 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
CASE REPORT UNILATERAL EXOPHTHALMOS CAUSED BY AN EXTRAMEDULLARY PLASMACYTOMA : A CASE REPORT M. Ashraf, J.Abdullah, AR Ariff, Biswal B. M*, Mokhtar I**, NH Othman*** Neuroscience Unit, Radiotherapy and Oncology, *Department
of Nuclear Medicine, **Department of Ophthalmology, ***Department
of Pathology, Hospital Universiti Sains Malaysia, 16150 Kubang Kerian, Kelantan.
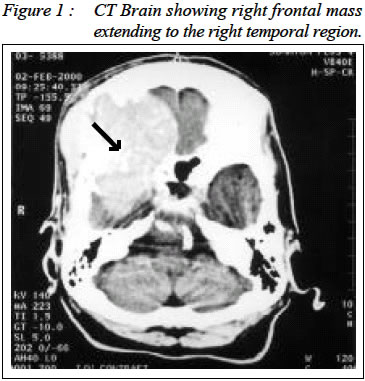
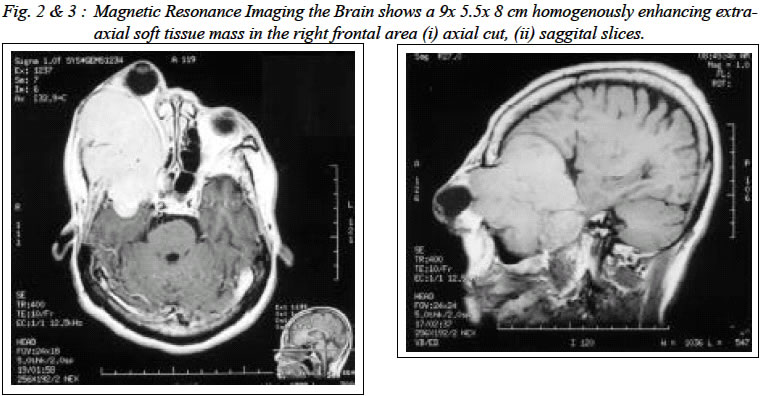
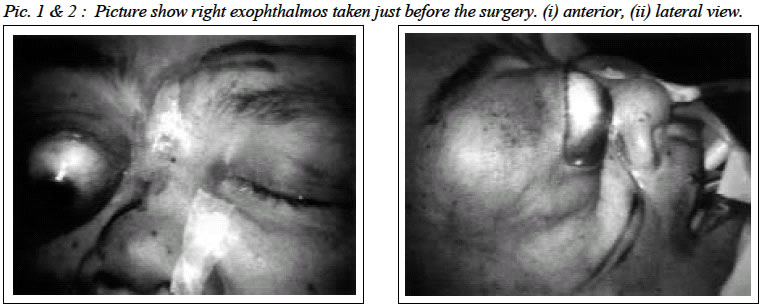
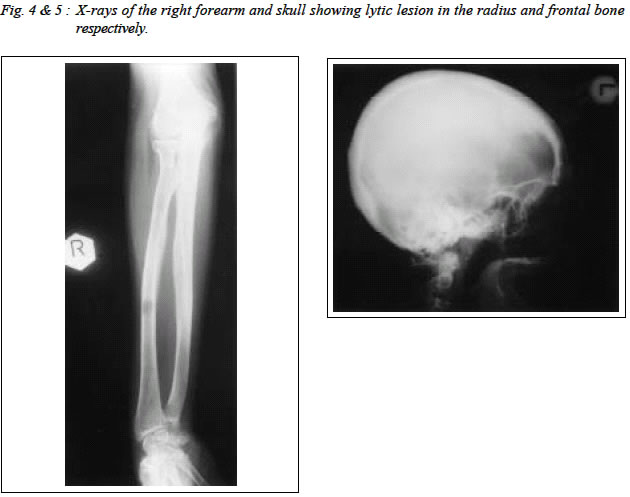
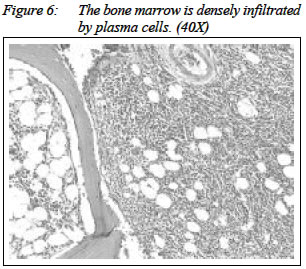
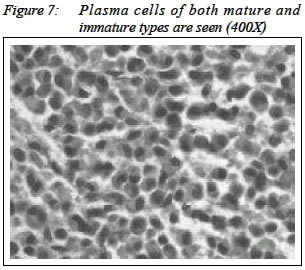
Malaysia. Submitted-10.10.2001, Code Number: mj03015 Solitary plasmacytoma of the head and neck is a rare disease entity. Its description in the literature consist of some case reports. Solitary plasmacytoma presenting with exophthalmos are rare. We report a case of intracranial solitary plasmacytoma in an elderly lady with involvement of the right orbitocranial region presenting with severe exophthalmos. The tumour was debulked and radiotherapy was given. Key words : Solitary plasmacytoma, Orbitocranial, Management. INTRODUCTION Head and neck solitary plasmacytoma is a rare disease entity. It is a part of a spectrum of plasma cell tumour ranging from benign solitary plasmacytoma to malignant cell plasma leukaemia with multiple myeloma in the middle. Its description in the literature consist of some case reports (1). It is usually considered to be the diagnosis in cases where only one plasma cell tumour is found. To date, there are only 2 series reported by Bindall et. al of 8 cases(2) and by Byram et. al of 6 cases(1). Solitary plasmacytoma can occur in soft tissues (or known as extramedullary) and in bones. Solitary intracranial plasmacytoma, which is the most appropriate term used for the above case, can affect the meninges, skull and cerebral tissue. The commonest sites for plasmacytoma of the bones are spine and long bones of arms and legs which usually present with pain and the tenderness at the sites of the lesions. A less common site is the skull bone. In the soft tissues, it commonly occurs in the nasal cavity, nasopharynx and paranasal sinuses, which commonly presents with dysphagia, but it can also occur in the gut, the central nervous system, bladder, thyroid gland, breast, testes, parotid (salivary) glands and in the lymph nodes. The risk factors for solitary plasmacytoma are the same as for myeloma, which is nearly always a disorder of the middle aged or elderly. These disease are not found in childhood or adolescense and are, in fact, very rare below the age of 30. Our case falls in the appropriate age group. CASE REPORT A sixty seven year old Malay lady presented to Hospital Universiti Sains Malaysia for one year duration progressive proptosis of the right eyeball. This swelling was associated with severe right frontal headache. She was initially diagnosed clinically to have meningioma of the right orbit 5 years ago. The CT scan of the brain (Figure 1) at that time showed an enhancing homogenous soft tissue mass involving the maxilla, sphenoid, ethmoidal sinuses and frontal bone with the presence of dural tail. When the patient presented to us two years later she appeared well with an obvious right eye exophthalmos with third, fourth and sixth cranial nerve palsies. The was no perception to light. Blood pressure was 160/95 mm/Hg. There was no other neurological deficit. The other systems revealed no evidence of haematological disease. The provisional diagnosis of meningioma of the right sphenoid wing was made as evidenced by Magnetic Resonance Imaging of the brain and orbit (figure 2 & 3). Four vessel cerebral angiogram revealed a hypervascular tumour. In view of the radiological diagnosis of meningioma surgical excision was planned. She underwent debulking of the tumour including right eye enucleation. There was no immediate post-operative complication. Intraoperative finding showed a solid tumour in the right anterior cranial fossa displacing frontal lobe posteriorly. The tumour involved the frontal skull bone, orbital wall and dura mater. Skeletal survey noted the presence of lytic lesions in the frontal bone (where the tumour was situated preoperatively), occipital bone and right radius (figure 4 and 5). 99m-Tc MDP bone scan revealed increase tracer uptake at the right frontal bone, right elbow and tip of the mandible. Preoperative blood investigations were normal except for high serum creatinine of 266 mmol/l and serum calcium of 2.41 mmol/l. The histopathological examination showed plasmacytoma (Figure 6 & 7) of lambda light restriction. Postoperatively urine Bence Jones test was positive. 24-hour urine protein was 5.4 g/day. Immunofixation test disclosed abnormal band with faint lambda light chain but no heavy chain. Serum immunoglobulins revealed high level of IgM, 4.65 (1.2-3)g/l with normal IgG and IgA, 12.56 (8-16) g/l and 1.19 (0.99-2.2)g/l respectively with the presence of paraprotein of 2.5 g/l. Serum and urine electrophoresis were normal. The patient underwent radical radiotherapy, 50 Gy in 25 fractions over 5 weeks, delivered to the affected cranium using a 6 MV linear accelerator. The course of post-operative radiotherapy was uneventful, subsequently she was on regular follow up. DISCUSSION Exophthalmos is a very rare presenting sign of solitary plasmacytoma(1). Bayram et. al reported 2 cases which presented with exophthalmos as initial diagnosis(1). Our patient had right eye blindness and exophthalmos. Presentation depends on the location of the lesion. Lesions of the convexity present themselves as a mass lesion much like the 3 cases of parietal mass as noted by Bayram et.al in their series (1). Bindall et. al reported that lesions infiltrating the skull base were not likely to be solitary, and the patients who harbor these neoplasm should undergo complete evaluation to exclude multiple myeloma (2). However, cases involving cranial base in the series of Bayram et. al did not reveal multiple myeloma after close and extensive screening(1). Minoru et. al have strict definition of `solitary' plasmacytoma, which is radiologically solitary bone lesion, neoplastic plasma cells in the biopsy specimen, fewer than 5% plasma cells in bone marrow, less than 2.0 g/dl monoclonal protein in the serum when present and negative urine test for Bence Jones protein (monoclonal light chain)(6). The above patient had positive Bence Jones protein in the urine, either spot test or 24 hour urine collection, multiple lytic bone lesions and no bone marrow specimen obtained contradicting the criteria given by Minoru et. al. However, Woodrof et.al defined solitary plasmacytoma of the bones as presence of solitary osteolytic lesion without evidence of multiple myeloma on bone marrow examination(8). Unfortunately, our patient refused the invasive investigations and furthermore she also has more than one osteolytic lesion though we cannot certify that the lesions occur simultaneously or part of metastases. To diagnose solitary plasmacytoma is sometimes difficult. The X-ray and laboratory findings in a case of plasmacytoma of the bone are very similarly to those multiple myeloma. The most important step in management is for investigations to confirm that there is only one tumour present. Bone marrow involvement in multiple myeloma is patchy and the specimen may be taken for a region not involved with the disease. Skeletal survey is also insufficient for the precise diagnosis of solitary bone plasmacytoma. The presence of lytic lesion in the occipital bone and right radius in our case may indicate metastasis rather than diagnosis of bone plasmacytoma as shown in the right frontal bone. A recent report by Moupoulus et. al (9) indicated that magnetic resonance imaging showing additional bone abnormalities which had not been detected by standard skeletal survey in some patients with a diagnosis of solitary bone plasmacytoma. The MRI to exclude other bony lesion was not done in this patient. The above patient had high level of IgA with normal level of other immunoglobulin groups i.e. demonstrating a monoclonal gammopathy (M component). However, serum and urine electrophoresis was reported as unremarkable. Solitary plasmacytoma is thought to be a kind of monoclonal gammopathy(3) but Woodrof et. al stated that presence of M band on serum electrophoresis is not so important. Intracranial plasmacytoma is very radiosensitive(8). Some authors advocate curative radiotherapy following biopsy or partial resection. Arienta et. al (11) reported cure with complete resection without radiotherapy. High local control rates reported with radiotherapy, although the optimum dose and extent of radiotherapy portals remain controversial(7). Our patient was subjected to a tumour dose of 50 Gy same as median radiation dose (range between 30-70 Gy) used by Liebross et. al(4) who reported local control of 96%. Byram et.al also used 50 Gy. Dimopoulus et. al(10) reported less than 10% recurrence rate. However, surgical removal followed by postoperative irradiation is the treatment of choice(2). Experience by Bayram et.al(1) revealed that total resection combined with radiotherapy may not achieve a complete cure in every patient hence larger series are needed to support this statement. The efficacy of chemotherapy is not certain. Shih et. al(12) failed to find any benefit on the outcome of patient who received chemotherapy. Bayram et.al use chemotherapy for patients with partially resected tumour and who had bone involvement. The outcome depends very much on the primary site of origin. If it occurs in soft tissues then the outcome is good. The histopathological examination of the tumour in this patient could not identify the tumour's primary tissue origin. It is either from the soft tissue infiltrating into the skull bone or in the opposite direction. There may be recurrence of plasmacytoma. About 50% of patients with solitary plasmacytoma progressed to multiple myeloma after treatment(1,4,10). The amount of M-protein after radiotherapy was a predictor of subsequent development of multiple myeloma(4,10). Therefore, with the cure of solitary plasmacytoma, a drop in the level of immunoglobulin in serum or cerebrospinal fluid is expected and it can be used as a tumour marker to detect the recurrence. From the literature review, besides persistent presence of myeloma protein, cases with infiltration of cranial base are similar to plasmacytoma of the spine and carry high risk of progression to multiple myeloma over long term follow up.(13) Solitary plasmacytoma of bone tends to disseminate or progress to multiple myeloma even as long as 7-23 years after presentation(6). In conclusion, solitary intracranial plasmacytoma continues to be a problem in neurosurgery. There is no specific pattern of presentation. It is very important to exclude multiple myeloma as the management bastly different. At the moment, radiotherapy has an important role in the treatment of solitary plasmacytoma. Further study with larger series may be helpful in identifiying patients who are likely to progress to multiple myeloma. ACKNOWLEDGEMENTS This case report was written as part of the corresponding author's fulfilment during his six month posting in neurosurgery for the Master of Surgery (usm) in the first six months of 2000. REFERENCES
Copyright 2003 - Malaysian Journal of Medical Sciences The following images related to this document are available:Photo images[mj03015f4-5.jpg] [mj03015f6.jpg] [mj03015p1-2.jpg] [mj03015f7.jpg] [mj03015f1.jpg] [mj03015f2-3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}