a mix of esophoria and exophoria or purely esophoria). The mean heterophoria and standard deviation are shown in Table 2. There was a significant difference in the heterophoria findings between exophores and non-exophores (F=7.04, p<0.05). Approximately 72% of emmetropes were exophores, and 28% were non-exophores. Meanwhile about 64% of myopes were exophores and 36% were non-exophores. There was no significant difference in the distribution of exophores and non-exophores between myopes and emmetropes (χ2= 2.00, p>0.05). When the heterophoria was plotted against viewing distance in centimeters, the heterophoria was found to change logarithmically with viewing distance. If the viewing distance was plotted in diopters instead of centimeters, the graphs become linear with negative slopes. The mean heterophoria changes with different dioptric viewing distance are plotted in Figure 2 for exophores and Figure 3 for non-exophores. Linear regression equations are listed as follow: Exophores : y = -1.51x - 0.74 (R2=0.95) Non-exophores : y = -0.71x - 1.40 (R2=0.74) where x is the dioptric distance in diopter and y is the heterophoria in prism diopter. The rate of change in heterophoria for exophores (1.5) was almost double compared with non-exophores (0.7), but the comparison of the two regression lines was found to be insignificant (t=-0.14, df = 32, p>0.05). Discussions In general, exophores (69%) were most common in this study. Regardless of the type of heterophoria, the amount of heterophoria decreased towards orthophoric position with increasing viewing distances. Our finding are also consistent with the report of fixation disparity at different viewing distance (24). Jaschinski reported an exo-shift of fixation disparity from 60cm (approximately 0.25 min arc fixation disparity) to 30 cm (approximately 2.5 min arc fixation disparity) of viewing distance. We too report an exo-shift of the heterophoria with decreasing viewing distance in 97% of our subjects. One subject however showed an eso-shift for closer distance. Although near-point exophoria has been associated with visual stability, where it acts as a buffer to the near point stress to preserve emmetropization (22-23), and near-point esophoria with visual deterioration such as faster myopia progression (16-18), our finding did not show any significant difference between myopes (early onset myopia) and emmetropes in the type or the degree of heterophoria for all testing distances. However, further investigations of the heterophoria at different distances in young progressive myopes might reveal different results. Meanwhile, hyperopia and exophoria had been described as buffers for emmetropization (22), where the absorption of both hyperopia and exophoria might be an early sign of near-point stress-induced vision disorder or myopia progression. A further study to compare the heterophoria changes with viewing distances between symptomatic and asymptomatic patients might be useful. There is a possible different pattern of heterophoria changes with viewing distances between symptomatic and asymptomatic patients because symptomatic and asymptomatic subjects (eg: asthenopia) had been reported to behave differently in tonic adaptation (25) and in transient myopic shift performance (26). This additional information on the changing pattern of heterophoria with viewing distance might be useful in the diagnosis and management of non-strabismic binocular problems (27) such as divergent excess, convergence weakness and so on. ACKNOWLEDGEMENT This study was supported by UKM research grant (NTGO/22/98). REFERENCES
Copyright 2003 - Malaysian Journal of Medical Sciences The following images related to this document are available:Photo images[mj03014f1.jpg] [mj03014t1.jpg] [mj03014t2.jpg] [mj03014f3.jpg] [mj03014f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}